


1. Introduction
Oral mucositis is one of the most uncomfortable and common complications in cancer patients who receive chemotherapy [1]. Pain due to mucositis influencess swallowing and mastication, resulting in subsequent malnutrition or dehydration. Bacterial infection of injured oral mucosa may cause the invasion of bacteria into the blood stream. Dose reduction or treatment schedule modification may be necessary when severe oral mucositis develops. Moreover, oral mucositis begets excess costs for supportive care and hospitalization on cancer patients receiving chemotherapy.
Currently oral mucositis is considered to take place in five different phases Initiation, Message generation, Signaling and amplification, Ulceration, and Healing [2]. In the initiation phase, mucosal epithelium, vascular endothelium and connective tissues exposed to anticancer drugs release free radicals. These free radicals not only cause direct tissue injury but also initiate a biological cascade. In the message generation phase, activated transcription factors such as NF-κB upregulate genes that control synthesis of biologically active proteins including pro-inflammatory cytokines. Anticancer drugs are also capable of activating enzymes that increase the rate of apoptosis. The production of these proteins results in the damage and death of mucosal epithelium, hence making oral mucosa thin and erythematous. Many of these proteins simultaneously enhance message generation and then mucositis proceeds to signaling and amplification phase. For example, tumor necrosis factor-alpha (TNF-α) -whose level is increased as a consequence of NF-κB activation in message generation- amplifies NF-κB activation in addition to direct tissue injury. In turn, NF-κB activation leads to further production of pro-inflammatory cytokines. Consequently, tissue injury continues to occur beneath the mucosal surface, even after chemotherapy has been completed. Increased vascular permeability induced by inflammation also enhances cytotoxicity of anticancer drugs [1]. In ulceration phase, tissue injury reaches a climax; the integrity of oral mucosa is lost, followed by stimulation of exposed neuronal endings, which creates clinically significant pain, and colonization of oral resident bacteria on the ulcerated surface. Furthermore, colonized bacteria release cell wall products that penetrate adjoining tissue and stimulate inflammation. When patients have neutropenia, bacteria invade into blood vessels and in the worst-case scenario it results in bacteremia or sepsis. Finally, in the healing phase, proteins that promote migration, proliferation and differentiation of immature cells at the border of the ulcer are released from the extracellular matrix and oral mucositis is eventually healed.
In 2004, the first evidence-based clinical practice guidelines for the management of mucocitis were published [3]. The guidelines addressed the importance of basic oral hygiene and oral care protocols in maintaining mucosal health and function. Although specific agents or approaches used in oral care protocols had insufficient evidence to support the guidelines, a lot of attempts, (e.g. topical application of growth factors [4] and agents with anti-inflammatory [5]. Or antimicrobial effects [6]) have been made to manage chemotherapyinduced oral mucositis. After the publication of the guideline, the efficacy of many agents, such as herbal medicine [7], palifermin [8], honey and its mixture of beeswax and olive oil- propolis [9], or supersaturated calcium phosphate oral rinse [10], for the prevention and treatment of oral mucositis have been evaluated since management of chemotherapy-induced oral mucositis is an very important issue in oncology nursing.
The authors have been investigating the effect of the application of sesame oil on the oral care of elderly individuals. As anti-inflammaroty [11,12] and antioxidant effect [12, 13] of sesamne oil, or sesamin, one of its lignans, and antimicrobial effect of fatty acids contained in sesame oils [14] have been reported, it is suggested that sesame oil might be also effective for the prevention of chemotherapy-induced mucositis. Sesame oil is particularly suitable as a natural treatment in oral care because it is widely used as cooking medium in many Asian countries, including Japan. So, it can be used as a readily available ‘home remedy’ for preventing/containing the development of mucositis. Some Japanese nurses have practically used sesame oil in three cancer patients receiving chemotherapy and reported that development of mucositis was prevented in all of them [15].
In the present study, the authors report the results of topical sesame oil application in seven hematopoietic cancer patients.
The distinct cerebral activation was observed during low-level laser acupuncture (continued wave and 10 Hz-modulated wave stimulation) at KI1 of the left foot in healthy right-handed volunteers [14]. Most of the activated areas, observed by functional magnetic resonance imaging, were involved in the functions of memory, attention, and self-consciousness. The cerebral hemodynamic responses to two laser acupuncture stimulation modes and its mechanism is based on not only afferent sensory information processing but also alteration of hemodynamic properties during external stimulation.
2. Materials & Methods
2.1 Subjects
Eleven patients who had been admitted to the general hospital for the chemotherapy of hematopoietic cancer received an explanation of the study and those whose consents were obtained participated in the study.
2.2 Materials
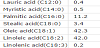
Sesame oil of Japanese Pharmacopoeia grade (Nikko Pharmaceutical, Japan) was used for application. Table 1 shows the fatty acid composition of sesame oil [16].
2.3 Procedure
Seven subjects used sesame oil in addition to their ordinary oral hygiene (Sesame oil group). Sesame oil was applied for 14 days by swabbing with cotton swab more than 3 times a day after ordinary oral hygiene, such as gargling or tooth brushing. Subjects in Sesame oil group received detailed explanation and demonstration of the procedure of sesame oil application (Figure 1). Application was started on the previous day of the beginning of chemotherapy. Subjects in Sesame oil group were asked to record the following data:
- How many times they applied sesame oil and
- How many times performed ordinary oral hygiene.

Four hematopoietic cancer patients who received chemotherapy during the same period acted as controls (Control group). Subjects in Control group were asked to perform ordinary oral hygiene and to record the number of oral hygiene.
2.4 Evaluation
Information of age, sex, diagnosis, chemotherapy regimen and clinical data of the subjects were obtained from the medical records.
The effect of sesame oil application was evaluated by objective and subjective symptoms, grading of mucositis and cytological evaluation of swabbed oral mucosa. In addition subjects of Sesame oil groups answered to the questionnaire about their impressions on sesame oil application.
Objective and subjective symptoms: Oral cavities of the subjects were observed and recorded once a day by the researcher. Subjects were also asked to record subjective symptoms.
Grading of mucositis: Results of the objective and subjective symptoms were graded according to the grading scale of Mucositis/ stomatitis of Common Terminology Criteria for Adverse Events (CTCAE), v3.0 (Table 2) [17].

Cytological examination: Samples for cytological examination of both Sesame oil and Control group were obtained on Day 14 by swabbing the oral mucosa with sterilized cotton swab. Samples were spread on glass slide and fixed immediately with ethanol. Fixed samples were then stained with Papanicolaou’s stain solution. Each sample was examined by qualified cytologist who was blinded about the sample source. The samples were examined according to the following criteria [18]:
- Inflammatory change: (- )No inflammation; (±) very small number of inflammatory cells are observed; (+) Inflammatory cells are observed in less than one third of the fields: (++) Inflammatory cells are observed in more than one third of the fields; (+++ ) Severe inflammatory changes are observed in all fields
- Bacterial contamination: (-)No bacterial cell are observed ; (±) very small number of bacterial cells are observed; (+) Bacterial cells are observed in several fields: (++)Bacterial cells without prominent colony formation are observed in entire background.; (+++ ) Bacterial cells with prominent colony formation are observed in entire background.
Questionnaire: Subjects of Sesame oil group answered a short questionnaire about their impressions on sesame oil application.
2.5 Statistical analysis
Average age, lowest leukocyte count, highest CRP value and mucositis grade of Sesame oil group and Control group were compared by Student’ s t test. Chi squared test was used for the comparison of cytological evaluation. P values of < .05 were considered statistically significant. IBM SPSS Statistics version 19 was used for statistical analysis.
2.6 Ethical consideration
The study was approved by Ethical Committee of both Graduate School of Nursing, Chiba University and the research facility.
3. Results
3.1 Outline and general status of the subjects
Table 3 shows the outline of the subjects. 4 of 7 subjects in Application group and 3 of 4 subjects in Control group were the patients with acute myelogenous or lymphatic leukemia. Additionally, 3 of 7 subjects in Sesame oil group and 1 of 4 subjects in Control group were the patients with non-Hodgkin lymphoma. Mean age was 63.7 (range 31 to 87) in Sesame oil group and 57.5 (range 43 to 74) in Control group respectively and there was no significant difference. Regimens and phases of chemotherapy differed among the subjects. Methotrexate (MTX), cyclophosphamide(CPA), doxorubicin and etoposide which have higher risks of oral mucositis [19, 21] were administrated to 5 subjects in Sesame oil group (Subject A, C, D, F, G) and 2 subject (Subject H, I) in Control group. High dose of MTX or CPA and doxorubicin were administrated to one subjects of each group (Subject G in Sesame oil group and subject H in Control group).

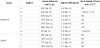
Lowest leukocyte count, highest CRP value and number of the episodes of fever over 37.5°C were summarized for each subject (Table 4). After the beginning of chemotherapy, leukocyte count started to decrease and consequently leukocytopenia was observed in most subjects (5 of 7 subjects in Sesame oil group and all subjects in Control group, respectively). Leukocyte count showed the lowest value 7 to 14 days after the beginning of chemotherapy. It fell below 1000/μL in 3 of 7 subjects in Sesame oil group and 2 of 4 subjects in Control group. In 2 subjects in Sesame oil group and 1 subject in Control group, the lowest white blood cell count was below 500/μL. No statistical difference was found in both lowest leukocyte count and highest CRP value.
Elevated CRP value over 2 mg/dL which indicates more than moderate inflammation was also observed in 5 subjects of Sesame oil group and 3 subjects of Control group. 2 subjects in Sesame oil group showed fever over 37.5°C. However, no symptoms were caused by sesame oil application.
3.2 Changes in oral mucosa
4 of 7 subjects in Sesame oil group had to stop application of sesame oil due to fever (Subject B, from Day 3 to 5), severe fatigue (Subject E, from Day 2 to 8; Subject G, Day 5), or discharge (Subject C, Day 10). The rest 3 could continue to apply sesame oil to their oral cavity more than 3 times throughout 14 days. Additionally 2 subjects (Subject A, from Day17 to 37; Subject F, from Day 15 to 25) continued sesame oil application after Day 14 since they wished to continue it.
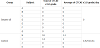
Table 5 shows total and average CTCAE v3.0 grade of each subject during 14 days. None of the subjects of Sesame oil group had developed oral mucositis while they used sesame oil for their oral care. Mucositis of grade 1 appeared in Subject A on the next day of the termination of sesame oil application. His regimen included MTX, an aniticancer drug with higher risk of oral mucositis. He started applying sesame oil again on Day 17. Three days after he restarted the application, his mucositis was healed. He continued the application until Day 37. However, on the next day of the last application of sesame oil mucositis reoccurred in his mouth.
In Control group, oral mucositis was observed in 2 subjects (Subject H, I). Mucositis of grade 1 developed in Subject H on Day 4.Although it disappeared by gargling with sodium gualenate solution, uncomfortable feeling in oral cavity still continued and mucositis occurred again on Day 7. Mucositis continued to worsen and consequently CTCAE v3.0 grade also increased from grade 1 to 3 after Day 12. Subject I already had 2 lesions of oral mucositis of grade 1 before chemotherapy; one more lesion developed after chemotherapy started. Anticancer drugs with high incidence of oral mucositis were included in the regimen of both subjects (CPA and doxorubicin for subject H and etopside for subject I)
However, no statistical significance was found between CTCAE v3.0 grades of Sesame oil and Control group.
3.3 Cytological examination
Figure 2 shows the results of cytological examination of Sesame oil group and Control group on the previous day of chemotherapy (Day 1) and 14 days after chemotherapy started (Day 14).
After 14 days, in Sesame oil group, grade of inflammatory change improved in 3 subjects (Subject A, B, F), remained unchanged in 3 subjects (Subject C, E, G) and worsened in 1 subject (Subject D). In case of Control group, although grade of inflammatory change worsened in all subjects, but no statistical significance was found (Figure 2A).
Grade of bacterial contamination was observed to have increased in 2 of 7 subjects (Subject B, G) in Sesame oil group. In the other subjects, it was unchanged (Subject A, C, D, E, F). In Control group, grade of bacterial contamination worsened in 1 subject (Subject I), remained unchanged in 2 subjects (Subject J, K) and decreased in 1 subject (H) (Figure 2B).

3.4 Questionnaire
Figure 3 shows the impressions of the subjects in Sesame oil group about sesame oil application. 5 of 7 subjects who had experienced mucositis in previous chemotherapy session felt that sesame oil was effective in preventing oral mucositis. Subject also answered that sesame oil was effective in preventing dry mouth (4 subjects) and tongue coat (2 subjects), and in increasing saliva secretion (2 subjects). All subjects in Sesame oil group told that they would use sesame oil again when they received the next chemotherapy.

4. Discussion
In the present study, topical application of sesame oil seemed to be useful for the management of chemotherapy–induced oral mucositis because of lower incidence of mucositis and lower grade of inflammatory cells in Sesame oil group although no statistical significance was found between Sesame oil group and Control group. Anticancer drugs with higher risk of development of oral mucositis were included in the regimen of 4 subjects in Sesame oil group and 2 subjects in Control group, respectively. Moreover, high dose of MTX or CPA and doxorubicin were administrated to one subjects of each group. Oral mucositis occurred in only one patient in Sesame oil group whereas it developed in both of the two subjects who received chemotherapy regimen with higher risk of oral mucositis.
The clinical course of subject A in Sesame oil group who developed oral mucositis immediately after the termination of sesame oil application suggests the effectiveness of sesame oil application for the prevention of oral mucositis. Since his mucositis was healed after restarting of sesame oil application, sesame oil might also be useful for the treatment of oral mucositis.
It is possible to explain the mechanisms by which topical application of sesame oil prevented oral mucositis based on its pathophysiology. As previously mentioned, release of free radicals by anticancer drugs is the trigger of upregulation of genes coding biologically active proteins including pro-inflammatory cytokines. Sankar et al examined the plasma of the hypertensive patients who were fed sesame oil for 45 days. They found decrease in lipid peroxidation (thiobarbituric acid reactive substances; TBARS) and increase in the activities of erythrocyte superoxide dismutase and reduced glutathione [13]. Therefore, it is suggested that released free radicals become detoxified by superoxide dismutase activated by sesame oil.
Anti-inflammatory effect of sesame oil also may contribute to the prevention and healing of oral mucositis. Inflammation in oral mucosa caused by upregulation of genes regulating synthesis of proinflammatory cytokines caused by activation of NF-κB is a critical event in message generation and signaling and amplification phase. Cui et al reported that sesamin treatment inhibited the activation of NF- κB induced by bacterial chemotactic peptide in human monocytic cells. Results of cytological evaluation that inflammatory change was reduced in Sesame oil group support anti-inflammatory effects of sesame oil.
It should be also emphasized that topical application of sesame oil was incorporated into oral care protocol in the present study. Subjects were asked to apply sesame oil after ordinary oral hygiene, such as tooth brushing and gargling. Importance of basic oral hygiene and oral care protocols in maintaining mucosal health and function has already been mentioned in the guideline while basic oral hygiene alone cannot prevent oral mucositis [3]. As leukocytopenia, especially decrease in nutrophil is inevitable in most patients receiving chemotherapy and neutrophil plays an essential role in the defense against bacteria, prevention of excessive proliferation of oral resident bacteria in neutropenic patients is extremely important in avoiding the formation of severe oral mucositis. Here, the antimicrobial activity of fatty acids in sesame oil also helps.
In addition, topical sesame oil application is easy. It can be performed by patients themselves, and saves costs. No prescription is necessary. Taste and mouth feel is acceptable even in the patients who may have nausea because of chemotherapy. More than anything, it is noteworthy that all subjects of Sesame oil group desired continuation of sesame oil application.
Due to small number of subjects and variety of the regimen, the results of this study are not sufficient enough to support the effectiveness of sesame oil. A randomized controlled study with a large sample size is necessary to provide reliable evidence of effectiveness of topical sesame oil application for the management of oral mucositis.
5. Conclusion
The effectiveness of topical sesame oil application for the prevention of chemotherapy- induced oral mucositis was tested on 7 hematopoietic cancer patients. Their incidences and grades of oral mucositis were lower than that of controls. Cytological examination revealed that inflammatory change was reduced in sesame oil application group. Topical application of sesame oil was suggested to be useful for the prevention of chemotherapy-induced oral mucositis.
Competing Interests
The authors declare that they have no competing interests.
Author Contributions
All authors substantially contributed to the study design, collection and interpretation of data, and drafting the manuscript.