


1. Introduction
Professional behaviors that contribute to nursing professionalism are considered an essential component of nursing leadership within a global context. The importance of developing global knowledge has been recognized in nursing, and because many healthcare issues cross international borders, the need for a global exchange of knowledge and evidence is greater than ever [1]. Many international nursing research studies have been conducted; however, there are no international studies that compare nursing professionalism across countries. Little is known about the levels of nursing professionalism from the global point of view.
The purpose of the present study was to investigate and compare nursing professionalism among nurse leaders in the United States of America (U.S.A.) and Japan. Each of the nursing professional behaviors was investigated with self-reported survey, and the results by country were compared and discussed.
2. Background
Nursing professionalism has been demonstrated by attitudes, knowledge, and behaviors that reflect a multifaceted approach to the regulations, principles, and standards underlying successful clinical practices [2]. Hall described five attributes of professionalism: 1) using a professional organization as major referent, 2) belief in public service, 3) belief in self-regulation, 4) a commitment to the profession beyond economic incentives, and 5) a sense of autonomy in practice [3]. Miller developed the Wheel of Professionalism in Nursing Model to demonstrate that a scientific background is critical for professionalism in nursing [4]. In the model, education in a university setting and scientific background in nursing appear in the center of the wheel. The spokes of Miller’s wheel depict eight additional characteristics that define professionalism in nursing: 1) publication and communication; 2) research development, use, and evaluation; 3) participation in professional organizations; 4) community service orientation; 5) competence and continuing education; 6) theory development, use, and evaluation; 7) self-regulation and autonomy; and 8) adherence to the American Nurses Association (ANA) Code of Ethics. According to Rutty, the nursing profession is characterized by a defined knowledge base, power and authority over training and education, registration, altruistic service, a code of ethics, lengthy socialization, and autonomy [5].
The development of nursing professionalism has made considerable progress in the U.S.A. The nursing practice act now allows for more expanded nurse roles, and the ANA has worked to enhance the status of professional nurses. The development of doctoral programs in nursing at major universities has increased the number of qualified and dedicated nursing leaders across the U.S.A. [6]. One area in which great strides have been made since the 1960s, most notably in the 1980s and 1990s, is the growth of advanced practice registered nurses (APRNs). Nurse anesthetists, nurse-midwives, clinical nurse specialists, and nurse practitioners are now qualified as APRNs. As such, these nurses practice with autonomy, authority, and responsibility [7]. An estimated 250,527 nurses were classified as APRNs in 2010 [8].
Nursing practices in Japan have been adapting to Western nursing style, but the improvement in nursing professionalism is behind that found in the U.S.A. [9]. Nursing autonomy is limited by the Japanese Nursing Law, which legally requires that nurses’ work only be performed under medical doctors’ orders [9]. Feminist issues also remain in Japan, so traditional professions for women have a negative stigma. Decreasing the gender-stereotype of nursing is required to promote nursing professionalism in Japan [10]. Certified nurse specialists were first introduced to Japan in 1996 and have increased in number, yet comprise only 0.06% of the nursing population in Japan [11]. Nursing education differs greatly between the U.S.A. and Japan, where nursing is less well developed and preregistration programs remain at the diploma level, delivered primarily by Schools of Nursing attached to hospitals in Japan [9]. To reduce traditional and cultural barriers in nursing professionalism, the Japanese Nursing Association (JNA) has worked toward enhancing nursing standards. The Act on Public Health Nurses, Midwives and Nurses and other lawmaker-initiated amendments states that graduation from a fouryear college is now a prerequisite for taking the nurse’s examination [11]. However, there are a limited number of re-entry study programs for RNs who have a diploma or associate degree [12]. Moreover, no measurable tools exist to assess the behaviors that contribute to nursing professionalism [13]. Behaviors relevant to nursing professionalism in Japan need further investigation.
3. Method
Although various professional behaviors are proposed to contribute to professionalism, Miller’s Wheel of Professionalism in Nursing Model and its corresponding inventory, the Behavioral Inventory for Professionalism in Nursing (BIPN), were chosen as a theoretical framework for this study. Miller’s Wheel of Professionalism in Nursing Model is a well-known model in nursing, and the BIPN is one of the few instruments used worldwide to measure nursing professionalism [14].
This study used a descriptive design with cross-cultural comparative to understand and compare differences in the current status of nursing professionalism among nurse leaders in the U.S.A. and Japan.
3.1 Participants and procedures
In this study, “nurse leader” was defined as a nurse who has a leadership role, such as clinical manager, nursing supervisor, clinical director of nursing, nurse administrator, advanced practice nurse, and nursing faculty. The inclusion criteria were a nursing license, a baccalaureate degree or higher, and having a leadership position in a healthcare environment.
The BIPNs were distributed from 2007 to 2011. A snowball sample in the U.S.A. was drawn from Southern California. The survey was distributed to nurse leaders who graduated from a state university with a Master of Science in Nursing Administration degree, and to attendees at meetings of the Association of California Nurse Leaders. Of the 247 BIPNs distributed, 142 were completed and returned, yielding a 59% response rate. Sixteen surveys were excluded owing to incomplete information and unsuitable inclusion criteria, so 126 surveys from the U.S.A. were included in the analysis.
In Japan, 2,972 BIPNs were distributed to a random sample as a national survey. Using statistical software, 44 hospitals were chosen randomly from the 353 hospitals in Japan. A total of 1,846 respondents returned surveys from 25 hospitals in the random sample, yielding a 62.1% response rate. Of those returned, 123 surveys were excluded owing to incomplete information. Nurse leaders were extracted from the returned surveys according to study inclusion criteria, resulting in 182 acceptable surveys from Japan for inclusion in the analysis.
This study was approved by the Institutional Review Board of California State University (Fullerton, California) in the U.S.A., and the Kyushu University Institutional Review Board for Clinical Research in Japan.
3.2 Instruments
The BIPN measures the degree of nursing professionalism within the past two years through dichotomous responses to 48 items. The BIPN weightings for specific behaviors within each of the BIPN’s nine categories equal 3; thus, a total composite score of 27 is possible. The nine categories correspond with the attributes of Miller’s Wheel of Nursing Professionalism in the Nursing Model previously described. Higher mean scores indicate more professional behavior. Reliability and validity of the BIPN were established by previous studies [4,15]. Permission to use the BIPN was granted by Dr. Adams at Arizona State University. The Japanese version of the BIPN was translated using the back-translation method. Reliability and validity of the Japanese version of the BIPN has been established by a pilot study in Japan [13].
3.3 Data analyses
The total mean score and each subscale score of professionalism are presented as means and standard deviations. These scores were compared by groups using t-tests. The Chi-square test was performed to evaluate the degree of professional behaviors between the countries, and Fisher’s exact test was used to confirm the p-value. The degree of significance for the calculation was chosen as α = .05, and a calculated p-value < .05 was considered significant. All analyses were carried out with the Statistical Package for JMP® 9 software (SAS Institute Inc., Cary, NC).
4. Results
4.1 Demographic characteristics
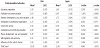
A total of 308 nurse leaders completed the study (126 from the U.S.A. and 182 from Japan). The majority of the sample (94%) was female. There was cultural difference in that all nurses in the sample from Japan worked in a single workplace full-time, whereas 7.3% of nurses in the U.S.A. worked in more than one workplace, balancing full-time and per diem work. Nurse leaders in the U.S.A. were highly educated and experienced: 69.8% had a master’s degree, and 75.6% had more than 21 years of nursing experience. In comparison, 41.2% of nurse leaders in Japan had a master’s degree, and 47.5% had more than 21 years of nursing experience. There were no differences in gender owing to the low quantity (5.55%) of male participants in the sample. As shown in Table 1, there were differences in age, current position, current practice setting, educational preparation, and years of nursing experience between nurse leaders in the U.S.A. and Japan (p < .0001).

4.2 Professional behaviors
The mean total score of professionalism was significantly different between the two countries (15.07 and 12.63 in U.S.A. and Japan, respectively; t=4.845, p<.0001). Significant differences were alsorevealed in the following subscales of professionalism: education preparation (t=3.559, p<.0001), publication and communication (t=−2.691, p=.008), research development (t=−2.336, p=.02), community service (t=9.232, p<.0001), theory development (t=8.426, p<.0001), and self-regulation and autonomy (t=9.008, p<.0001) (Table 2).

A detailed comparison of professional behaviors according to the BIPN subscales is presented in Table 3. The professional behavior publication and communication was more prevalent among nurse leaders in Japan compared with the U.S.A. Japanese nurse leaders submitted more (χ2=3.89, p<.05) and published more (χ2=12.50, p<.0001) manuscripts than their U.S.A. counterparts. Japanese nurse leaders also engaged in more proposal writing within research development than nurse leaders in the U.S.A. (χ2=23.22, p<.0001). The professional behavior community service showed a significant difference (p<.0001) between the two countries: the U.S.A. nurse leaders reported more professional behaviors (e.g., participating in community services and serving on a community advisory board) than their Japanese counterparts. Significantly more professional behaviors related to theory development were reported in the U.S.A. than in Japan (p<.0001); the exception was the application of nursing theories in practice (p=.274). Additionally, six of the 10 professional behaviors related to self-regulation and autonomy were significantly more common among nurse leaders in the U.S.A. compared with Japan: quality assurance (χ2=17.23, p<.0001), peer review (χ2=29.49, p<.0001), consultation (χ2=17.20, p<.0001), budgeting (χ2=66.34, p<.0001), performance evaluation (χ2=31.02, p<.0001), and hiring personnel (χ2=86.66, p<.0001). There was no significant difference in nurse leaders’ adherence to the ANA Code of Ethics.
5. Discussion
The details of each professional behavior are discussed in this section.
5.1 Publication and communication
Nurse leaders are active in disseminating knowledge with colleagues through publications [16]. The knowledge and skills necessary for contributing to publications are acquired in doctoral degree programs. Because the percentage of nurses with doctoral degrees was less than 15% in each country, the mean total score of publication and communication was low. Within the past two years, 33.5% of the participants from Japan had published in a nursing journal, whereas only 15.9% of nurse leaders in the U.S.A. published during the same time period. The difference may have been affected by the number and quality of nursing journals, which differ considerably between the two countries. Nursing journals in the U.S.A. have been active since the 1960s, using rigorous peer review to discuss evidenced-based nursing. In contrast, there are only two Japanese nursing journals with an impact factor to date, and few peer-reviewed journals are available in Japan. That is, Japanese nursing journals are open to all nurses to publish case reports, commentaries, or research at any scientific level.
5.2 Research development, use, and evaluation
Involvement in research is a characteristic of professionalism in nursing [17]. Nursing research is essential for the development of scientific knowledge, and nurses are accountable to society for providing evidence-based practice [16]. The findings indicated that more nurse leaders in Japan had attended a workshop, seminar, or course concerning research, wrote a proposal, or participated in a research study in the past two years compared with nurse leaders in the U.S.A. The demographics of our samples from the U.S.A. and Japan likely influenced the result for this characteristic because more than 30% of the participants from Japan were school faculty for whom research activity is required.
5.3 Competence and continuing education
In the nursing profession, as in many professions, continuing education is frequently identified as a necessary component of professional competence [14]. Participating in continuing education promotes new knowledge and skills, keeps a nurse informed of new trends that may have an impact on nursing practice, and improves confidence among nurse leaders [18]. Although Japanese nurses are not required to renew nursing licenses, there was no significant difference in the professional behavior of competence and continuing education between nurse leaders in the two countries.
5.4 Participation in professional organization
Joining professional organizations can contribute to career development, updating of professional issues, an increase in skillbuilding and professional networking opportunities [19]. The ANA is the primary organization that advances the nursing profession [20]. Similarly, the Japanese Nurses Association (JNA) is the primary organization for Japanese nurses. JNA upholds nursing standards in Japan through organizing support activities for members and undertaking initiatives to address challenges in the areas of public health, medical care and social welfare [11]. In the present study, more than 60% of participants from both countries were involved in one or more nursing professional organizations. Thus, it was apparent that nurse leaders recognized the importance of professional organizations; however, the way to participate differed between the two countries. Only 11.9% of U.S.A. participants were current members of the ANA, whereas 96.2% of nurse leaders in Japan belonged to the JNA. The U.S.A. nurse leaders reported membership in professional organizations specific to their positions/specialties; 73% were members in a nursing organization other than the ANA, demonstrating they value participation in professional organizations.
5.5 Community service orientation
Professions exist for meeting the needs of society [21]. Serving one’s community demonstrates a nurse leader’s willingness and commitment to share knowledge and assist in healthcare decisionmaking, and community service furthers a nurse leader’s professional development. In the U.S.A., in-service programs combine instruction with community service, resulting in meaningful contributions to the community [22]. Conversely, Japanese nurse leaders had low levels of involvement in community service. To improve professionalism, Japanese organizations could provide community service programs for nurses.
5.6 Adherence to the ANA Code of Ethics
The Code for Nursing is the pledge to the public that promises the highest standards of nursing practice; therefore, adherence to the Code for Nursing is a primary requirement of professionalism. There were no significant differences between nurse leaders in U.S.A. and Japan regarding adherence to the Code for Nursing. A code of ethics should be integral to nurse leaders to create a strong sense of professionalism [23]. The JNA adapted the Code of Ethics for Nurses in 1988, and it clearly stated the scope of the responsibilities that nurses should take as professionals in practicing nursing in Japan [11]. The Code should be considered a framework for professional practice; however, adhering to the code in practice may be difficult for less-experienced nurses [24]. Nurse leaders need to make sure that less-experienced nurses integrate the Code of Ethics for Nurses into their practice.
5.7 Self-regulation and autonomy
Autonomy, the condition of being independent and having responsibility, authority, and accountability, is an essential component for professional practice [25]. Nurses at the master’s level have demonstrated the highest scores in autonomy, and nurses in administrative roles showed clear role expectations and correspondingly higher scores on autonomy [23]. All of the autonomous behaviors examined demonstrated high involvement among nurse leaders in the U.S.A. Six of the nine behaviors were significantly higher in the U.S.A. than in Japan, reflecting advanced nursing autonomy in the U.S.A. and limited nursing autonomy in Japan. Drennan found that a master’s degree in nursing plays an essential role in providing effective leadership, which relates to autonomy [26]. In recent years, clinical nurse leaders with a master’s degree have been recognized as advanced nurse generalists. This role requires in-depth knowledge of management, leadership, evidence-based practice, risk appraisal, and outcomes analysis, and is accountable for providing high-quality care [27]. Because education preparation differences affect the levels of nursing professionalism, it is critical to develop various educational programs for nurses, and to provide encouraging environments for obtaining higher degrees [12].
5.8 Theory development, use, and evaluation
The ability to generate and apply theory forms the legitimacy of any profession [28]. Theories clarify and define nursing, and the purpose of nursing theory is to distinguish it from other caring professions. The importance of theory in nursing is that it offers structure and organization to nursing knowledge [29]. Nursing practice, therefore, occurs within a large context and framework that is shaped by theories [30]. In the present study, professional behaviors related to theory were higher among nurse leaders in the U.S.A. compared with Japan. These results show that the U.S.A. nurse leaders have been exposed to the importance of theories to nursing practice and are practicing within a theoretical framework. In contrast, few curricula for nursing students related to nursing theory are available in Japan. Rather, practical skills are the focus. A theory-practice merger in nursing has been considered globally [31]. To improve theoretical behaviors, it is critical to succeed in bridging the gap between theory and practice in Japan.
6. Limitations
A limitation of this study is the generalizability of its findings. The sample of nurse leaders in the U.S.A. was nonrandom (only from Southern California). Participants from other settings are necessary to increase the diversity of participants and to expand the generalizabilityof findings in the U.S.A. Another limitation is the four-year data collection period. A third limitation relates to the challenge of engaging in cross-cultural research, specifically the issue of equivalence of concepts of professionalism. The professional constructs may not translate equally across the backgrounds and cultural boundaries of the two countries. However, the same emphasis and importance are placed on professionalism in nursing in the two countries [12]. Further exploration of the leader role in the profession of nursing in both countries is needed to improve nursing professionalism among these populations.
7. Conclusion
International collaboration in nursing research is important to exchange evidence at the global level. To the best of our knowledge, no previous study has compared nursing professionalism among nurse leaders from the U.S.A. and an Asian country. It is acknowledged that nursing professionalism in the U.S.A. and Japan are at different levels of development. The present findings extend our understanding of the behaviors that contribute to nursing professionalism in differing cultural contexts, and they provide a rare direct comparison of nursing professionalism between the U.S.A. and Japan for future transcultural comparisons. Nurse leaders in both countries are expected to exhibit high levels of professionalism, are well equipped to serve as role models, and can absorb good practice from international colleagues to improve nursing professionalism. Overall, we hope that this study opens the door to further international comparative studies of nursing professionalism.
Competing Interests
The authors declare that they have no competing interests.
Author Contributions
All the authors equally contributed to intellectual content of the manuscript as well as proposal of design, data collections, data analysis, and drafting the manuscript.
Acknowledgments
We thank all the nurses who participated in this study for their contribution and dedication.