


1. Introduction
Glasser and Lerner-Geva reported a prevalence of perinatal paternal depression ranging from 2.3-8.4% in the meta-analysis [2]. In Japan, Takehara reported a prevalence of depression among 9.7% of fathers, at 20 weeks of gestation in Aichi Prefecture [3]; in a similar regional study, Suto et al. reported a prevalence of 17% during pregnancy [4]. Additionally, Konishi et al. reported that the prevalence of prenatal depression among fathers with pregnant partners was between 3.7% and 10.3% [5]. Whereas these studies were conducted in a particular region of Japan, Kido et al. found, from a nationwide web-based survey, that 31.3% (95% CI: 27.3-35.7%) of men with pregnant partners suffered from prenatal depression [6]. They also reported prevalence rates in different areas of Japan; Chugoku region (it consists of five prefectures (Tottori, Shimane, Okayama, Hiroshima and Yamaguchi) in the most western part of mainland in Japan) having the highest score out of any region with a median Edinburgh Postnatal Depression Scale (EPDS) of 11. The EPDS used in Kido et al.’s study considered a cut-off score of 13 points or more. It was assumed that EPDS scores were generally higher in the Chugoku region, although the proportion of scores above 13 was small [6].
Whereas previous assessments of perinatal paternal depression have used the EPDS, the scale was developed for mothers [7]. As the nature of depressive symptoms in men has been reported to be different from those in women [8], questions have been raised about the reliability of the EPDS as a measure of perinatal depression in fathers [9]. Alternative to the EPDS as an instrument for perinatal depression in fathers, there are studies using the Patient Health Questionnaire-9 (PHQ-9) as a general depression screening scale [5].
As part of its efforts to decrease in number of the childbirth, the Ministry of Health, Labour and Welfare (MHLW) of Japan has been encouraging fathers to avail of childcare leave. Starting April 2022, the Act on Childcare Leave, Caregiver Leave, and Other Measures for the Welfare of Workers Caring for Children or Other Family Members will be amended to allow men four weeks of postnatal leave, out of the eight weeks they are entitled to after their partner delivers a baby [10]. This implies that fathers’ involvement in childcare is being increasingly encouraged nationally; the prevalence of perinatal paternal depression may rise as a result of this new policy.
Untreated paternal depression occurring during the perinatal period has been reported to increase the risk of specific mental disorders among school-aged children, twice as significantly. In Japan, Nishigori et al. reported on paternal perinatal depression and child attachment [11]. Postnatal depression in mothers has been identified as an issue that required addressing in Japan, mothers has been approached with a questionnaire to assess their feelings towards their babies using the Japanese version of the Mother-Infant Bonding Scale (MIBS-J) [12]. Because, perinatal depression can be associated with negative feelings towards baby, which increase the potential risk of neglect or abuse of the baby in both mother and father [12]. Postnatal depression in mothers was identified as an issue that required addressing in Japan, mothers were approached with a questionnaire to assess their feelings towards their babies using the Japanese version of the Mother-Infant Bonding Scale (MIBS-J) [12]. Although the scale have been used to assess mothers during their pregnancy, no studies have been reported that assess fathers during their partners’ pregnancy. Paternal depression should be treated as a crucial problem that negatively impact children’s mental health and thus, requires urgent intervention [13].
This study aimed to investigate paternal depression occurring during a partner’s pregnancy in the Chugoku region of Japan, as well as to examine the factors associated with paternal depression and its possible relevance to attachment with the child. In this study, instead of the EPDS, a general depression scale was used to assess perinatal paternal depression. The findings of this study provide a basis for considering interventions for perinatal paternal depression.
2. Methods
2.1 Study design
This cross-sectional study examined the prevalence of depression and associated factors among men whose partners were pregnant in a rural area, Chugoku region, in Japan.
2.2 Measurement for paternal depression
The PHQ-9 [14] was used to assess depression in men. The PHQ- 9, which has previously been reported to be available for screening the prevalence of perinatal depression in men, used in this study [5]. The PHQ-9 comprises a nine-item scale to assess depression levels. The symptom assessment was based on the existence of symptoms for each question within a week, with the score distributed as follows: never: 0 points, a few days: 1 point, more than half of the week: 2 points, and almost every day: 3 points. The total score (0-27 points) was calculated. It also assesses depressive severity, based on the total score of questions 1 to 9: 0-4: normal to minor; 5-9: mild; 10-14: moderate; 15-19: moderate to severe; and 20-27: severe.
2.3 The risk factors associated with perinatal depression for fathers
The following sociodemographic details and main background factors, considered from previous studies on paternal depression, were collected: number of children; unexpected pregnancy; own (partner’s) mental health history; family bereavement as a life event; health status of children; and economic status [15-17]. Additionally, the questionnaire asked about marital status, occupational stress, occupational satisfaction, and feelings toward the child that affect men’s perinatal depression. The questions on the marital relationship consisted of the following six items: “building trust in each other,” “mutual understanding,” “spending enough time as a couple,” “having many conversations as a couple,” “respecting some hobbies and activities,” and “doing my best at parenting and housework”. All of these were examined using a four-point Likert scale ranging from “I don't feel it at all” to “I always feel it strongly.” The questions on occupational stress consisted of the following 11 items: “Excessive responsibility,” “no one talks with me at work,” “long working hours,” “not suited to the job,” “difficulty coping with information technology and innovation,” “uncertainty about the future of the company,” “fear of redundancy or bankruptcy,” “excessive emphasis on work performance,” “heavy workload,” “uncomfortable working environment,” “difficult working relationships' uncomfortable working environment”, “difficulties in interpersonal relations at work”. All of these were examined on a four-point Likert scale, ranging from “I don't feel at all” to “I always feel strongly.” A high score indicates lower stress at work, and a lower score indicates a better relationship with the spouse. Occupational satisfaction is constructed from the following seven items: “Salary and wages,” “amount of week off and holiday,” “work contents,” “discretion of the work,” “evaluation and compensation,”“work/ life balance,” and “the amount of paperwork to take home”. All of these were examined on a five-point Likert scale, ranging from “I completely satisfied” to “I totally dissatisfied”. A lower score indicates a higher level of job satisfaction. The Japanese version of Mother to Infant Bonding Scale (MIBS-J) [12] was used to question the feelings towards their baby. It consists of 10 items, rated on a scale of 0 to 3, with higher scores indicating stronger negative feelings toward the baby. The scale assesses attachment and rejection/anger toward the baby
2.4 Sample size
The number of births per year in the rural area was calculated to be approximately 8,000 (year 2021), with a confidence level of 90%, a tolerability of 10%, and a response ratio of 0.5, resulting in a sample size of 67.
2.5 Subjects, procedures, and the exclusion criteria
The participants were 64 men whose partners were in their third trimester of pregnancy. All data were obtained from the male partners of pregnant women who visited the obstetrics and gynecology department of a general hospital in a regional city (population 140,000) in Japan. Participation in the study was voluntary. In terms of exclusion criteria, foreign nationals living in Japan were excluded because their language skills may not allow them to fully understand the questions.
2.6 Analysis methods
Descriptive statistics were calculated and subsequently analyzed by bivariate and multivariate statistical analysis using IBM SPSS® Statistics version 24.0 and EZR [1], with P-value <0.05, considered statistically significant. Also, the PHQ-9 cut-off were used to compare the two groups, PHQ-9 <4 (non-depression group) and PHQ-9 >4 (depression group).
2.7 Ethical considerations
A midwife working in the Department of Obstetrics and Gynecology of the General Hospital explained the significance, purpose, and methods of the study to the participants. It was also explained that refusal to participate would not affect them in any way. In addition, the privacy of the respondents was protected by asking them to complete the questionnaire anonymously to prevent the researcher from identifying them. The study was approved by the Ethical Committee of the Kagawa Prefectural University of Health Sciences (approval number 274) and the Ethical Review Boards of the hospitals where the data were collected (approval number K402- 20210203).
3. Results
3.1 Depression and feelings about the baby (Table 1)
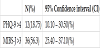
The prevalence of perinatal paternal depression and the negative feelings towards baby were showed Table 1. Twelve participants (18.75%, 95% CI: 10.1-30.5%) had greater than mild depression on the PHQ-9. Thirty-six (56.3%, 95% CI: 25.40 - 37.10%) had an MIBS-J score of >3.
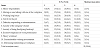
Demographics of the participants showed Table 2. Sixty-four fathers completed the survey although 67 were invited to participate (the valid responses were 95.5%). The demographics of the fathers were compared between two groups: PHQ-9 <4 (non-depression group) and PHQ-9 >4 (depression group). PHQ-- >4 (depression group) were significantly more frequently reported poor about health status of the child.

3.2 Occupational stress, satisfaction, and marital relationships
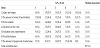
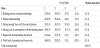
The level of occupational stress of the subjects is shown in Table 3, and satisfaction with their work is shown in Table 4. The marital status of couples is shown in Table 5.
3.3 Depression-related factors
The results of the Mann-Whitney U test showed significant differences in the scores of occupational stress and marital relationship in the results of the comparison between the depressionand nondepression groups (Table 6). The depression group had significantly higher occupational stress, and marital relationships were also poor.
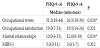
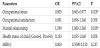
The factors associated with depression with significant odds ratios (OR) were occupational stress and marital status (Table 7).
4. Discussion
4.1 The prevalence of paternal depression
In Japan, depression among fathers during their spouse’s pregnancy has been reported to be between 3.7% and 31.3% [3-6]. In the present study, 12 men showed depressive symptoms when their partners’ pregnancy was identified (PHQ-9 >4= 18.75%, 95% CI: 10.1-30.5%). In this study, the PHQ-9 was used to assess perinatal depression in fathers. In a rural area of Japan, it was revealed that less than 20% of men show depressive symptoms during the perinatal period of their partners in this study. In a meta-analysis, Tokumitsu et al. reported that the prevalence of depression during pregnancy among Japanese women was 14.0% in the second trimester and 16.3% in the third trimester [18]. This highlights the need for the assessment of the mental health status of the father and the mother throughout the pregnancy. Mothers are required to receive regular prenatal examinations to ensure their mental health status and appropriate interventions; however, there is no such obligation for the fathers; therefore, their mental health conditions are less likely to be identified.
The EPDS has been used as a measure to assess perinatal depression in mothers; however, as mentioned above, it has been pointed out that the EPDS inadequately covers the depressive symptoms experienced by men. For instance, Massoudi et al. identified different factors of perinatal depression - worry, anxiety, and unhappiness - that were more frequently observed in fathers than in mothers [8]. Psouni et al. questioned the validity of the EPDS for men and attempted to develop a perinatal paternal depression scale [9]. Further research needs to be conducted in using or developing a scale that can assess specific perinatal depressive symptoms in fathers.
4.2 Factors associated with perinatal paternal depression
This study found that high occupational stress was one of the main factors associated with depression among perinatal fathers. In comparison with the normal group, men with PHQ-9 > 4 had a median of eight working hours; in other words, they were not overworked. The occupational stress scale provides an assessment of work responsibilities, workload, and relationships at work. For men, feeling overburdened at work and having a poor working environment can affect their mental health. However, the association between having a baby and stress at work could not be confirmed.
Marital relationships have also been associated with paternal depression. In a couple in a bad relationship, the birth of a child may lead to poor parenting responsibilities; furthermore, if one of them undertakes a higher amount of burden than the other, the parenting environment may deteriorate. Thus, interventions to improve a couple’s relationship are necessary, as poor parenting environment can have a negative impact on the child’s development [13]. However, it is extremely difficult for health professionals to grasp the participants’ marital relationships. It remains to be explored how and who assesses the couple's relationship and intervenes accordingly.
4.3 Fathers’ bonding with the child
The MIBS-J has been validated by Yoshida et al. as an instrument for assessing the attachment of postpartum mothers to their children [12]. Whereas there is no cut-off score for MIBS-J, scores >3 indicate the need to be alert for the possibility of child abuse or neglect. However, research on the use of the MIBS-J as an instrument to assess fathers’ attachment to their children during partners’ pregnancy is lacking. Thus revealing that the majority of fathers (56.3%, 95% CI: 25.40 - 37.10%) had an MIBS-J score of >3, during their partner’s pregnancy. Kitamura et al. found that failure of bonding with the child after delivery predicts maltreatment in mothers. Similarly, for fathers, their feelings toward their children may negatively affect their attitudes toward parenting in cases where the bonding with the child has not been well developed [19]. Whereas maternal bonding with the child occurs before childbirth, it remains unclear when the father’s bonding with his child starts to emerge. To prevent maltreatment of the children by fathers, it is necessary to intervene from the period of pregnancy to develop and ensure father’s bonding with the child. However, there is no opportunity to assess the father’s feelings towards the child during the partner’s pregnancy; therefore, it is essential to explore this aspect in further research.
5. Conclusion
In the Chugoku region of Japan, prevalence of depression among fathers whose partners were pregnant was similar to the prevalence in mothers. However, the specific factors associated with depression in men appeared to be occupational stress, marital relationships, and the health status of the child. However, this study has certain limitations, in that it was conducted in one rural area. Additional data need to be collected to ensure the reliability of the findings.
Competing Interests
The authors declare that they have no competing interests.
Author Contributions
Mitani A and Kido K contributed to the idea of the study design, data analysis and drafting the manuscript. Mayumi Ono and Junko Maeda collected and analyzed the data. All authors read and agreed on the final manuscript.