


1. Introduction
Ultrasound guided regional anesthesia (UGRA) was first described by La Grange et al. in 1978. In recent years UGRA has been gaining popularity. There is increasing focus on UGRA in educational programs, increased use in the clinical setting and a continuously growing volume of literature on the topic [1].
Regional anesthesia is a well-accepted modality of treatment in the perioperative setting. Ultrasound guidance allows us the visualization of anatomic structures (nerve roots, vasculature, etc.). The peripheral nerve stimulator method of regional anesthesia does not allow for the direct visualization of anatomy and instead relies on physical signs to determine correct needle placement. One of the disadvantages of performing regional anesthesia without the use of ultrasound is a higher rate of nerve block failure as compared to general anesthesia. Higher rates of failure could possibly be attributed to a lack of appropriate equipment such as ultrasound machines, supplies for the ultrasound machine, a dedicated area to perform blocks, and more so the lack of proper training. The use of the modern ultrasound has alleviated some of these problems. The use of ultrasound, however, requires some basic understanding of the ultrasound technology along with knowledge such as the ability to properly identify various anatomic structures and vessels using the ultrasound machine [2].
Though UGRA has been gaining popularity, information regarding the learning process, development of skills, training programs and standards of practice are scarce. There currently is no gold standard for UGRA education [3]. The UGRA process requires a new set of skills in relation to understanding and operating the ultrasound machine, comprehension of cross-sectional human anatomy and knowledge of appropriate terminology. Current methodologies used to learn UGRA by nurse anesthetist graduate students are lacking in areas of simulation learning and it’s efficacy. There is also a lack of standardization in the teaching process both in the clinical setting as well as in terms of standards of practice [1].
Literature on the number of UGRA iterations to achieve a level of proficiency in the nurse anesthetist graduate student population is scarce. In general, research suggests that a combination of simulation training along with education does improve the quality of UGRA from a baseline accuracy rate of 57% to 79% and 52.5 to 79.2% respectively at the 12-month period [4]. Simulation training has been shown to be effective in improving UGRA skill in anesthesia residents [5]. The use of simulation as an educational tool has been widely accepted as a means where students can practice and hone their skills to help prepare for clinical [6].
Ultrasound guided regional anesthesia is beneficial from an economic standpoint as it helps reduce costs in comparison to the nerve stimulator approach. A cost reduction of $13.90 occurred per nerve block when placing infraclavicular catheters[2]. Sites et al., [1] suggests that future research be geared towards developing teaching interventions to educate clinicians on UGRA. There is also no research on the number of iterations required to achieve a level of proficiency to perform UGRA of the interscalene brachial plexus nerve block among neophytes.
Ultrasound guided regional anesthesia requires the acquisition of additional skill sets as compared to the peripheral nerve stimulator approach. Furthermore, clinical care has increasingly been driven by efficiency and time management. UGRA training requires increased coordination of staff and resources. A factor that plays a key role in the time management and cost is how quickly and proficiently a clinician can identify the interscalene brachial plexus nerve bundle. The overall aim of this project was to evaluate the efficacy of simulation education on learning UGRA. This project specifically aimed to quantify the number of iterations and the amount of time required to reach a level of proficiency to identify the interscalene brachial plexus nerve bundle accurately. Currently there are no studies that evaluates the efficacy of simulation education of UGRA of the interscalene brachial plexus nerve bundle among the nurse anesthetist graduate student population. The results from this pilot study will provide the Nurse Anesthetist Program at the School of Nursing, University at Buffalo (UB) with evidence-based information, which might assist in UGRA training activities. This intervention is important to all graduate student nurse anesthetists, as regional anesthesia is a part of our anesthetic practice. Graduate student nurse anesthetists would be required to have some understanding of UGRA in the clinical setting as well as in their professional career as clinicians. Knowledge of UGRA is also critical to clinicians in their practice as healthcare organizations aim towards providing quality and cost effective care that improves patient satisfaction.
The project aims to investigate
- Quantify the number of iterations required by graduate student nurse anesthetists to accurately identify the interscalene brachial plexus nerve bundle;
- Assess the efficacy of the UGRA program by calculating time differences over iterations required to note a statistically significant decrease in time taken to locate the interscalene brachial plexus nerve bundle;
- Assess student perception of this UGRA program as noted by improved confidence levels, comfort and knowledge related to the use of the ultrasound & identification of interscalene brachial plexus nerve bundle.
2. Literature Review
Orebaugh, Williams, & Kentor [7], conducted a study to assess the impact of ultrasound guidance on anesthesia resident performace. They concluded that UGRA of the interscalene, axillary, popliteal, and femoral nerve blocks required less time as compared to the peripheral nerve stimulator method [peripheral nerve stimulator method lacks the visualization of the never bundle and relies on physical signs to determine correct needle placement] (median = 1.8 mins vs 6.5 mins respectively; p< .001). UGRA required fewer needle insertions than the peripheral nerve stimulator approach (median = 2 and 6 respectively; p<.001). There were fewer blood vessel punctures with ultraound as compared to the peripheral nerve stimulator method (p=.03). This study illustrated the benefits of UGRA vs. the nerve stimulator method.
Niazi, Haldipur, Prasad, & Chan [5]conducted a study to evaluate whether simulator training assists novice anesthesia residents in attaining proficency in UGRA. The reseachers used a randomized convenience sample of third year anesthesia residents: ten in the simulation group and ten in the conventional group. Both groups received conventional training of 4 didactic lectures on peripheral nerve blocks and ultrasound guidance. Additionally, the simulation group received an hour long low fidelity training session on needling and proper hand-eye coordination. Residents recorded the number of successful and failed UGRA blocks performed over a three week period during their block rotation (period of time dedicated to solely doing regional anesthesia). The convetional training group of ten residents had 98 successful blocks and the simulating group of ten residents had 144 successful blocks (51.3% vs 64%; P =0.016). Proficiency was reached by 4 of 10 residents in the conventional group and 8 of 10 residents in the simulation group (40% vs 80%; P=0.0849). This study illustrates the effectiveness of simulation as a tool in learning UGRA.
Sites, Gallagher, Cravero & Johan [8],evaluated the learning curve of performing an ultrasound guided interventional procedure among experienced anesthesia residents. The reserchers enrolled ten subjects. The subjects were given an introduction to the ultrasound system and were asked to perform 6 sequential trials of simulated breast cyst aspirations in two sets of 3 trials. After completion, the researchers noted that the performace times of the task was reduced by 38% and 48% respectively. Composite accurary scores improved 36% and 59% respectively. This study showed that anesthesia residents can drastically improve their performace speed and accuracy in performing a simulated task repetitively.
Simulation training also leads to performance improvements. Two groups of anesthesia trainess were selected for a simulation exercise. One group underwent training for management of malignant hyperthermia and the other group underwent training for anaphylactic shock. Both trainee groups were then asked to participate in a test scenario related to the management of malingnant hypertheremia. Participants who were trained in the malingnant hyperthermia group responded more quickly, managed the simulation better, and deviated less from the accepted procedure compared to those trained in the anaphylactic shock group. The group that underwent simulation training for malignant hyperthermia had significantly overall better performance than the anaphylactic shock group. This study also concluded that anesthesia simulation training improves performance [9].
Repetition and learning are memory dependent phenomena where in performace of a repeated task is improved as a function of repeated expereinces. Research by Hauptmann & Karni [10] suggests that performance learning of a simple and memorization test improves dramatically from the first to the sixth repetition. After the sixth repetition, improvements in the learning curve plateaus up to the tenth iteration.
The articles above can be generalized and applied to this project. The literative review informs us that UGRA is more efficient as compared to the nerve stimulator method of regional anesthesia. It also illustrates that simulation education is a good method of learning UGRA and suggests that repetition of a simulated activity can improve task performace.
3. Theoritical Basis
Malcom Knowles’ Adult Learning Theory (ALT) has been identified as the theoritical basis for this capstone project. The ALT was built on the principles of generalization, reinforcement, and transference of knowledge. A presumed expectation for ALT is that the students would have set self-directed learning goals for themselves [11]. According to Knowles [12], the readiness to learn states that “people become ready to learn something when they experience a need in order to cope more satisfyingly with real life tasks or problems. The educator has a responsibility to create conditions and provide tools and procedures for helping learners discover their ‘needs to know’ ” (p. 44). This assumption could be made for the graduate student nurse anesthetist population, as regional anesthesia is part of the educational curriculum in the SUNY UB nurse anesthetist program. Students are expected to be relatively proficient at UGRA by the end of the educational program through in class learning as well as practice in the clinical setting. There are several ATL principles that support the idea of simulation such as: (a) learning occurs when a learning deficit is identified, (b) the learner wants to be an active participant in the learning process, (c) the instructor aims to facilitate learning, (d) learning is centered around the problem and the learner, and (e) timely feedback reinforces what is learned [13]. Limitations of the ALT in this setting could be that it is based on observations and that the adult learning experiences could vary among individuals.
This project involved educating the second year nurse anesthetist graduate students who volunteered to be a part of the UGRA program. Participants were educated about UGRA and provided a demonstration on how to locate the interscalene brachial plexus nerve bundle under ultrasound guidance. Students repeated the hands on learning experience six times in total. Through each progressing repetition, the students identified limitations in the learning and hopefully worked on these limitations through repetitive action. Feedback was provided at the end of the simulation sessions. These steps fulfill the basic principles of the ALT.
4. Ethical Issues
The Institutional Review Board (IRB) at the University at Buffalo has approved this project. All participants were volunteers and there was no monetary compensation of any sort. Participants did have the option to remain anonymous during the study. Anonymous recordings on ultrasound nerve blocks have been securely stored on the UB server.
5. Design
This is a pilot study. Following IRB approval, an in person announcement was made at UB targeting second year nurse anesthetist graduate students. Students who committed to the time requirements of this project were selected. This capstone project used a repeated measures design (RMD) with a pretest – posttest method on a convenience sample of second year nurse anesthetist graduate students. The second year graduate student nurse anesthetists were in their fifth semester of a nine-semester program at the time of the project. The participants were asked to use the ultrasound machine and identify the interscalene brachial plexus nerve bundle. This sequence was timed. Performance of the ultrasound-guided procedure was recorded on the ultrasound machine and analyzed by an expert in the field of anesthesia for accuracy.
Overall percentages of successful identifications among students for each iteration were plotted on an X-Y graph. Participants were also provided with a one-page survey at the end of the program to assess their perceptions of the UGRA program. The RMD involved collection of data at multiple points in time and the data were used to track changes noted in the study[14]. The main advantage of the RMD is subject heterogeneity. The level of error is reduced since there is only one group of participants in all level of the independent variable. Another advantage to the RMD is that fewer subjects are required as each subject serves as its own control [14].
6. Methods & Analysis
Data collection occurred via observation by the researcher along with electronic data. Electronic data was recorded and included video recordings of the ultrasound identification of the interscalene brachial plexus. The video recordings were used to analyze accuracy of the interscalene brachial plexus nerve bundle located by the participants. The pretest was conducted in a simulation laboratory of the School of Nursing, University at Buffalo two weeks prior to the education session and five post-test iterations. An enclosed and private space was made available for the study. A volunteer model was relied upon for the identification of the interscalene brachial plexus nerve bundle. The same volunteer model was also used for the educational session. Each participant was assigned a unique non-identifiable participant number to keep track of each participant’s progress through the project. A Sonosite ultrasound machine was used for the project. The image depth for the ultrasound machine was set at a constant 2.7 centimeters for all image identifications. The cursor function was selected on the Sonosite ultrasound machine. This function activates a cursor on the screen. The start time for the interscalene brachial plexus nerve bundle identification began once the ultrasound probe was placed on the skin. Once the participant felt they had accurately identified the interscalene brachial plexus nerve bundle they were asked to move to cursor and place it over the nerve bundle and the timer was stopped. No feedback was provided to participants after the pretest iteration.
The education session and five posttest iterations was also conducted two weeks after the pretest iteration in the simulation laboratory of the School of Nursing, University at Buffalo. This educational session covered the basics of the ultrasound machine and the anatomy related to the interscalene brachial plexus nerve bundle. Videos and hands on demonstration were used to educate the participants on how to appropriately identify the interscalene brachial plexus nerve bundle under ultrasound.
Participants served as models for each other. Participants and models were randomly assigned in a manner that no participant had the same model twice. Watching other participants perform the simulated task while being a model could affect performance and learning. Therefore, all participants were instructed to turn their head away from the screen of the ultrasound machine when they were acting as models for other students. The participants performed five iterations of the interscalene brachial plexus nerve bundle using the ultrasound and these iterations were timed and the ultrasound images were recorded. An expert in the field of anesthesia evaluated data recorded on the ultrasound to assess whether participants correctly identified the interscalene brachial plexus nerve bundle. Results are plotted on an X-Y graph. The graphs illustrate the relationships between time taken to identify the interscalene brachial plexus nerve bundle and the number of iterations required for successful identification. Results of accuracy of identification of the interscalene brachial plexus nerve bundle for each iteration is plotted on an X-Y graph. Results are also summarized using descriptive statistics.
Participants filled out an evaluation survey (Participant Survey) to assess the quality of the instruction component of the project. The researcher also collected data (Researcher Data Collection Form) for the capstone project during the simulation exercise. Thomas E. Obst, PhD, CRNA, validated whether participants have accurately identified the interscalene brachial plexus nerve bundle under ultrasound guidance. Dr. Obst assessed validity of the student satisfaction survey and protocol.
7. Protection of human subjects
Maintaining the ethical principles of beneficence, justice, and respect for person as per The Belmont Report would safeguard participants [16]. Participation in this capstone project is voluntary. Informed consent was obtained from participants and participants had the choice to be anonymous if they wanted to. All recorded ultrasound images will be stored on the secure UB server. The survey results will be destroyed once the capstone project data analysis and defense has been completed.
8. Results
Six participants were involved in this study. Each participant performed one pretest ultrasound guided identification of the interscalene brachial plexus nerve bundle. This was followed by and educational session and five-posttest ultrasound iterations. Figure 1.0 illustrates the relationship between iterations and the percentage of correct responses. During the pretest (iteration #1), only oneparticipant (16.67%) was able to accurately identify the interscalene brachial plexus nerve bundle. During posttest iterations #2, #3 and #4, three of the six (50%) participants accurately identified the interscalene brachial plexus nerve bundle. Posttest iteration #5 and #6 had 4 out of 6 (66.67%) and 5 out of 6 (83.33%) participants respectively identify the interscalene brachial plexus nerve bundle. The overall accuracy rate for all participants improved from 16.67% for the first iteration (pretest) to 83.33% during the sixth iteration.

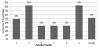
Figure 2 illustrates the time taken to accurately identify the interscalene brachial plexus nerve bundle. Time to accurate identification ranged from 21 seconds (s) in the first iteration to 40s in the sixth iteration. The average time taken to accurately identify the interscalene brachial plexus nerve bundle during the second, third, fourth and fifth iteration was 64s, 97s, 52s and 63s respectively. The average overall time to identification of the interscalene brachial plexus nerve bundle over six iterations was 1minute 19seconds. A point to be noted is that from iteration number 2 (first iteration after education session) to iteration number 6, the time taken to accurately identify the interscalene brachial plexus nerve bundle decreased from 64s to 40s along with an increase in the number of participants who accurately identified the nerve bundle. A clear trend cannot be noted due to the variations in the number of participants who accurately identified the interscalene brachial plexus nerve bundle, however, a downward trend in time can be observed.

Time to correct response (time to first correct identification of the interscalene brachial plexus) for participants to identify the interscalene brachial plexus nerve bundle ranged from 21s to 351s. The average time to correct response was 1 minute 24 seconds. The number of iterations required to accurately identify the interscalene brachial plexus nerve bundle accurately ranged from 1 to 3 iterations with an average of 1.83 iterations required. Figure 3 illustrates the overall rate of accuracy of identification of the interscalene nerve bundle for each participant. The rate of accuracy ranged from 33% to 83% (rounded) with an average accuracy rate of 53% (rounded).
The participant survey distributed out at the end of the simulation program was aimed at assessing participant’s satisfaction with the UGRA simulation program. Figure 4 illustrates that all participants strongly agreed that the UGRA program was beneficial; the information present was pertinent to their program of study, the program provided them with knowledge of the ultrasound anatomy of the interscalene brachial plexus nerve bundle and the objectives of the program were clearly defined. All participants either strongly agreed or agreed (83% and 17% respectively) that they felt confident in their ability to perform the interscalene brachial plexus nerve block after this UGRA program. Eighty three percent of participants (5 participants) agreed that the quality of the audio-visual presentation supported their learning vs. 17% (1 participant) had a neutral view towards to presentation.

9. Discussion
Limitations to this study include a small sample size and short duration of the project. The educational component and 5 post educational iterations were all done on the same day. The results obtained could be skewed due to the short duration of the program. These results may not reflect long-term knowledge. The use of face validity is another limitation to the study as it is subjective and only provides an appearance of a measurement and not a quantification of the validity of the data. The average accuracy rate of identification of the interscalene brachial plexus nerve bundle for each participant is 53% (average of three correct iterations out of six). Only one participant in the pretest was able to identify the interscalene brachial plexus nerve bundle. The increase in rate of accuracy over iterations could be attributed to the education component and repetitive simulation activity. An added limitation to this project includes incomplete data received in the participant survey.
Ideally this study would have been conducted over a period of a couple months to analyze long-term learning and retention of information. Figure 5 illustrates previous ultrasound workshop attendance and previous ultrasound use experience of participants in the study. Four of the six participants in the study had attended ultrasound workshops prior to the study and five participants had previous experience using the ultrasound. Participants who had previous ultrasound experience stated they had used the ultrasound between one to five times. Prior use of the ultrasound and participation in the ultrasound workshop could have also influenced the results of this project. Since participation was anonymous, a correlation could not be made between participants who had prior experience with ultrasound use and/or prior exposure to an ultrasound workshop and test results. For future research, my recommendation would be to replicate this study on a larger scale over a longer period of time to assess long-term learning and efficacy of simulation learning of ultrasound guided regional anesthesia.

The study contributes to the body of knowledge related to the learning of UGRA and the nurse anesthetist graduate student population. Results from the study could be used to help create an educational training program for nurse anesthetist graduate students. This project could also be used as a blueprint to replace other UGRA projects.
Competing Interests
The authors declare that they have no competing interests.