


1. Introduction
1.1 Statement of the problem
Cardiovascular disease (CVD) is the main cause of mortality and a leading cause of disability among men and women in the United States (US). The most recent statistics show that CVD accounted for 32.8% (almost 812,000) of all US deaths [1]. This implies that more than 2200 Americans die of CVD each day, or that one death from CVD occurs almost every 40 seconds. Each year, nearly 800,000 Americans experience a new myocardial infarction (MI) and approximately the same number experience a new or recurrent stroke [1]. CVD is present in approximately one-third of all US adults and imposes a large financial burden, which was estimated at $448.5 billion in 2008 [2]. The majority of cardiovascular (CV) events are not limited to the elderly; approximately 150,000 Americans aged 65 years or older died of CVD in 2008 and 33% of CVD deaths occurred in those greater than 75 years. Fifty percent of annual major coronary events are recidivistic and of these, fifty percent are fatal [3]. A continual increase in the prevalence and costs of CVD has been projected as far as 2030 [4]. With these compelling statistics as a backdrop, the purpose of this article is to describe the DIRECT program, identify the gaps in current guidelines and then describe the process by which the DIRECT program was tested with a group of practicing nurse practitioners.
1.2 Atherosclerosis is initially a silent condition
Although the guidelines for treatment are based on risk factor paradigms, plaque in the artery wall is the actual culprit of vascular events [5].The natural progression of vascular disease (atherosclerotic disease) can potentially begin in early adolescence as fatty streaks within the artery wall [6].At the same time, it is important to realize that atherosclerosis and CVD are not inevitable consequences of aging and there are opportunities to intervene early in the disease state and halt the progression of atherosclerosis [7].Gradual, oftensilent expansion of these lesions may eventually limit blood flow in the arteries [8]. However, such slow growing stenotic lesions are not typically the cause of acute CV events; rather, either rupture or erosion of the endothelium overlying an atheroma leads to a thrombus [9].
Often times, the thrombus causes an acute obstruction that result in a symptomatic ischemic event: heart attack or ischemic stroke. If the thrombus is small, it may migrate distally, causing silent ischemia. Additionally, the thrombus may simply heal, leading to progression in the size of the underlying atheroma. This scenario can occur in any artery and eventually present as coronary, renal, intestinal, peripheral, or cerebral disease [10,11].With this understanding of the atherosclerotic disease process, identifying vulnerable plaques that are at high risk for causing a CV event is a critical element for CV risk assessment.
1.3 Exploring the current gap in practice with CV risk factor analysis
Accurate risk assessment is essential in order to ensure patients get the appropriate level of treatment and minimize CVD-related morbidity, mortality and associated health care costs. Appropriate risk assessment is especially important for middle-aged adults, as recent studies show that they are approximately 2 to 3 times more likely to experience a CV event as they are to die from non-CV causes [12]. The current CVD risk categories outlined by the National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP) III and its updates are based on the presence of existing coronary heart disease validated by a previous coronary event or procedure and on the traditional Framingham Risk Score (FRS). Silent, asymptomatic vascular disease is not part of the equation. The FRS components include age, hypertension, smoking and total and high-density lipoprotein cholesterol (HDL-C) levels [8].
Additional risk assessments that have been suggested as supplements to the NCEP ATP III guidelines include the Reynolds Risk Score (RRS) [13], which is another risk algorithm that incorporates FRS factors in addition to family history, the inflammatory marker highly sensitive C - reactive protein (hs-CRP), and glycated hemoglobin levels [14]. The most recent rendition of this risk model paradigm shift the recommendation for statin therapy to lower risk category profiles but fall short to embrace the evaluation of asymptomatic vascular disease or vascular inflammation as a determinant for treatment [15]. However, the absence of such risk factors does not exclude the presence of atherosclerotic plaque, which is a necessary ingredient for a CV event to occur [16].
1.4 Identifying asymptomatic vascular disease
The current literature supports the concept that looking for vascular disease with valid clinical tools and assessing the state of vascular inflammation allows for an improved risk assessment outcome for patients. One of the earliest pieces of research challenging these two paradigms was the work of the 10-year CAFES-CAFES study [5] which 10,000 asymptomatic and low risk FRS patients were evaluated with Carotid and Femoral Ultrasound Morphology Screening at baseline. The degree of atherosclerosis (assessed by carotid-intima media thickness [CIMT]) in low-risk, asymptomatic patients strongly correlated to CV events.
The Society of Atherosclerosis Imaging and Prevention [17] and the Screening for Heart Attack Prevention and Education (SHAPE) Task Force [18] have endorsed the use of CIMT in clinical practice. The CIMT measurement, specifically, offers a practical, noninvasive approach to complement risk factor assessment by identifying subclinical atherosclerosis and carotid plaque formation. Another structural tool that can be utilized to identify asymptomatic disease is the Coronary Artery Calcification Scan, which has been shown to provide superior discrimination and risk classification when added to FRS [19].
Once disease identifying tools are incorporated into clinical practice, CV treatment decisions begin to hinge on the presence or absence of an atheroma rather than simply the absence or presence of a risk factor burden. The ultimate goal of this combined risk assessment approach is to better enable the practitioner to make well-informed therapeutic decisions for each patient. Interestingly, as an additional benefit, structural testing for asymptomatic disease has demonstrated to be a motivator for improvements in patient behaviors [20]. In addition to structure, the current guidelines fail to comprehensively assess the inflammatory state of the arterial system. Inflammation is causal of atherosclerosis [21]. Inflammation is involved in the initiation and progression of atherosclerosis, as well as the provocation of plaque rupture leading to a cardiovascular event [9]. To halt atherosclerosis, clinical identification of the multiple root causes of atherosclerosis and vascular inflammation must be identified. Unfortunately, this evidence based disease/inflammatory clinical paradigm is not a part of the current risk factor clinical guidelines.
The Bale/Doneen Method is the backdrop for which the DIRECT program is established. DIRECT utilizes the Bale/Doneen disease/ inflammatory approach to risk assessment, which has been proven to cause vascular disease regression [22].The DIRECT program utilizes the assessment aspects of the Bale/Doneen Method for the CE portion of the course.
2. The DIRECT Program
The DIRECT program highlighted the scientific evidence that is not included in current guidelines and developed continuing education for primary care nurse practitioners to close the gap in practice related to cardiovascular disease risk assessment. Patients without major CVD risk factors may have clinically silent atherosclerosis that predisposes them to experiencing a CV event. Additionally, advanced prepared nurses have the core competency to integrate organizational science to practice the highest level of nursing practice. Challenging the current risk factor paradigm with the science surrounding asymptomatic vascular disease identification provides an opportunity for improved clinical CV risk assessment. This disease/inflammatory paradigm to CVD prevention aim to provide the evidence-based science to answer this gap in practice for CVD risk assessment.
The purpose of this CE activity was to advance the prevention and screening skills of primary care nurse practitioners. A recent systematic review of 26 studies published over the last 13 years found that health status, treatment practices, and prescribing behavior were consistent between nurse practitioners and physicians [23]. As stated by Cassidy [24], recognizing the upcoming shortage of primary providers in an ageing population, there is a need to innovate with new health care delivery models to meet the demand for primary care to a growing and aging population. The DIRECT program is an innovative, evidence-based approach to tackle the most common disease in this country-cardiovascular disease. This CME activity focuses on screening for CVD in patients seen by nurse practitioners.
Nurse Practitioner autonomous practice policies at the state and national level need to be explored. The DIRECT program will be successful if NPs are allowed to implement the screening procedures and order the inflammatory tests on patients. The Washington State law, WAC 246-840-300, supports that nurse practitioners have the ability to practice without limitations and have full, independent scope of practice. Autonomous NP practice is present in 18 states, including Washington and the District of Columbia. Initially, Alaska, New Hampshire, Oregon, and Washington were the first states to adopt broad autonomy for NPs in the 1980s to answer the increase in demand of primary care providers in rural areas [25]. The Affordable Care Act of 2010 has influenced the states of California, Massachusetts, Michigan, Pennsylvania and New Jersey to consider passing laws related to NP autonomy.
3. Methods
The DIRECT program identified the scientific evidence that is not included in current guidelines and developed continuing education for primary care nurse practitioners to close the gap in practice related to cardiovascular disease risk assessment. The pilot study of the DIRECT program was undertaken to determine if nurse practitioners believed that a disease/inflammatory approach to CVD risk assessment was valuable in their clinical practice. It was also utilized to expose barriers to application of the information learned in the DIRECT program. The course included an analysis and systematic review of the current guidelines for CV risk assessment. DIRECT offered a comprehensive review of the evidence supporting a disease/inflammatory approach to CV prevention. The DIRECT program receivedapproval through the NPGS education committee. The investigator delivered the course to nurse practitioners and performed an analysis of competency of the material along with clinical application of both models to assess clinical decision making differences when NPs utilize the evidence to enhance the current risk factor paradigm that is embraced so readily in current practice. Using the 2006 Essentials of Doctoral Education for Advanced Nursing Practice as a guide, the course effectively illustrated the DNP core competencies through this evidence-based practice model for improved cardiovascular disease prevention. The study received expedited review under the internal review board at Gonzaga University.
This CE course aimed at quality improvement of care and the application of a new care model for nursing practice. The program celebrated the core foundational calling for doctoral prepared nurses to practice the most advanced level of nursing practice, which involves the application of scientific knowledge that is current and transcends specialties for the benefit of optimal health for the patient.
4. Significance of the Project for Nursing and Healthcare
The course was delivered to the Nurse Practitioner Group of Spokane (NPGS) during their regular monthly CE dinner meeting. The course was delivered in power point and open discussion format and the subjects were given worksheets and a written outline of the material. Two cases were presented following the dissemination of the didactic scientific evidence surrounding the disease/inflammatory approach to CVD risk assessment. The cases involved a male and a female patient, each of whom were assessed using the information learned in the DIRECT program and compared and contrasted to a standard assessment with the standard of care. Thirty minutes was allowed for discussion following the formal power point session.
Immediately following the presentation, participants were asked to voluntarily fill out a 20-question survey about their thoughts regarding the information. The questions were rated on a Likert scale model, ranging from strongly agree to strongly disagree. Barriers to practice application also were explored on the form, including autonomy, time with patient, colleague support, access to labs and tests, and understanding of the information. Demographic questions were utilized to perform ANOVA one-tailed t-tests to determine statistical relevance of relationships. Also, each question was analyzed for statistical integrity.
5. Data Analysis and Results
Descriptive statistics were used to determine participants’ demographics and distribution of variables of interest related to the DIRECT program. One and two-sample tests and simple linear regression were utilized to address the study analyses. Twenty-six nurse practitioners voluntarily participated in the DIRECT program. All were members of the NPGS. Eighty-one percent (n = 21) of participants were BSN/RN graduates while nineteen percent (n = 5) were ADN/RN graduates. The majority (84%) of post baccalaureate graduates were ARNP/MSN, 12% were ARNP/DNP, and the remaining 4% Ph.D. The majorities of the participants were female and practiced as an RN for more than 10 years before they obtained their graduate degree as a nurse practitioner (54%). Additionally, most had been in practice for 10-15 years.
Key questions related to the impact of the DIRECT program included the NPs’ perception of the scientific material and the intent of the NPs to utilize the information in practice. Responses were presented in a Likert scale with 1- strongly agree to 5-strongly disagree. The NPs believed that the current standard risk factor model was inadequate for screening for CV risk, determined by stating they disagreed that FRS was adequate to determine risk (M = -4.0, SD = 1.35, t(26), p = 0.000, one-tailed); a disease/inflammatory approach to CVD care is more effective to identify which patients are at risk for a cardiovascular event, (M = 2.00, SD = 1.131, t(25) = -4.507, p = .000, one-tailed); and their practices would greatly be enhanced when cIMT (disease assessment) and inflammatory testing were added (p = 0.000 for both).
The results of this study indicate that the participating NPs wanted to learn more about the scientific evidence surrounding cardiovascular disease prevention from a disease/inflammatory backdrop as discussed in the DIRECT program, (M = 1.65, SD = 0.689, t(25) = -9.955, p = .000, one-tailed). The data also revealed that the NPs believed that adding inflammatory testing to their clinical work-up would play a key role in their ability to properly assess for CV risk and treatment effectiveness, (M = -1.81, SD = 0.849, t(25) = -7.157, p = .000, one-tailed). Additionally, it was found that the NPs believed the information learned in DIRECT would enhance their practice, (M = 1.62, SD = 0.69, t(25) = -10.126, p = .000, onetailed). NPs believed that the DIRECT program fits well into a family practice environment, (M = 1.44, SD = 0.621, t(24) = -11.988, p = .000, one-tailed). Participants also were asked if they believed that NPs were uniquely positioned and qualified to deliver an effective CV prevention program in primary care, and the results revealed that they did (M = 1.19, SD = 0.402, t(25) = 22.934, p = .000 (one-tailed)). A summary of the findings is provided in Table 1.
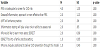
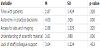
6. Barriers to Implementation
To determine barriers to implementation of the DIRECT program, the participants were asked to answer a Likert scale 1-5 with 1 = poses a great barrier to practice application and 5 = not a challenge to application to practice. Time with patients for education as a great barrier to application of the DIRECT program was found not to be significant (M = 2.87, SD = 1.424, t(22) = -439, p = .328) while Autonomy was found to pose a challenge to practice application, as the results were found to be significant, (M = 4.00, SD = .926, t(21) = 5.066, p = .000, one-tailed). “Access to labs and imaging” was not identified as a barrier to practice; however, the results were found not to be significant, (M = 2.88, SD = 1.329, t(23) = -.461, p = .325). However, the data indicated that the understanding of scientific material does not pose a barrier to practice application (M = 3.61, SD = .988, t(22) = 2.954, p = .0004). Lastly, the participating NPs believed that “the lack of staff/colleague support” was not a barrier to practice application; however, the results were not significant, (M = 3.04, SD = 1.244, t(22) = .170, p = .433). Table 2 summarizes the findings.
To explore the differences in the NPs’ ability to apply DIRECT Program to practice based on socio-demographic characteristics, several two-sample t-tests were performed. Findings indicated that the mean for NPs having more than 15 years of experience (M = 3.50, SD = 1.406) was different from NPs with fewer than 15 years of experience (M = 3.14, SD = 1.406); however, the difference (d = .357) was not statistically significant t(22) =.638; p = .530, two –tailed).
Testing whether there was a significant difference in the NPs’ belief that they are uniquely positioned and qualified to deliver an effective CV prevention program in primary care was not found to be based on the number of years practiced as RNs. The results revealed that the mean for the category of NPs having fewer than 15 years was higher (M =1.27, SD = .458) than that of the category of NPs having more than 15 years; furthermore, the difference (d = .267) was significant t(23) = 1.829, p = .040, one-tailed).
To determine whether the NP’s believed that cardiovascular prevention through a disease/inflammatory lens fits well into the backdrop of family practice care differed based on the number of years they have been in practice as an ARNP. Using a t-test with a median split; two categories were formed: up to 9 years in practice and more than 9 years in practice. The results found that the mean for the category of ARNPs having fewer than 9 years was lower (M = 1.18, SD = .603) than that of the category of ARNPs having more than 9 years (M = 1.64, SD = .633); the difference (d = -.461) was significant, t(23) = -1.845; p = .039, one-tailed.
Time with patients also was determined to be significant when determining if NPs had a desire to learn more about the information learned in the DIRECT program. The difference was determined based on how much time the NPs were able to spend with each patient; using a median split, two categories were established: fewer than 15 minutes and more than 15 minutes. The results indicated that the mean for the category of fewer than 15 minutes was higher (M = 2.00, SD = .816) than that of the category of more than 15 minutes (M = 1.47, SD = .516); moreover, the difference (d = .533) was significant, t(23) = 2.008, p = .0285, one-tailed. Time with patients was also found to be significant on whether the subjects believed NPs were uniquely positioned and qualified to deliver an effective CV prevention program in primary care (M = 1.40, SD = .516) than that of the category of more than 15 minutes (M = 1.07, SD = .258); additionally, the difference (d = .333) was significant, t(23), p = .0215, one-tailed.
Lastly, a regression model was used to test the impact of age on the NPs’ belief that cardiovascular prevention through a disease/ inflammatory lens fits well into the backdrop of family practice care. The regression model was found to be marginally significant, F(1, 23) = 4.285, p = .050. Additionally, as age increases, mean increases as well (b =.021, t(23) = 2.070, p = .050). Lastly, Adjusted R2 was 0.12; hence, 12% of the variation in the dependent variable was explained by age.
7. Discussion and Limitations
The DIRECT program has the potential for practice impact by showing statistical significance with nurse practitioners desire to apply the recommendations discussed in the DIRECT program. These include the belief that risk factor screening guidelines are inadequate to assess for CV risk. They also include the belief that a disease/inflammatory approach to CVD is more effective than the standard of care and also the NPs believe that adding CIMT screening will enhance the ability to identify patients at risk for heart attack and ischemic stroke. Equally impactful is the fact that the subjects agreed that adding inflammatory testing to clinical work-up plays a key role in the ability to assess for CVD risk. Another indication that the DIRECT program has significant impact is that the NPs strongly agreed that they wanted to learn more about this program suggesting that it will enhance their practice and it fits into the backdrop of family practice. Another key element is that the subjects almost unanimously strongly agreed that NPs are uniquely positioned and qualified to deliver an effective CV prevention program in primary care.
The DIRECT program challenges NPs to think outside of the standard risk based paradigm and embrace a new, evidence-based approach to care with the goal of preventing heart attacks and ischemic strokes in primary care practice. Ultimately, the NPs reported that the information learned in the DIRECT program will enhance their practice and they wished to learn more. With this knowledge, this pilot program can be replicated to a larger audience, potentially to all primary care providers.
There is an anticipated shortage of family practice providers in the United States and nurse practitioners have an important role in filling this need (Cassidy, 2012). Primary care providers, such as NPs, care for patients through prevention services and screening, evaluation of new symptoms and ongoing care of chronic disease.
The most significant limitation to this study was the small sample size (N=26), creating an environment of a strong pilot study. To be able to perform certain tests, it was necessary to use median split in a few cases, such as age and the years of practice. Recognizing these limitations and embracing the small sample size as a pilot study opportunity, the positive impact of the DIRECT program creates an opportunity to bring this CV disease/inflammatory risk assessment program to larger audiences. Ultimately, the DIRECT program, created from the Bale/Doneen Method, demonstrates that nurse practitioners believe they are prepared, willing and poised to deliver CVD prevention through the lens of a disease/inflammatory paradigm.
Acknowledgments
No funding sources were utilized for this study. I would like to thank the Nurse Practitioner Group of Spokane for their participation and interest in this research. I would also like to thank Dr. Mirjeta Beqiri for her statistical support and wisdom. Also, Drs. Neva Crogan sand Alice Dupler for their valued insight and expertise in research. Lastly, Dr. Bradley Bale for his contribution as a content expert and mentor.
Competing Interests
The authors declare that they have no competing interests.