



1. Introduction
Within specialized rehabilitation facilities, patients are in need of complex rehabilitation following spinal cord injury, brain injury, stroke, multiple trauma, burns or other neurological diseases. Impaired balance control, increased risk of falling and further disability due to this, are common challenges for a large part of the patients. Therefore, prevention of falls is a priority, both in clinic and research. To improve balance control through a variety of rehabilitation actions, are important objectives and it is essential to use reliable, valid, clinically feasible and applicable assessment methods. The Mini-BESTest is a relatively new instrument for assessing dynamic balance.
Balance control is the foundation of our ability to move and function independently [1] and may be reduced due to loss of motor, sensory and cognitive function. In older adults, the psychological impact of a fall may be considerable, leading to fear of falling, imposing constraints on functioning and activity, and increasing dependence on assistance and aids, thus limiting independence [2]. This is a concern also in rehabilitation, thus, fall prevention, assessment and training of balance control is therefore important during rehabilitation. The objective of clinical testing of balance control is to assess the risk of falling, assess changes over time and to identify disorders in the different subsystems involved in balance control.
The Mini-BESTest is a short version of the Balance Evaluation System Test (BESTest) [1], a theory based comprehensive clinical balance test, developed to identify the postural control systems causing balance impairments. The BESTest assesses six subsystems of balance control: biomechanical constraints, stability limits, anticipatory balance reactions, reactive balance reactions, sensory orientation and stability in gait. In order to identify the items included in the Mini-BESTest, a factor analysis and Rasch analysis of the BESTest were performed, and redundant and insensitive items were eliminated. The total number of items was reduced from 36 to 14, items was scored from 0–2, with a maximum score of 28 points [3,4].
The Mini-BESTest takes 15-20 minutes to complete, compared to 45-60 minutes for the full BESTest, and has gained in popularity both as a clinical tool and as a research outcome measure [4]. It has been translated into Swedish, Danish [5,6], Spanish, Japanese, Portuguese (Brazil), Portuguese (European), Greek and French [7]. A Norwegian translation is in progress (Master's thesis, University of Oslo, 2015). The Mini-BESTest has been found to have good concurrent validity for patients with neurological disorders such as stroke and Parkinson's disease (PD) [5,8,9], and has satisfactory predictive validity in identifying future recurrent fallers in patients with PD, especially during the first 6 months following assessment [10].
In order to determine whether the Mini-BESTest could be used in a rehabilitation facility on a regular basis, the validity and the feasibility of the test had to be determined. The aim of the present study was therefore: a) to study the difference in dynamic balance between fallers and non-fallers, between patients afraid of falling and not afraid of falling, between patients with high and low fall concerns, between patients with good versus bad ambulatory ability and between different diagnostic groups, b) to study the relationship between dynamic balance and fall concerns and, c) to study the feasibility and usefulness of the Mini-BESTest as a clinical tool in a rehabilitation facility.
To our knowledge, this is the first study using the Mini-BESTest within a specialized rehabilitation facility in Norway.
2. Methods
2.1 Design and approach
A cross sectional study was conducted. Data was collected as part of the regular assessment of dynamic balance in patients hospitalized at Sunnaas Rehabilitation Hospital, Norway during the period May 2011 to March 2012.
2.2 Data collection
Twenty-nine physiotherapists with 1 to 25 years of clinical experience (median 10 years) assessed 1-5 patients each (median 2 patients), in total 59 patients. Prior to the study the PTs had been trained in using the Mini-BESTest. In 37 of 59 (63%) of the cases the assessment was conducted by two cooperating physiotherapists.
2.3 Participants
Patients aged ≥ 18 years hospitalised at Sunnaas Rehabilitation Hospital during the study period, with impaired balance control as regarded clinically by their physiotherapist (PT), fulfilling the inclusion criteria and willing to participate in the study, were included. Patients were recruited by their regular PT. The inclusion of patients was pragmatic and based on the comprehensive assessment by the PT, regarding the suitability of using the Mini-BESTest as a measure of dynamic balance for the individual patient. Patients who used a neck brace or a 3-point corset, or who had weight bearing or mobility constraints of the lower limbs were excluded. A total of 59 patients were included, 38 men and 21 women, median age 52 (range 20-76) years (Table 1).
2.4 Ethics
All participants gave their informed consent prior to participation in the study. The study was approved by the Norwegian Data Protection Officer for Research at the Oslo University Hospital. The study was regarded as a quality control study at the hospital, thus no formal ethical application was necessary.
2.5 Measurement instruments/variables
Demographic and other relevant background information were obtained from the patient's electronic records. The patients' history of falls the past year and fear of falling were reported in a structured interview.
2.6 Dynamic balance
Dynamic balance was assessed with the Mini-BESTest [3,7]. Anticipatory balance reactions were tested in 3 test items (sit to stand, rise to toes, stand on one leg), reactive postural control were tested in 3 items (compensatory stepping correction – forward, backward and laterally), sensory orientation were tested in 3 items (stance on firm surface, foam surface or incline, with eyes open/closed) and dynamic gait was tested in 5 test items (change in gait speed, walk with head turns, walk with pivot turn, step over obstacle and Timed up & go with cognitive task). The 14 items are scored on a 3-level scale, 0= 'severe impaired balance', 1 = 'moderate impaired balance' and 2 = 'normal balance’, giving a total score from 0-28 points, higher scores meaning better dynamic balance. In lack of a formal Norwegian translation of the Mini-BESTest, a working translation into Norwegian was conducted by the research group based on the English, Danish and Swedish translations and was used in the present study.
Ambulatory ability was assessed using the Functional Ambulation Categories (FAC) [11], which classifies walking ability in six categories (0-5). Categories 0-3 indicate dependent walking and 4-5 independent walking.
Fear of falling was assessed asking the patients the single-item question: In general, are you afraid of falling? [12] Answering alternatives were ‘not at all’, ‘a little’, ‘quite a bit’ and ‘very much’. The responses were dichotomized, and patients answering ‘not at all’ were categorized into the ‘not afraid of falling’ group.
Fall concerns was assessed using the Falls Efficacy Scale - International (FES-I) [13,14]. FES-I refers to the patients concern about falling while performing specific daily activities [13].The patients were asked to assess concern about falling during 16 standing and walking activities, scored from 1 to 4 where 1 = 'not concerned and 4 = 'very concerned'. Items were summed into a total score of 16- 64 points, higher scores indicating stronger concerns about falling, i.e. low falls- efficacy. According to Delbaere et al. [15], the cut off point for low fear-related self-efficacy is ≥23 points.
The number of falls during the last year (after injury/disease onset) was reported by the patients. Patients with one or more falls were classified as ‘fallers’. After the completion of each Mini-BESTest, the physiotherapists scored the feasibility and the usefulness of the Mini- BESTest on a structured questionnaire developed for the study (Table 2). The questionnaire contained 12 statements scored on a 0-6 points Likert scale, 0='Agree completely' and 6 = 'Disagree completely'. A score of 3 was interpreted as neither agreement nor disagreement (indifference).
The data were analysed with the statistics program SPSS, version 19.0 (IBM SPSS Inc., Chicago, IL, USA). Non-parametric statistics, and median and range were used to display central tendency. The Mann-Whitney U test was used to compare two independent variables, and the Kruskal-Wallis test or One-way ANOVA for more than two variables. The level of significance was chosen to be 5% for all analyses (p < 0.05). Pearson's correlation coefficient (Pearson's r) was used to determine the correlation between the total score for the Mini-BESTest and the total score for the FES-I, and was interpreted in accordance with Domholdt [16]: 0 to 0.25 = little, if any correlation, 0.26 to 0.49 = low correlation, 0.50 to 0.69 = moderate correlation, 0.70 to 0.89 = high correlation and 0.90 to 1.00 = very high correlation. The determination coefficient (r2) was used to show the amount of variation in one variable that can be explained by the other variable.
3. Results
3.1 Patients
One third of the patients had a spinal cord injury (34%) and 29% had a traumatic brain injury. The distribution between diagnostic groups can be seen in Table 1. Walking aids were used by 17 of 51 (33%) patients, the number increased with decreasing ambulatory mobility; 8 of 42 (19%) in FAC 5, 7 of 10 (70%) in FAC 4 and 3 of 3 (100%) in FAC 0-3. A total of 21/51(41%) had been falling at least once the past year (Table 1).
3.2 MiniBEST-test
The median score in the Mini-BESTest for the whole patient group was 22 (1-28) points (Table 1). The distribution of scores on the Mini- BESTest is presented in Figure 1. There was no significant difference in MiniBESTest score between fallers and non-fallers (p=0.49), between patients afraid of falling and those not afraid of falling (p=0.43), or between diagnostic groups (p = 0.67). A significant difference (p=<0.001) in dynamic balance was found between patients with different degrees of ambulatory ability (FAC 0-4 versus FAC 5).

3.3 Fall-related concerns
Fear of falling was reported by 23/52 patients (44%) and the median FES-I score was 22 (range 16-45) points (n=52) (Table 1). There was no significant difference in FES-I score between fallers and non-fallers, between patients afraid of falling and those not afraid of falling, between patients with different degrees of ambulatory ability, nor between the diagnostic groups (p = 0.45). Twenty-three patients (44%) had strong fall concerns (FES-I ≥ 23 points). There was no difference in Mini-BESTest score between those with high versus low fall concerns. The largest proportion of patients with low fall concerns was among patients with spinal cord injury (11 of 18) and lowest proportion was found in patients with traumatic brain injury (4 of 15).

3.4 Falls
The median number of falls among those who had fallen in the last year was 3 (range 0-300) falls. Eight of the 21 fallers (38%) had low fall concerns (Table 1). There was no significant difference in age (p = 0.70), ambulatory ability, dynamic balance (p = 0.49) or falls-efficacy (p = 0.81) between fallers and non-fallers. There were 48% women in the group of fallers, and 7% women in the group of non-fallers. There was a low and negative correlation between the total Mini-BESTest score and the total FES-I score (r = - 0.394, p = 0.004, r2 = 0.16) for the group as a whole (n = 52) (Figure 2).
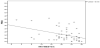
Trendline for the correlation superimposed (n = 52).
3.5 Feasibility
In 94% of the cases the PT’s agreed that the test facilities and equipment satisfied their expectations, and that the test was easy to learn (Table 2). The lowest agreement were found on statements concerning whether the test could be conducted by only one PT, and PTs assessing patients with traumatic brain injury in particular responded negatively to this statement.

3.6 Usefulness
In 83-89% of the cases, the PTs agreed that the test was relevant, provided valuable information, and was consistent with the patient's functional level (Table 2). Lowest agreement was found on the statement that the test information alone could be used to customise a treatment programme for the patient. In 75% of the cases the PTs agreed with the statement ´Overall, I think the Mini-BESTest can be used in the clinical rehabilitation setting'.
4. Discussion
4.1 Summary of results
A total of 21 out of 51(41%) patients had fallen during the last year, and 23 out of 52 (44%) had a strong concern about falling. Generally, the patients had moderate to light reductions in dynamic balance, median Mini-BESTest score of 22 (range 1-28) points. There was no significant difference in dynamic balance between fallers and nonfallers, between those afraid of falling and not afraid, between those with high and low fall concerns or between the diagnostic groups. There was a significant difference in dynamic balance between groups with different degrees of ambulatory ability. The PTs found the Mini-BESTest feasible and useful as a clinical tool for assessing dynamic balance in a specialized rehabilitation facility, with some precautions. Two testers should be present when assessing patients with severe physical and /or cognitive impairments. Also, the results from the Mini-BESTest should be supplemented with the patient's history of falls, fall-related concerns, diagnostic specific data on movement function, activity limitations and participation restrictions within a therapy programme for improved balance control.
4.2 Dynamic balance
The patients in the present study showed a somewhat better dynamic balance than the patients with PD reported by Bergström et al. [5] and Duncan et al. [17], who found 23 and 22 out of 32 points, respectively. Bergström et al. [5] and Tsang et al. [18] studied patients with stroke, and reported 14 out of 32, and 19 out of 28 points, respectively. The somewhat better balance control found in the present study may be explained by the diverse group of patients with a lower median age (52 years versus 60 and 78 years, respectively). Also, the higher level of dynamic balance in the present study may be caused by the selection done by the PTs who for each patient considered whether conducting the balance assessment would be correct from a clinical and feasible/ workable perspective. Thus, primarily patients with moderate to minor balance deficiencies were included.
Contrary to what we had expected, we found no difference in dynamic balance between fallers and non-fallers (known-groups validity), between those afraid of falling and not, between those with high and low fall concerns, or between the diagnostic groups. This may both be due to the lack of spreading on the Mini-BESTest scale, as well as relatively small patient groups. It may be that with a different cut-off point, for instance between frequent fallers (≥ 3 falls) and less frequent fallers (0-2 falls), would have made a different result. However, based on these findings, we could not confirm the construct validity based on the known group validity method of fallers versus non-fallers or persons afraid of falling versus persons not afraid of falling.
4.3 Fall-related concerns
The patients reported a moderate degree of fall concerns, and there was a low correlation between the Mini-BESTest and the FES-I, where only 15% of the variation in the Mini-BESTest could be explained by the variation in FES-I. This is consistent with Bergström et al. [5], who found a low correlation between the Mini-BESTest and the FES-I in patients with a mild to moderate PD, indicating that factors other than dynamic balance influence the patients’ concern about falling while performing specific daily activities.
A larger proportion of patients with spinal cord injuries reported strong fall concerns than patients with traumatic brain injury, also when controlling for Mini-BESTest score. There may be both motor control, perceptual, cognitive and/or other differences between the groups that may account for this, and needed to be further investigated.
4.4 Dynamic balance and falls
In the present study, dynamic balance was not related to previous falls. This finding was in contrast to studies of patients with stroke [18] and patients with PD [9,19], who found lower scores of dynamic balance in fallers than in non-fallers. The discrepancy between these studies may be because the patients in the present study often had minor balance deficiencies, and was a diverse group of patients with several different diagnoses. Falls may also be affected by other factors such as cognition and attentiveness, in addition to neuromuscular and sensory function.
4.5 Feasibility
Overall, the PTs felt comfortable with the test situation, and found the Mini-BESTest easy to learn. The PTs who took part in the study had clinical experience of balance assessments, and were familiar with the test items in the Mini-BESTest. It can therefore be assumed that the test will be relatively simple to implement in the clinic. However, only 1/3 of the tests were conducted by only one tester, showing that this test might substantial human resources. The need for two persons present during assessments applies in particular to testing of patients with severe physical and/or cognitive impairments. Thus, lack of resources and the availability of an assistant can make the PT choose other clinical assessments than the Mini-BESTest.
4.6 Usefulness
The physiotherapists found that the Mini-BESTest provided relevant and valuable information, and was consistent with the functional level of the patient. Thus, it may be argued that the Mini-BESTest is better suited for persons with a higher functional level, for example compared to Bergs balance scale [20], which to a greater extent assesses static balance. This view was supported by King et al. [8]. who found that the Mini-BESTest was more suited for distinguishing between high and low functioning patients. One observation from the present study period was that the PTs seldom included patients with major balance deficits. They found it not appropriate to use the Mini- BESTest as the patient would achieve a very low total score, and/or that the patient would not benefit from the assessment.
Most of the PTs took an indifferent or negative stance on whether the results of the Mini-BESTest alone could be used to customise treatment programme for a patient with impaired balance control. This was in accordance with both King et al. [8] and Duncan et al. [17] who highlight the importance of including supplementary tests of muscular strength, sensory function and cognition, together with the patient’s history of falls and concern of falling, to strengthen the assessment of the patient's dynamic balance [17].
The results of the present study indicate that the Mini-BESTest may be appropriate for use in a rehabilitation facility. The Mini-BESTest may enable PTs to acquire useful information about the patient's dynamic balance that, together with supplementary information, can be used to build targeted treatment programmes.
4.7 Method discussion
The present study has several limitations. The inclusion of patients were based on the PTs own judgement of suitability for balance assessment. This led to a selection bias in favour of patients with minor to moderate balance deficiencies which are limiting this study's validity for use of the test for patients with severe balance impairments. Experience indicates that these patients will require two testers present, and that results must be supplemented with additional information to form the basis for interventions. Also, patients who uses walking aid such as a stick or lower limbs orthotics will be given one score lower, implicating that these patients very often would be given the score zero, thus these patients would score very low on the mini-BESTest.
It is a limitation to the reliability of the study that there were 29 PTs, i.e. data collectors. A formal inter- or intra-rater reliability study has not been conducted in the present group, thus we do not know how different these results would have been with another group of PTs.
Furthermore, retrospective reporting of falls, as in this study, may have led to under- or over-reporting of falls, which, together with missing data regarding falls and fear of falling, adds uncertainty to the interpretation of the results.
One strength of the present study was that the data was collected in a real-world clinical setting and all PTs underwent training on the Mini-BESTest prior to patient inclusion in order to ensure a common understanding. Also, often there were two therapists present during assessments, and this may have increased the reliability of the testing.
The Mini-BESTest was considered as a feasible and useful clinical tool for assessing dynamic balance in the specialized rehabilitation facility, when including two precautions. Two testers should be present when conducting the assessment in patients with severe physical and/or cognitive impairments, and the results of the Mini- BESTest should be supplemented with the patient's history of falls, fear of falling, diagnosis-specific data, activity limitations and participation restrictions when used to build therapy programmes. The results from the present study may only be generalised to patients with a moderate to minor degree of impaired dynamic balance, and with the same diagnoses as in this study. There is a need for further research to establish psychometric properties for the Mini-BESTest in rehabilitation, for instance the responsiveness to change.
5. Conclusion
The Mini-BESTest was found to be a feasible clinical tool for assessing dynamic balance in a facility for specialized neurological rehabilitation. Two testers should be present when conducting the test in patients with severe physical and /or cognitive impairment. The mini-BESTest should be supplemented with the history of falls, fall-related concerns, diagnosis-specific data and data on activity and participation.
Competing Interests
The Authors declares that there is no conflict of interest.
Author Contributions
Kirsti Skavberg Roaldsen: idea, conceptualization, study design, data
analysis, interpretation, drafting, final approval.
Ellen Wakefield: study design, data collection, data analysis,
interpretation.
Arve Opheim: conceptualization, study design, data analysis,
interpretation, drafting and critical review.
Acknowledgments
The authors would like to thank all the 29 PTs that contributed with the data collection. We also want to thank the expert PTs participating in the project group contributing to conceptualization of the study, study design, administration, data collection, constructive discussions and interpretation of the data; Vivien Jørgensen, Jill Underland O’Farrell, Grete Anmarkrud, Vedrana Bebanic, Marit Nygaard Olsson and Ingeborg Prestholt. A special thanks to Britt Elfving at Karolinska Institutet, Stockholm, for critical review of the manuscript and for guidance in interpretations.