


1. Background
Nurses having an important role in the health care system. they are considered to be members of a stressful job as a profession because they care for a stressful group comprising patients or those at health risk. The organizational structure of the health care system, improper working environment, critical patient care, working on a shift basis and the process of becoming a profession can affect the level of stress in nurses [1]. According to literature review the hardest hit by burnout are the service providers like nurses and counselors. When a professional is affected by burnout they feel drained and used up and have little desire to return to work the next day. This problem is specific to the work context. It is generally perceived that Intensive Care Nurses are particularly exposed to burnout since they literally deal with life and death situations most of the time. Therefore, it is suggested that nurses comprise the group that experiences the maximum stress, and burnout among health professionals. Burnout syndrome often occurs as a result of chronic work stress seen in Intensive Care Units [2].
The most widely referred definition of burnout among general occupations conceptualizes the phenomenon as "a syndrome of emotional exhaustion, cynicism and reduced professional efficacy". Researches suggest that burnout contributed to job stressors is associated with a negative outcome in both individuals and organizations. At an individual level, burnout has been associated with mental and physical health problems, for example, psychological distress, anxiety, depression, reduced self‐esteem [3]. At an organization level, burnout is also consistently linked to negative attitudes towards work, which include low levels of motivation, job satisfaction and organizational commitment, but high levels of job uncertainty [4]. These in turn induce counter‐productive work behavior, such as reduced productivity, absenteeism and staff turnover and hence lower the overall effectiveness of the organization itself [5]. Furthermore, some researches suggest that burnout is contagious, spreading to affect the colleagues of those who experience it and even resulting in negative spillover into one's home life [6]. From this standpoint, burnout is not only an individual well‐being issue but could also influence socio‐economic factors.
Coping behavior is a constantly changing cognitive and behavioral effort to manage specific external and/or internal demands that are appraised as taxing or exceeding the resources of the person. Coping behavior affects well-being and adaptation; In addition, coping behavior has also received attention from nursing researchers [7]. There is a growing understanding that coping strategies, which have been regarded as a psychological intervention in the stressor–strain relationship, play an important role in influencing the tangible and intangible outcomes of the stressor [8].
Coping strategies act as a variable that affects the direction and/or strength of the relation between an independent or predictor variable and a dependent or criterion variable’-it is reasonable to suggest that coping strategies may have a moderating effect on the relationship between the stressor and its consequential strain. Role overload may be regarded as a form of stressor, and burnout is one relevant stress reaction (i.e. strain), coping strategies are therefore likely to have a moderating effect on the relationship between role overload and burnout. Therefore, given constant role overload levels, the presence of coping strategies weakens the stressor-strain relationship, reducing the levels of burnout in the individual [9].
1.1 Significance of the study
Nursing is a sensitive job which includes communicating with patients and caring after them; failing to identify and fighting the accompanying stress can have dire consequences. In such units as CCU and ICU the problems nurses encounter are more serious and they are subject to greater levels of stress. Obviously, the main reason for most physical and mental disorders is one's inability to deal with psychological pressure, which in turn affects one's reactions to stress [10]. The provision of Intensive Care (IC) can lead to a health care provider’s physical, psychological and emotional exhaustion, which may develop into burnout. The researcher noticed that there was a limited specific study regarding this syndrome at Intensive Care Units (ICUs) in Assiut University Hospital. The findings will address some implication concerning the managerial coping strategies adopted by nurses at ICUs in the healthcare settings when dealing with job related burnout and role overload.
1.2 Aim of the study
The present study aims to investigate relationship among nurses role overload , burnout and managerial coping strategies (i.e. rational problem solving, resigned distancing, seeking support/ventilation and passive wishful thinking) at Intensive Care Units in Assiut University Hospital.
1.3 Research questions
- Is there a relationship between managerial coping strategies and nurses role overload?
- Is there a relationship between managerial coping strategies and nurses burnout?
2. Subjects and Methods
2.1 Study design
A descriptive design was used to carry out the present study.
2.2 Setting
The study was carried out at four Intensive Care Units in Assiut University Hospital which including the following: Causality Intensive Care Unit, General & Postoperative ICUs, and Coronary Care Unit (CCU).
2.3 Subjects
Includes all nurses working in aforementioned settings with a total number of 6 0 nurses classified as the following:
| Place of work | Number of Diploma degree Nurse | Number of Technical degree | Number of Bachelor degree Nurse |
| Causality Intensive Care Unit | - | 5 | 15 |
| General ICU | 18 | 7 | 4 |
| Postoperative ICU | 10 | 10 | - |
| Coronary Care Unit | 16 | 10 | 4 |
2.4 Tools of data collection
Four tools were used to collect data for this study as follows:
1st tool : Socio-demographic data sheet:
This part includes socio-demographic characteristics data as: age,
sex , unit name, marital status, educational qualification, and years
of experience.
2nd tool : Role overload questionnaire which developed by [11], it
included five items. The Scoring system of this tool was five-point
Likert-scale ranging from “strongly disagree” (1) to “strongly agree”
(5).
3rd tool : Managerial coping strategies questionnaire which
developed by [12] , it included twenty nine items classified into
four factors. Rational problem solving, resigned distancing, seeking
support/ventilation and passive wishful thinking. The Scoring system
of the this study tool was four-point scale in the following sequence (0
= not used, 1= used somewhat, 2 = used quite a bit, 3 = used a great
deal), and
4th tool: Burnout questionnaire which developed by [13], it included
twenty two items. The Scoring system of this study tool was five-point
Likert-scale ranging from “Not important” (1) to “More important”
(5).
Their reliability was assessed in a pilot study by measuring their
internal consistency using Cronbach's alpha coefficient method. This
turned to be 0.88 for coping strategies, 0.90 for burnout, and 0.96 for
role overload, thus indicating a high degree of reliability .The validity
was measured by five experts in the field of nursing administration.
2.5 Pilot study
The pilot study also served to test the feasibility of the study and the clarity and practicability of the data collection tool. It was carried out on 20 nurses from different inpatient departments in Assiut University Hospital. The pilot study collected on April 2015. The subjects included in the pilot study were excluded. Data collected from the pilot study were reviewed and used in making the necessary modifications prior to the finalization of the data collection tool.
2.6 Fieldwork
An official permission was obtained from the hospital director, the nursing service director, and the head of each Intensive Care Unit before embarking on the study. The actual data collection was started in June 2015 and ended in July 2015. The researcher met the eligible nurses, explained to them the purpose of the study, and asked them for their oral consent to participate. Those who agreed to participate were given the tools and asked to fill them out and return them anonymously in the same setting or at most the next day.
2.7 Ethical considerations
The study protocol was approved by the pertinent authority. Participants’ oral consent to participate was obtained after informing them about their rights to participate, refuse, or withdraw at any time. Total confidentiality of any obtained information was ensured. The study maneuver could not entail any harmful effects on participants.
2.8 Statistical analysis
Data entry and statistical analysis were done using SPSS 16.0 statistical software package. Data were presented using descriptive statistics. Pearson correlation analysis was used for assessment of the inter-relationships among quantitative variables, and Spearman rank correlation for ranked ones. Statistical significance was considered at p-value <0.05.
Table 1: Illustrated that more than three quarters of study subjects were aged less than 30 yrs and more than one quarter worked at Coronary Care Unit, 98% were females and half of them were single. While, 44% had a diploma degree and more than half of the study subject had less than 5 years of experience.

Table 2: Showed that role overload had highest mean score in general ICU followed by Casuality ICU (16.51±3.18 & 15.71±3.18) . In addition, managerial coping strategies highest mean scores of rational problem solving , resigned distancing, and seeking support/ ventilation were in Casuality ICU followed by post operative ICU ( 34.80±4.08& 33.50±7.68 ; 11.42±2.35 & 10.55± 0.32; and 15.23±3.40 & 14.50±3.76) respectively except passive wishful thinking had highest mean scores in General ICU followed by Casuality ICU (12.68±3.08 & 12.28±3.63).Also, burnout had highest mean scores in post operative ICU followed by general ICU (66.30±14.54 & 63.17±14.72) respectively.
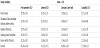
Table 3: Illustrates that burnout had positive relations with managerial coping strategies with a highly statistically significant differences (r = 0.49**(. While, there were no relation between role overload & burnout (0.16) and role overload & coping strategies (0.13).

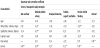
Concerning the relations of study variables with nurses' sociodemographic characteristics, Table 4) demonstrates that burnout had positive relations with role overload , rational problem solving, resigned distancing, seeking support/ventilation and passive wishful thinking coping strategies with a highly statistically significant differences (r = 0.49** , r = 0.34** , r =0.23* ,r = 0.32**, and r = 0.45**) respectively. While, role overload had weak negative statistically significant correlation with qualifications (r= -0.14). In addition, burnout had weak negative correlations with age, marital status, educational qualifications, and years of experience (r= 0.13, r= -0.02, r= -0.02& r= -0.14) respectively. Also, rational problem solving coping strategy had weak negative statistically significant correlations with age, marital status, and years of experience (r=-0.03, r= -0.23, & r= -0.06) respectively. Meanwhile, resigned distancing & seeking support/ventilation and passive wishful thinking coping strategies had weak negative statistically significant correlations with age and marital status( r= -0.09 , r= -0.18; r=-0.08, r= -0.19 & r= -0.12 , r= -0.26) respectively. There were positive relation among role overload and age, marital status, and years of experience (r = 0.04, r = 0.02 & r = 0.05) respectively. Educational qualifications had positive relations with the four managerial coping strategies rational problem solving , resigned distancing, seeking support/ventilation, and passive wishful thinking ( r = 0.37**, r = 0.04, r = 0.20 &r = 0.07) respectively. Role overload had positive relations with rational problem solving, resigned distancing, and passive wishful thinking managerial coping strategies ( r = 0.10, r = 0.14 & r = 0.07) respectively except seeking support/ventilation coping strategy had a negative relation with role overload (r = -0.01).
3. Discussion
The results of the present study showed that role overload had highest mean score in general ICU followed by Causality ICU . In addition, coping strategies highest mean scores of rational problem solving , resigned distancing, and seeking support/ventilation were in Causality ICU followed by post operative ICU respectively except passive wishful thinking had highest mean scores in General ICU followed by Causality ICU. Also, burnout had highest mean scores in post operative ICU followed by general ICU respectively (Table 2). These results indicated that nurses working in the intensive care unit, coronary care unit and emergency department experienced lower levels of personal accomplishment and high level of stress due to these nurses face more death and dying while exert more efforts. Nurses working in an intensive care unit rarely see patients returning home when hospital treatments are successful so nurses use coping strategies to overcome the effects of job stress.
These results is supported by a study on female hospital nurses, it was reported that affective-oriented coping was significantly associated with depressive symptoms, even after controlling for the effects of job stress, nursing-related work experience, and social support [14]. In addition, a study of hospital nurses in Australia and New Zealand found that type of coping strategy was significantly associated with physical and mental health, after controlling for the effects of job stress [15]. Moreover, [16] also reported that burnout among nurses is reduced when coping skills training was provided. A passive coping style, which is a type of emotion-focused coping, associates with poor health in both Norwegian and Dutch hospital nurses. Nurses with habitual passive coping may experience little control over work and low support within the nursing team [17]. Moreover, [3] concluded that positive stimuli in general make individuals happy whereas in the face of negative stimuli, stress can be generated. While, [18] found that burnout may develop in the individual as a result of a long duration of the state of stress.
On going the results of the current study demonstrates that burnout had positive relations with role overload and different types of managerial coping strategies with highly statistically significant differences (Table 3 & 4). These results might be attributed to the work in the ICUs is hard than other general units because nurses in ICU provide intensive care for a long period (12 hours) shift and after that patients may died so these situation is stressful and lead to burnout. These results supported by [19] who mentioned that there are certain / inevitable stressful factors in nursing that can adversely affect nurses' minds and behaviors; it is important to find ways to deal with these factors before we can take measures to improve nurses' professional quality and teach them coping strategies. Nurses, when experiencing great stress, draw upon various coping strategies, and obviously, their manner of coping with stress and role overload influences the quality of their professional performance. In the same line the study results were in agreement with [20] who clarified that one of the important factors in avoiding burnout is applying stress coping strategies. Moreover, [21] mentioned that two dimensions of coping are problem-focused coping and emotion-focused coping. Problemfocused coping consists of concrete attempts made to alter the stressfulevent while emotion-focused coping consists of attempts made to alter stressful feelings. People typically employ problemfocused coping strategies, purposively targeted at solving the problem at hand, when they perceive control over stressful events. Emotionfocused coping, aimed at minimizing negative emotions through seeking distraction and social support or by avoiding problems, predominates when people feel that the stressful event is something that must be endured.
As shown in (Table 4) burnout had weak negative correlations with age, marital status, educational qualifications, and years of experience. Also, rational problem solving coping strategy had weak negative statistically significant correlations with age, marital status, and years of experience. Role overload had positive relations with rational problem solving, resigned distancing, and passive wishful thinking coping strategies respectively except seeking support/ventilation coping strategy had a negative relation with role overload. These results might be attributed to most of the studied nurses are young aged and had limited years of experience so they had not the ability to use the support /ventilation coping strategy and may be inability to communicate effectively which may reflected on their performance. This finding was inconsistent with [22] Foster, who found that older nurses in the United States experienced a lower level of burnout in emotional exhaustion, depersonalization, and reduced personal accomplishment than younger nurses.
In addition, A study in China found that Chinese nurses tended to cope actively with stress resulting from decreased personal achievement [23], but passively when the stress came from resource and environment problems, patient care and interaction issues, and from interpersonal relationships and management issues. Nurses apply different coping strategies, such as wishful thinking, planned problem-solving, to deal with different stressors, and apply avoidance strategies to cope with stress resulting from the shortage of resources, role overload and interpersonal relationships [23,24].
4. Conclusion
In the light of the study results, the following conclusions can be drawn:
Nurses employed at ICUs in Assiut University Hospital reported high burnout. They were more likely to use managerial coping strategies as rational problem solving, resigned distancing, seeking support/ventilation and passive wishful thinking to handle burnout. While, Role overload had positive relations with rational problem solving, resigned distancing, and passive wishful thinking managerial coping strategies except seeking support/ventilation coping strategy had a negative relation with nurses’ role overload.
5. Recommendations
Based on the forgoing conclusions, the following recommendations are proposed:
- Recognizing the impacts of job-related stress and making use of effective coping methods play a vital role in reducing nurse's burnout.
- Developing and implementing a training program on managerial coping strategies to assist nursing staff in health service institution in Egypt to cope with burnout and role overload effectively.
- A change in leadership styles from the managerial level and reallocation of manpower may help reduce burnout and role overload.
- It is important for nurse managers to recognize passive coping, because this type of coping associates with poor health
- Hospital decision-makers need to consider arranging for the nurses to work in other units for periods of time during the year to buffer their negative experience at work.
- Further researches should be done to investigate relations among job satisfaction, job stress, personality traits and burnout among ICU staff.
Competing Interests
The authors declare that they have no competing interests.