


1. Introduction
Adolescent mothers have been reported to experience difficulties with parenting, repeat pregnancies, and failure to complete high school [1-2]. Pregnancy in adolescence can be viewed as a complex social problem. As such, core aspects of Bronfenbrenner’s theory of human ecological development are proposed as an organizing framework [3]. Bronfenbrenner identified competing factors essential to the understanding of an individual’s environment [4]. These factors include the individual’s microsystem, mesosystem, and macrosystem. For example, the microsystem for an adolescent mother can be reflected in her unique psychological characteristics, her physical factors such as age, and her immediate physical setting such as her home. Mesosystem factors include individuals and institutions in the community such as peers, school systems, and community agencies. Macrosystem factors could include state and federal initiatives designed to reduce pregnancy among adolescents and improve their parenting.
While adolescent pregnancy and birth rates have been declining over the last decade, they remain unacceptably high at both national and state levels [5]. According to Martin, Hamilton, Osterman, Curtin, and Mathews a total of 305,388 babies were born to women aged 15-19 years, for a live birth rate of 29.4 per 1,000 women in this age group [6]. Although this is a record low since its peak in 1991, rates for adolescent pregnancy in Texas are a persistent health disparity [7]. The overall birth rate for Texas is 1.5 times higher than the national birth rate. The birth rate for Hispanic adolescents in Texas is 1.3 times higher than the national birth rate for Hispanics [8].
According to Mytton, Ingram, Manns, and Thomas, “parenting programs are increasingly recognized as an intervention with the potential to improve the health and well-being of both parents and children (pg. 127) [9].” These authors performed a systematic review of qualitative studies in which the perceptions of parents and researchers were compared in terms of the program benefits and weaknesses. Parent perceptions were most favorable when the program had a focused message, was delivered by a trusted individual, provided opportunities for group learning, and offered attainment of new parenting skills.
Since 1982, the Office of Adolescent Pregnancy Programs (OAPP) began funding two types of projects: (1) Prevention Demonstration Programs (i.e., abstinence only); and (2) Care Demonstration Programs to improve parenting, health, and life course outcomes for pregnant and parenting adolescents [10].
One such Care Demonstration Project is Project Mothers and Schools (MAS), which offers services to adolescent mothers attending 8 high schools and 5 alternative schools/academies within an urban Texas county. This school district services a large geographical area and represents approximately 25 zip codes. Six of these 25 zip codes were identified as high risk areas for public health due to high numbers of births to school age mothers. Using a case management approach, family social workers provide home visits focused on parenting skills, continued education, family planning, and life skills.
Project MAS received 5-year funding to evaluate the impact of a community-based intervention for pregnant and parenting adolescents enrolled in school. The goal of this study was to examine if intervention services would influence the likelihood of high school completion, increase parenting skills, and delay subsequent pregnancies among adolescent mothers enrolled in Project MAS. The following research questions were examined:
# 1: Will adolescent mothers who receive intervention services be more likely to complete high school or obtain a GED than adolescent mothers who receive the basic core services?
# 2: Will adolescent mothers who receive intervention services score higher on measures of parenting than adolescent mothers who receive the basic core services?
# 3: Will adolescent mothers who receive intervention services be less likely to have subsequent pregnancies than adolescent mothers who receive the basic core services?
2. Materials and Methods
2.1 Participants and Setting
The population for this study was adolescent mothers eligible and enrolled in Project MAS in an urban Texas county, between 14 and 18 years of age, who were not currently pregnant and who had delivered an infant within the last 3 months. Both English and Spanish speaking adolescent mothers were eligible for enrollment. The majority of these adolescent mothers (90%) self-reported their ethnicity as Hispanic.
2.2 Recruitment and Human Subjects Protection
Prior to conduct of this study, Institutional Review Board (IRB) approval was sought and obtained from the University of Texas Health Science Center at San Antonio. Using school records, Project MAS staff identified and contacted eligible adolescent females to describe their services. Informed consent was obtained from all adolescent females and at least one of the parents among those willing to participate in the study.
2.3 Design
The study design was an experimental, randomized controlled trial of adolescent mothers in an urban setting. The purpose was to assess the impact of post-delivery services on two groups of adolescent mothers, an intervention and a control group. The intervention group received Project MAS core and wrap around services, whereas the control group only received core services (see Table 1 for description of services). Data collection occurred at baseline (within 1-3 months post-delivery), 12 months follow-up (plus or minus one month) and at 18 months (plus or minus one month).

2.4 Analyses and power calculation
To evaluate high school completion and subsequent pregnancies, descriptive statistics and χ2 analyses were performed. To evaluate changes in parenting skills, a series of repeated measures ANOVAs were performed. To determine an appropriate sample size to have adequate power for the analyses, a medium effect size with a beta of .80 and p value of .05 was selected. Based on these parameters, the minimum sample size for the χ2 analyses was 80 and for the repeated measure ANOVAs, the minimum sample size was 100 [11].
2.5 Instruments
This study used data from two instruments administered by Project MAS staff. The Adolescent Family Life (AFL) Core Evaluation Instrument was developed for demonstration projects funded under Title XX of the Public Health Service Act and administered by the Office of Population Affairs [12]. Items were drawn from large surveys, giving the ability to compare community data to national data. Selected items for the current study included demographics, academic completion and subsequent births.
The Adult Adolescent Parenting Inventory-2 (AAPI-2), a normed and standardized research-based assessment tool, was developed to assess parenting and child-rearing attitudes among adult parents, adolescent parents, and expecting parents [13]. A recent article supported the reliability of the AAPI-2 with at-risk, low income, adolescents [14].
The AAPI-2 assists in identifying maladaptive parenting attitudes and behaviors that may require intervention. The AAPI-2 has been used for over 30 years in numerous studies and projects. The instrument consists of 40 items with five subscales. The subscales provide individual scores for Expectations of Children, Empathy toward Children, Use of Corporal Punishment, Parent-Child Role Reversal and Children’s Power and Independence. Item and factor analysis were used to determine the content related validity of the instrument. Cronbach estimates of internal reliability range from .86 to .96 for the five subscales on the AAPI-2.
Domain responses are coded two ways: (1) standard ten scores (sten) scores, which are standardized on a scale from 0-10, in which higher scores indicate more appropriate parenting attitudes and behaviors, and (2) RISK scores, which are scaled from 0-2, in which higher scores indicate more risk. For the current study, sten scores were chosen for analysis due to greater variability leading to higher precision.
3. Results
3.1 Participation in data collection
The total sample at baseline consisted of 172 adolescent mothers (86 in each group). At 12 months, the total sample consisted of 129 adolescent females (64 intervention and 65 control). At 18 months, the total sample consisted of 103 adolescent females (52 intervention and 51 control). Interpretation of the findings from chi-square analyses at baseline, 12 months, and 18 months failed to yield significant differences in group characteristics.
3.2 Demographics
In general, the adolescent females were slightly under 17 years of age at enrollment and slightly over 18 at study completion. In addition, the sample remained predominantly Hispanic across all time periods (Table 2).
3.3 Research question # 1
Will adolescent mothers who receive intervention services be more likely to complete high school or obtain a GED than adolescent mothers who receive the basic core services?
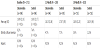
At baseline, only 10% of intervention mothers and 8% of control mothers had completed high school or earned a GED (Table 3). At 12 months, 38% of intervention mothers and 40% of control mothers had completed high school or earned a GED. At 18 months, 48% of intervention mothers and 52% of control mothers had completed high school or earned a GED. By 18 months, only 8% of intervention mothers versus 11% of control mothers had dropped out of school. There were no differences in educational attainment across the data collection points.

3.4 Research question # 2
Will adolescent mothers who receive intervention services score higher on measures of parenting than adolescent mothers who receive the basic core services?
To measure parenting, the five sten scores for the AAPI-2 domains were assessed. The domains measure inappropriate parenting knowledge/attitudes and as sten scores increase (range 0-10), they reflect better parenting knowledge/attitudes. To evaluate changes in parenting skills, a series of repeated measures ANOVAs were performed using time (i.e., baseline, 12 and 18 months) and group (i.e., control versus intervention) as the independent variables and each sten score for the dependent variable. From baseline to 12 months, there was a significant increase in the five mean sten scores for all mothers irrespective of group (Table 4a for mean score differences and Table 4b for the repeated measures ANOVAs).
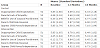

In contrast, from 12 to 18 months, both control moms and intervention moms showed slight decreases in mean scores for the AAPI-2 construct, Inappropriate Child Expectations. Interestingly, from 12 to 18 months, control moms showed small but significant improvements in two AAPI-2 constructs (i.e., Belief in Corporal Punishment, and Oppress Child Power/Independence), and intervention moms evidenced small but significant decrements in the same two AAPI-2 constructs.
3.5 Research question # 3
Will adolescent mothers who receive intervention services be less likely to have a subsequent pregnancy than adolescent mothers who receive the basic core services?
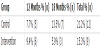
To assess if adolescent mothers receiving intervention services were less likely to have a subsequent pregnancy, χ2 analyses were performed at 12 and 18 months (Table 5). Only 15% or fewer of all adolescent mothers had a subsequent pregnancy by 18 months. The rate of subsequent pregnancies was lower for intervention mothers (15.3%) than for control mothers (21.2%), however, this was not a statistically significant difference.
4. Discussion
The overall objectives of Project MAS were to help adolescent mothers continue their education, to increase linkages to social support, to support self-sufficiency, and to help adolescent mothers and their families create an environment that is nurturing, positive, safe and supportive. In terms of the research questions, the results indicated that adolescent mothers were more likely to complete high school or obtain a GED, scored higher on measures of parenting over time, and were less likely to have a subsequent pregnancy. However, it should be noted that while there were positive outcomes overall, few differed by group assignment.
In retrospect, adolescent females in both groups received homebound education. The focus of home-bound education was individual academic instruction, which occurred weekly and was at least 6 weeks in length. Given that there were no group differences in completing high school or obtaining a GED, it suggests that the core services of home-bound education are sufficient to support academic completion in this population. These findings are consistent with other researchers who have noted that home-bound education/visiting was an essential intervention to alleviate risk through education, emotional support, and care coordination [15-16].
In addition, adolescent females in both groups received in-home case management that consisted of parenting education, family support plans, and community services. Family support plans included contraceptive planning, importance of spacing subsequent pregnancies, and education to prevent sexually transmitted infections (STIs). Community services encompassed: pregnancy testing and maternity counseling, adoption services, primary and preventative health care, nutrition information and counseling, screening and treatment of STIs including HIV/AIDS, pediatric care, educational services related to family life and problems associated with adolescent sexual premarital relations, educational and vocational services, mental health services and referral to mental health providers, counseling and referral to family planning services, and additional case management as needed. This wide array of community services was coordinated through Project MAS and integrated professional services from over 20 community agencies. Hence, it is not surprising that adolescent females in both groups had improved parenting skills at 12 months. This suggests that the core services for parenting education were sufficient to enhance parenting among adolescent females. Similarly, also using the AAPI-2, Barnet et al. found that a community-based home visiting program focused on parenting had a positive impact on parenting attitudes and beliefs among adolescent mothers [1].
It is interesting to note that although there were few changes in parenting skills from 12 to 18 months, changes for adolescent females in the intervention group were lower than expected and changes for adolescent females in the control group were higher than expected. While no definitive statements are possible, it should be noted that adolescent females in the intervention group received an additional six months of home-bound/group parenting education (i.e., wrap-around services, the primary intervention) than did their counterparts. Perhaps this intensive process led to greater awareness and introspection regarding their actual parenting, influencing their responses.
As noted earlier, in-home case management focused extensively on family planning services, pregnancy testing, and maternity counseling. Hence, it would be expected that all adolescent females in this study would recognize the importance of delaying subsequent pregnancies, which was supported in the data. Similarly, Sadler et al. found that adolescent mothers were more likely to delay subsequent pregnancies and stay engaged in school when they were enrolled in a school-based parent support program [17]. Likewise, Sangalang, Barth, and Painter noted adolescent mothers postponed subsequent births after receipt of case management and direct services from social workers [18].
5. Strengths and Limitations
This study had several strengths. Of note was the equivalency of groups at baseline on standardized instruments which facilitated comparisons across all time periods. A review of responses on standardized instruments revealed these adolescent mothers had few or no missing data. The use of the AAPI-2 risk scores throughout the study alerted Project MAS staff to those young women who required targeted interventions and follow-up regarding parenting and family support. Adolescent mothers in the study were assigned family social workers who delivered these services. While all family social workers were aware of the study aims they did not restrict services to only those adolescents in the intervention group.
Thus, while the comprehensive program services of Project MAS served as a major study strength, the lack of restriction to these services is also a major limitation. A review of dosage records revealed that when adolescents in the control group were in need of additional services they were provided similar services to the intervention group. Therefore while the study design was originally deemed an experimental, randomized controlled trial of adolescent mothers in an urban setting, in actuality it was not. Instead, the extension of services to the control group resulted in “experimental diffusion,” which occurs when there is a blurring of distinction between the intervention and control group. Hence, one challenge is to determine how to better balance a research design with delivery of comprehensive services.
Another limitation may have resulted from the intervals in data collection time periods. For example, the lack of significant differences from 12 to 18 months (e.g., educational attainment and subsequent pregnancies) may be due to insufficient time between data collection. Future research may want to examine the value of spacing data collection periods consistently by 12 months.
6. Conclusion
The main implications of this study are the value of communitybased partnerships in the delivery and evaluation of services to at-risk adolescent mothers [19]. Research has shown community and schoolbased services targeted at young mothers and children result in better short and long-term outcomes and have the potential to improve their health and well-being [1-2,9].
Another implication is the need for increased awareness of the challenges when conducting community-based research. In the present study, the authors served as program evaluators and collaborated with the community-based partner on design, analysis, interpretation, and reports. While the authors were most concerned with the study design, methods and results, the community-based partner emphasized delivery of comprehensive services based on ongoing assessment of adolescent mothers’ needs. Similar challenges were noted by Strunk in an integrative review summarizing data from 13 studies [2]. Strunk reported that all of these studies were limited due to smaller sample sizes, weaker design choices, and selection bias. Strunk’s findings highlight the emphasis of training and rigor among researchers. However, Mytton et al. recognized that participants and researchers differed in their perceptions of essential program qualities [9]. The most essential qualities from the participants’ perspectives was learning new skills, meeting others, and having a trusted or known person in the deliverer role. In contrast, the most essential qualities from the researchers’ perspectives was designing a program using a conceptual framework, tailoring messages to individual participants, and ensuring deliverers were well-trained.
The findings from this study support the importance of a selectively focused program to foster positive outcomes for adolescent mothers. Meeting the needs of these mothers necessitated a selective approach, one in which the unique needs of minority low-income mothers were addressed. Within Project MAS, the family social workers were nonjudgmental and compassionate with the mothers. A recent study found that social support from families, friends, and professionals was positively correlated with young mothers’ confidence in parenting skills [20]. Perhaps the interactions with family social workers from Project MAS with all adolescent mothers in the study may explain the positive outcomes for both groups.
Competing Interests
The study sponsor had a role in the study design, however, the authors had full access to all of the data in this study and take complete responsibility for the integrity of the data and the accuracy of the data analysis. Thus, the authors declare that they have no competing interests.
Author Contributions
Both authors endorse that they have made substantial intellectual contributions to this published study. Both authors were involved in the design, acquisition of data, and analysis and interpretation of data. Both authors have developed the manuscript.
Acknowledgments
Research reported in this publication was supported by the Department of Health and Human Services, Office of Adolescent Pregnancy Prevention (DHHS-OAPP), Project #: 1 APHP006042-01 (2008-2012). The content is solely the responsibilities of the authors and does not necessarily represent the official views of the DHHSOAPP.