


1. Background/Introduction
Type 2 diabetes mellitus (DM) has been increasing worldwide and Vietnam is not an exception [5,6]. During the last decade, along with rapid economic growth and urbanization, the Vietnamese lifestyle and dietary habits have changed [9]. There are studies suggesting that the risk factors for DM in Vietnam are high intake of white rice, abdominal fat, and a sedentary lifestyle [2-4,7].
Worldwide, the BMIs of type 2 DM patients are usually high (>25 kg/ m2) [13] but some studies have reported that the BMI of Vietnamese DM is usually not high (<25 kg/m2) [2,4,7]. According to a previous study, Taiwan and Vietnam are located in the same region (Asia); however, there are differences in the BMIs of newly diagnosed type 2 DM patients in the two countries (Taiwanese 26 and Vietnamese 23) [2]. In addition, Vietnam has recently been facing the problem of Nutrition Transition, including changing dietary patterns, different meal structure such as increasing meat and fat, and decreasing vegetable consumption [9]. Therefore, we think that dietary factors may be more important than genetic factors.
Although it is a fact that drug therapy is mandatory for most type 2 DM patients, dietary treatment is essential in diabetes management. Meta-analysis studies have shown that increasing dietary fiber intake in patients with type 2 DM decreases HbA1c and fasting plasma glucose levels [11,12]. Nhung BT and coworkers showed that increasing fiber intake (from mean 6.7 g/day up to mean 13.1 g/day) with pre-germinated brown rice was effective in controlling blood glucose and lipid levels as well as body weight in people who consume rice as a staple food [10]. White rice has a higher glycemic index and less fiber than brown rice. So perhaps fiber is effective in controlling blood glucose. The main source of fiber in Vietnamese cuisine is vegetables. Vietnam can produce vegetables throughout the year, e.g. in the northern part of the country 60-80 kinds in winter and spring, 20-30 kinds in summer [16]. However, according to a Vietnamese general national survey (2010), the average consumption was about 190 g/person/day [9]. This was less than the Vietnamese recommended daily allowances for adults (300 g/day) [17] and less than the Vietnamese clinical treatment guideline for type 2 DM patients (300-500 g /day) [1].
We have formed a hypothesis as to why Vietnamese consume low amounts of vegetables. We think it is because of a lack of nutrition knowledge (particularly the notion that eating meat is more prestigious than eating vegetables) and limited time for cooking, which leads to monotonous methods of cooking vegetables. In World-wide there is variety of methods for preparing vegetables. We attempted to adapt these. We tried dressing and mayonnaise, and studied the effect on vegetable intake and glycemic control. Some people worry about the high cholesterol of mayonnaise, however, the 2015 Dietary Guidelines Advisory Committee stated in its report that Previously, the Dietary Guidelines for Americans recommended that cholesterol intake be limited to no more than 300 mg/day, however, with available evidence, no appreciable relationship between consumption of dietary cholesterol and serum cholesterol [18]. This report made us confident about using mayonnaise.
2. Materials & Method
2.1 Setting and study subjects
The study was designed as a randomized controlled trial and was conducted in April 2017. This research received permission to proceed from Hanoi Medical University’s ethical committee. The study population consisted of type 2 DM outpatients being treated at hospital located in Hanoi City (northern Vietnam). After screening data for about 2000 type 2 DM outpatients at the hospital, we selected about 300 type 2 DM who met the inclusion criteria: (1) Type 2 DM out-patients aged 45-70 years old and with a diabetic history of more than 2 years at Dong Da Hospital, (2) they were receiving only oral medication and had not changed oral medication for 3 months (3) they did not suffer from other diseases (except hypertension and dyslipidemia). Through contacting by phone and meeting directly in the out-treatment clinic, 60 subjects who agreed to participate in this study were enrolled. Then 30 matched pairs were created by sex, age, BMI and years with DM. The subjects were divided into 2 groups: a vegetable group and a control group. Before implementing the study, a pilot study was carried out on 10 people at Hanoi Medical University Hospital (HMUH) to choose 22 menus and 3 kinds of dressing and mayonnaise to apply in this study. This study was implemented at Hanoi Medical University (HMU).
One week before intervention day, all the patients were assembled to be introduced to the research, to sign the consent form and to be instructed on how to record dietary items by the weighing method. During this week, patients recorded all the food they consumed for three days.
After conducting a dietary record for 3 days, both groups received nutrition education about dietary guidelines for DM patients, especially the role of vegetables, and were given nutrition education materials. For the vegetable group only, participants received further instruction on new methods of preparing vegetables using dressing and mayonnaise, ate samples and were given menus and products to use at home. All patients underwent anthropometric measurements and blood tests and submitted dietary records to the researcher at this time (baseline data).
For the next two weeks, the vegetable group applied the new vegetable cooking methods but the control group continued their diet without using dressing and mayonnaise (they received only nutrition education). All patients recorded dietary information for the last 3 days of the research period. During the whole study period, investigators contacted the subjects every day by telephone and found that the rough intake of vegetable was close to the results of the nutrition survey during the last 3 days.
After 2 weeks, all patients were assembled to collect final data on anthropometric measurement, blood tests, and dietary records during the research period.
For the equal treatment of the two groups, after the study, the control group also received vegetable cooking method instruction and was given products to ensure equitable treatment in keeping with ethical requirements.
2.2 Anthropometric measurement
Weight, height, waist and hip circumferences and body fat percentage were measured twice, at the beginning and on the last day, and the average value was calculated for each individual. Body weight and height were measured in light clothing and without shoes. Body mass index (BMI) was computed as the ratio of weight (kg) per height squared (m2). Waist circumference was measured at the minimum circumference between the umbilicus and iliac crest; hip circumference was measured at the widest circumference around the buttocks. Waist-hip ratio was calculated as waist circumference (cm) divided by hip circumference (cm). Body weight, percent body fat, percent muscle and visceral fat were measured by bioelectrical impedance using a body fat analyzer Tanita BC-526-WH scale (Tanita, Tokyo, Japan).
2.3 Blood test
Intravenous fasting blood samples were taken in the morning at baseline and final (after 2 weeks). Various indicators such as FBG and fructosamine were analyzed. Blood tests and analysis were done at HMUH.
2.4 Nutrition survey
A nutrition survey for 3 days by the weighing method was conducted before and during the intervention period. Each patient was given a scale to weigh all the food they ate and wrote dietary record by themselves. Energy and nutrient intakes were calculated based on the Vietnamese Food Composition Table 2007 [8]. We did not include potatoes, rice or beans as vegetables, following the Vietnamese definition [8].
2.5 Statistical analysis
Quantitative variables were checked for normal distribution and compared by the Student t-test paired and unpaired. p-values of less than 0.05 were considered statistically significant for all the analyses. The above statistical procedures were performed using Stata version 12.0.
3. Results and Discussion
We had some drop outs. With regard to the chemical blood data of the control group, at baseline, 2 patients ate breakfast and we did not use their data. Keeping the dietary record by the weighing method was difficult for some patients, so 4 patients either did not record their dietary intake or maintained such poor dietary records that we were not able to analyze them properly.
Table 1 shows comparison of physical characteristics and biochemical parameters at baseline and final of control and vegetable group. In the vegetable group, fructosamine for both genders was significantly reduced after intervention, compared to the baseline. Such reduction was not found in the control group. Average BMI in all the groups were 23.7-24.4, which were the normal range. There were no statistical differences in other item such as age, weight, BMI, body fat, visceral fat or FBG between the control and intervention group and changes in these values during the 2 week study period (P>0.05).

Table 2 shows that energy and nutrient intakes of both groups at baseline and final data within the group do not differ except for fiber. The fiber intake of both groups increased. With the vegetable group, fiber intake increased significantly (P<0.05).
Statistical analysis was conducted by unpaired Student t-test.
Figure 1 shows that the control and vegetable group consumed about 300 g and 450 g at final period, respectively. From our daily contact, these values were maintained throughout the whole period.
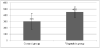
Figure 2 shows the relationship between change in vegetable intakes and change in blood fructosamine level. There was a negative correlation between the changes in vegetable intake and changes in fructosamine level (p<0.05).

The present 2 week intervention study suggests that increasing vegetable consumption is useful in controlling blood fructosamine levels in Vietnamese DM patients. The main focus of the study was a reduction of fructosamine by increasing vegetable intake. Fructosamine clearly decreased in the intervention group but did not change in the control group. In addition, we observed a negative correlation between vegetable intake and blood fructosamine levels. This proved that an increase in vegetable intake was associated with a reduction of blood fructosamine levels.
A decrease in vegetables as well as fiber in the meals of Vietnamese people has been a matter of concern. Cooking methods for meat are increasing in diversity but those for vegetables are still monotonous. There are three popular vegetable cooking methods in Vietnamese cuisine. These are boiling (boiled vegetables are dipped in fish sauce), stir-frying (with oil, garlic, etc) and soup (with salt and seasonings). We analyzed vegetable cooking methods in various countries and found that the major difference from ours from the Vietnamese methods is the use of dressing and mayonnaise.
In this study, at baseline, vegetable intakes of patients were in the range of 200-300 g. Most patients who agreed to participate in this study cared about the diet for type 2 DM and had some knowledge about nutrition. So it is understandable that they consumed more vegetables than average people (about 190 g vegetable/day) [9]. However, it was still not enough, compared with Vietnamese clinical treatment guidelines for type 2 DM patients (300-500 g vegetable/day) [1] or the Japanese guidelines for treatment for diabetes 2013 (>350 g vegetable/day) [15].
We found that the control and intervention groups consumed about 300 g and 450 g vegetable respectively. From our daily contact with the subjects, most of them maintained these levels throughout the whole period. The control group consumed about 300 g vegetable (reaching the recommendation [1,17]); we think that this was the effect of nutrition education. The increase of vegetable intake in the intervention group compared to the control group may be a further effect of using dressing and mayonnaise.
Energy intake was estimated by the weighing method for 3 days, which placed a heavier burden on the subjects but brought reliable results about patients’ actual intake. We found that the energy intakes at baseline in the two groups achieved the Vietnamese clinical treatment guideline for DM patients [1]. For overweight judged by Asia’s cut-off point (23-24.9 kg/m2) [19]: energy intake of 25 kcal/kg ideal body weight/day is recommended. Since BMI of all the groups were from 23.7 to 24.4, their weight was similar to standard values. Most of the subjects were already retired so their physical activity was light and their economic level was low. In addition, protein: lipid: carbohydrate ratio was about 20%:25%:55% (reaching the Vietnamese recommendation for DM patients [1]). Therefore, DM patients should maintain the energy and nutrient ratios that they already consumed except for fiber. Fiber intake was very low at baseline (being less than 8 g a day), compared with the recommendation [1]. In the intervention group, the increase in fiber was about 3 g, suggesting that even a small quantity of fiber as in this study is effective in controlling blood glucose. However, the intervention group’s intake reached a high level and it was perhaps difficult to consume more vegetables. Therefore, we should consider some other sources of fiber to include in main dishes such as brown rice and other sources such as fruit, potatoes and soybean pulp, which is a byproduct of tofu production and currently used as animal feed. Dietary fiber causes a delay in the absorption of carbohydrates, resulting in lower postprandial blood glucose.
This may also explain why the subjects’ BMI was not high even though DM patients worldwide are usually obese. We chose subjects randomly and did not consider BMI but most of our subjects had a normal BMI. In addition, the results of our DM patients’ BMI were similar to other studies which have reported about BMI of Vietnamese DM patients [2,4,7]. Another Vietnamese study indicated that DM patients have a normal BMI (WHO’s cut-off point (18.5-24.9 kg/m2) [19]); when they begin developing DM [2]. This suggests that the prevention of type 2 DM needs to focus on fiber intake more than on obesity.
Abdominal adipose tissue is one of the major causes of insulin resistance. The waist circumference and waist/hip ratio of DM patients in this study were higher than the normal cut-off point for Asia (85 cm and 0.9 for males; 80 cm and 0.8 for females) [14]. Some previous Vietnamese studies also have reported high waist circumference and waist/hip ratio [2,4,7]. We also observed that body fat in females was much higher than in males. Conversely, mean visceral fat for males was in the high range and for females was in the normal range [20]. Vietnamese males may possibly have unhealthy lifestyles such as consuming tobacco, alcohol, etc.
In this study, the limitation was that we made matched-pair groups by sex, age, BMI and year of DM but not by fructosamine or vegetable intake, because the fructosamine measurement and dietary record were conducted after the two groups were established. Because of this the baseline results were not the same. However, when we view the results within groups, fructosamine decreased in the vegetable group and vegetable intake increased in both groups but increased more in the vegetable group. The above limitations could have been avoided if we had done a cross-over design study. We regret that we were not able to do this due to limitations in research funding and time. The study was carried out in short term so effect may not sustainable in the long term. However, we hope through this study, Vietnamese food culture about vegetable will be more variety; patients eat higher vegetable to contribute positively treatment.
4. Conclusions
In conclusion, by using dressing and mayonnaise for 2 weeks, vegetable and fiber intakes were about 450 g and 12 g a day respectively, were effective in decreasing fructosamine concentrations.
Competing Interests
The authors declare that they have no competing interests.