


1. Introduction
An important part of nursing education is clinical training, where nursing students begin to develop professional ethics as healthcare providers and the foundation of their nursing competence. However, academic and personal sources of stress and coping behaviors associated with clinical training have been identified in the literature on mental health distress in nursing students [1]. High levels of stress can affect both academic performance and students’ overall health, leading to issues such as immune deficiency disorders, depression, and suicide [2,3]. In Japan, some students who have unproductive experiences during clinical training end up dropping out due to their inability to cope with the stress [4,5]. Although assessing sources of stress and coping behaviors in nursing students is important, doing so holistically is challenging. Nevertheless, it is now necessary to examine ways to design age-appropriate clinical training based on students’ interpersonal skills and ability to cope with stress [6].
Many previous studies on stress in nursing students during clinical training have found that faculty members and clinical instructors are a source of stress [7,8]. In addition, students’ insufficient knowledge and inexperience in completing clinical practice logs also causes stress[9-11]. It remains unclear what specific aspects of those relationships or clinical practice logs cause stress and what coping strategies can best manage those stressors during clinical training. Coping styles of nursing students in clinical training have been classified as active (positive reframing, planning, acceptance, and active coping) and avoidant (denial, alcohol/drug use, and behavioral disengagement) [3,12]. Other studies have also found that students use a moment-to-moment combination of coping strategies such as problem-solving and avoidance [13,14]. For example, avoidance behaviors helped students in coping with stressors related to patient care, the clinical environment, and teachers and nursing staff. Coping behaviors were also related to individual students’ stress tolerance [15,16]. One useful tool for assessing students’ stress tolerance or coping ability is sense of coherence (SOC). When confronted with a stressful event or situation, those with high SOC can successfully cope with stressors to realize growth and development without harming their mental or physical health [17]. SOC is considered useful for assessing students’ ability to cope with stress because it is a sense that people develop through their experiences until early adulthood.
SOC has also been used in research on nursing education. This research has shown disparities in student achievement, overall health, and self-esteem during clinical practice [11,18,19]. A few studies have examined first- and second-year students who have little experience with clinical practice and nursing skills. For example, a study on SOC and fundamental clinical training found an association between higher SOC and factors such as coping behaviors, positive thinking, and positive actions among nursing students [19]. Students with high SOC were more likely to solve problems proactively or change their perspective to cope with stress related to clinical training, whereas students with low SOC used avoidance strategies such as giving up and abandoning efforts [20].
However,it is difficult to understand the SOC of students before clinical training. Thus, it is not possible to coach in accordance with the high-low level of SOC. At present, the precise association between stress and coping with adjusted SOC and specific improvements in their clinical training remains to be elucidated.We should assess the relationship between stresses and copingbehaviors in nursing students during clinical training while controlling for the confounding factor of SOC.In our investigation on how to make clinical training more effective and appropriate for students, we considered stress-related coping styles of nursing students. The purposes of this study were to identify the structure of stress factors during fundamental clinical training and to determine the relationship between these stress factors and coping behaviors in nursing students while controlling for SOC.The main contributions of this study are provided the effective methods for the nursing students in clinical training.
2. Materials and Methods
2.1 Participants and setting
The participants in this descriptive cross-sectional study were 158 first-year undergraduate nursing students from a university nursing department. The study periods were before and after fundamental clinical training. Among 158 students, 79 were enrolled in 2012 and 79 were enrolled in 2013.
In the fundamental clinical training program at “A” University School of Nursing, students take a five-day, one-credit course during the second semester of their first year. The objective of the fundamental clinical training is for first-year students to build personal relationships with patients and understand the process of solving health problems.
2.2 Data collection
This survey study was conducted using anonymous self-completed questionnaires. After orientations held before clinical training began, all students received questionnaires with identification numbers. Students were instructed to return the questionnaires by inserting them in an envelope and placing them in a designated locked box to ensure the privacy of its contents.
2.3 Measurements
Students’ characteristics: The survey of before clinical training contained questions on age, sex, living environment, and commute time. Both before and after clinical training,the survey contained questions on hours of sleep and subjective health status. Subjective health status was assessed on a five-point scale (1 = good, 2 = somewhat good, 3 = normal, 4 = somewhat poor, and 5 = poor).
Stressors related to clinical training: We included 28 items on events related to clinical training to assess clinical training-related stressors. These 28 items were based on previously identified stress factors related to fundamental clinical training during the first year of college [19,21-23]. Each item was scored on a four-point scale (1= not stressful, 2 = not very stressful, 3 = somewhat stressful, and 4 = stressful).
Ability to cope with stress: We assessed ability to cope with stress using a 13-item Japanese version of Antonovsky’s SOC scale (SOC-13) scored on a seven-point scale. This scale was published by Yamazaki et al. in 1999 and has proven reliability and validity on college students [24]. The SOC-13 has an overall score range of 13-91 points, with higher scores indicating better ability to cope with stress.
Coping behaviors: We assessed coping behaviors using the Brief Scales for Coping Profile, which measures the coping characteristics of workers, and its reliability and validity have been verified in Japan [25]. This scale comprises 18 items evenly distributed among six subordinate concepts: “proactive problem-solving,” “seeking help to solve problems,” “changing mood,” “emotional expression involving others,” “avoidance and suppression,” and “changing point of view.” Each subordinate concept has a score range of 3-12 points, with higher scores indicating stronger coping behaviors.
Statistical analysis: We analyzed only those responses from questionnaires with fully completed SOC-13 items where the surveys before and after clinical training could be compared. First, we compared the characteristics of students who enrolled in 2012 with those of students who enrolled in 2013 by the Mann-Whitney U test and chi-square test, after confirming the normality of each item. Next, we analyzed collected data by exploratory factor analysis (EFA) with promax rotation to identify the main components affecting stress related to clinical training. Preliminary to the EFA, we closely examined the 28 items of events related to clinical training for both item-total and inter-item correlations. The item-total correlation revealed correlation coefficients of 0.3or smaller for four items, which were then excluded. The inter-item correlation revealed correlation coefficients of 0.8 or larger for four items, which were then excluded. Therefore, the EFA was conducted for 20 out of 28 items of events related to clinical training. We also calculated reliability coefficients using Cronbach’s alpha for each identified factor. Furthermore, we assessed relationships between SOC and each identified factor by Pearson’s correlation coefficient. We also assessed relationships between SOC and the six coping types by Pearson’s correlation coefficient. Finally, we assessed relationships between each identified factor and the six coping types by partial correlation coefficient adjusted for SOC score. Statistical processing was performed with SPSS ver. 19 (IBM, Tokyo, Japan). Statistical significance was set at p <0.05.
2.4 Ethical considerations
This study was conducted with the approval of the ethics committee of the author’s institution. Survey respondents were given an oral and written explanation of the study’s purpose, and informed that participation was voluntary, that study results would be analyzed after clinical practice ended, that their participation or non-participation would not affect their clinical practice or grades, and that the confidentiality of their personal information would be protected. Return of the questionnaire was considered implied consent to participate in this study.This study follows the ethical standards established in the Declaration of Helsinki in 1995(as revised in Seoul 2008).
3. Results
Among 148 students who returned the questionnaire (response rate, 93.7%), 132 provided valid responses (83.5%). Among these students, there were 123 women (93.2%) and the mean age was 19.5 years. Ninety-nine students (75.0%) commuted to school from home; with an average commute time of 50.4 min. Students obtained an average of 6.2 hours of sleep. For subjective health status, 71 (53.8%) students answered good or somewhat good and 5 (3.8%) answered poor or somewhat poor.
Between students who enrolled in 2012 and students who enrolled in 2013, we found a significant difference in sex (Table1), but no significant differences in other characteristics such as age, living environment, commute time, hours of sleep, and subjective health status.

3.1 Stress factors related to clinical training
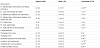
By EFA on clinical training-related stressors, seven factors were found with eigenvalues of 1 or higher and a cumulative contribution rate of 53.1% (Table 2). Seven factors were identified as stress arising from (1) “relationships with teachers and clinical instructors,” (2) “lack of knowledge and skills,” (3) “reflecting on patient-care experiences,” (4) “relationships with patients, families, and healthcare staff,” (5) “conferences,” (6) “peer relationships,” and (7) “daily planning in clinical practice.”

The first factor consisted of four items involving contact with clinical instructors and teachers (e.g., debriefing and guidance from a clinical instructor and/or faculty teacher). Therefore, we identified the first factor as stress from “relationships with teachers and clinical instructors.” The second factor consisted of three items involving insufficient nursing skills and knowledge of students related to the disparity between skills used in classroom practice and skills used in clinical practice. Therefore, we identified the second factor as stress from a “lack of knowledge and skills.” The third factor consisted of three items related to students’ reflecting on their patient-care experiences while writing a case report or using process records and to time management in clinical practice. Therefore, we identified the third factor as stress from “reflecting on patient-care experiences.” The fourth factor consisted of four items related to encouraging a personal relationship with patients and family to developing relationships with healthcare staff. Accordingly, we identified the fourth factor as stress from “relationships with patients, families, and healthcare staff.” The fifth factor consisted of two items related to conference presentations and document preparation for conferences, so we identified this factor as stress from “conferences.” The sixth factor consisted of two items involving cooperation with group members and a shared ward environment. Thus, the sixth factor was identified as stress from “peer relationships.” Finally, the seventh factor consisted of two items involving preliminary review of knowledge and skills relevant to daily action and care plans in practice and it was therefore identified as stress from “daily planning in clinical practice.”
Cronbach’s alpha coefficient for the overall scale (that included 20 items) was 0.84. Cronbach’s alpha coefficient for each factor was F1 = 0.85, F2 = 0.77, F3 = 0.65, F4 = 0.73, F5 = 0.70, F6 = 0.62, and F7 = 0.69.
3.2 SOC, stress factors, and coping behaviors
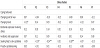
Average total SOC score before clinical training was 51.5 points. Table 3 shows averages for each stress factor and coping behavior. On the whole, we found high levels of stress for three factors: “lack of knowledge and skills,” “reflecting on patient-care experiences” and “conferences” (average SOC scores of 8.9, 9.4, and 6.1, respectively). We also found a negative correlation between SOC score and four stress factors: “relationships with teachers and clinical instructors,” “lack of knowledge and skills,” “relationships with patients, families, and healthcare staff,” and “daily planning in clinical practice” (r = -0.25, r = -0.17, r = -0.20, r = -0.17, respectively; p < 0.05). Whereas the SOC score was negatively correlated with the coping behavior pertaining to “avoidance and suppression” (r = -0.18, p <0.05), the SOC score was positively correlated with four other coping behaviors: “changing mood,” “emotional expression involving others,” “seeking help to solve problems,” and “proactive problem-solving” (r = 0.50, r = 0.46, r = 0.60, r = 0.64, respectively; p <0.01).
3.3 Relationship between stress factors and coping behaviors
Partial correlation analysis between stress factors and coping behaviors adjusted for SOC score showed a negative correlation between the stress factor “relationships with teachers and clinical instructors” and the coping behavior “changing mood” (r = -0.21, p <0.05). A negative correlation also existed between three stress factors “lack of knowledge and skills,” “reflecting on patient-care experiences,” and “conferences” and the coping behavior pertaining to “seeking help to solve problems” (r = -0.19, p <0.05, r = -0.24, p <0.01, r = -0.28, p <0.01, respectively).
4. Discussion
We clarified two important points through this survey. First, we examined the structure of stress factors during fundamental clinical training. Second, we determined the relationships between stress factors and coping behaviors while controlling for SOC.
4.1 Stress Factors in Fundamental clinical training
Using EFA, we found seven stress factors related to fundamental clinical training: (1) “relationships with teachers and clinical ” (2) “lack of knowledge and skills,” (3) “reflecting on patient-care experiences,” (4) “relationships with patients, families, and healthcare staff,” (5) “conferences,” (6) “peer relationships,” and (7) “daily planning in clinical practice.” The reliability of these factors was verified based on Cronbach’s alpha (0.84 overall, from 0.62 to 0.85 separately).
Previous studies have identified stress factors in nursing students during clinical training such as insufficient knowledge or skills, clinical practice logs, relationships with clinical instructors and faculty members, and relationships with patients [19,21-23]. The present study found similar trends as well as a more subdivided structure of clinical training-related stress factors. Notably, we identified two stress factors (i.e., “conferences” and “peer relationships”) not reported in previous studies on nursing students at vocational schools, suggesting that these stress factors are unique to nursing students at a university. Moreover, stress related to clinical practice logs was divided into two categories: “daily planning in clinical practice” and “reflecting on patient-care experiences.”
Therefore, orientations before clinical training should be redesigned to address the additional items identified in this survey as causing high levels of stress such as conference procedures and reflecting on patient care.
4.2 Relationship between stress factors and coping behaviors
We used partial correlation analysis to examine the relationship between stress factors and coping behaviors while controlling for SOC score, a confounding variable. Results showed that students with higher scores for the stress factor “relationships with teachers and clinical instructors” were less likely to engage in the coping behavior “changing mood.” Masamura et al. [8] reported that nurses’ relationships at the clinical practice site were a source of stress for nursing students (Table 4). Students had only limited contact with clinical instructors or faculty members, and they felt stress because they could not contact their clinical instructors whenever they neededdebriefing or guidance. Not only were students with higher stress levels in “relationships with teachers and clinical instructors” less likely to engage in the coping behavior “changing mood,” but they also resulted in students having too much to do. Therefore, faculty teachers and clinical instructors must actively engage with students to give them needed debriefing and guidance.
This study revealed that three stress factors, namely, “lack of knowledge and skills,” “reflecting on patient-care experiences,” and “conferences,” were negatively related to the coping behavior “seeking help to solve problems.” A previous study found that students with high SOC were more likely to proactively solve problems or change their perspective to cope with stress related to clinical training, whereas students with low SOC used avoidance strategies such as giving up [20]. However, regardless of whether SOC was high or low, we found that those stress factors were negatively related to the coping behavior “seeking help to solve problems.” For students who use avoidance strategies during clinical training, problems can become even more entrenched if they remain ignorant of the things they should know as they continue their clinical practice. Therefore, faculty members or clinical instructors supervising on wards must support their students by having them reflect on their actions daily to bring awareness to issues they do not understand or by presenting their students with other strategies useful for resolving their issues. Moreover, preliminary reviews must be considered to address students’ insufficient knowledge and skills.
5. Study Limitations
The present study has several limitations. First, our findings were based on a survey at a single institution. As a result, our conclusions cannot be generalized to other populations. Second, the survey used unique survey items on clinical training-related stress created by our research group based on previous studies assessing stress factors. Therefore, the reliability and validity of these survey items will need to be verified based on a larger amount of data in a future study. Third, the cross-sectional design of our study does not allow us to draw any conclusions on causality.
6. Conclusion
We clarified seven factors of clinical training-related stress such as “relationships with teachers and clinical instructors,” “lack of knowledge and skills,” “reflecting on patient-care experiences,” “relationships with patients, families, and healthcare staff,” “conferences,” “peer relationships,” and “daily planning in clinical practice.”We found that high stress due to “relationships with teachers and clinical instructors” was more likely to reduce the occurrence of the coping behavior “changing mood.” In addition, three stress factors (i.e., “lack of knowledge and skills,” “reflecting on patientcare experiences,” and “conferences”) were negatively related to the coping behavior “seeking help to solve problems.” Faculty teachers and clinical instructors need to actively engage with their students to provide debriefing and guidance, as well as encouragement to reflect back on their daily actions. Moreover, orientations before clinical training should be redesigned to address conference procedures and reflection on patient care.
Competing Interests
The authors have declared that no competing interests exist.
Author Contributions
All the authors substantially contributed to the study conception and design as well as the acquisition and interpretation of the data and drafting the manuscript.
Acknowledgments
We would like to extend sincere appreciation to the nursing students who participated in the study.