


1. Introduction
Inpatients in adolescent psychiatric wards have often had difficulties in school, at home, or in the community due to self-harm, problematic behaviors such as violence and harm to others, or depression and obsessive-compulsive symptoms [1]. Inpatient psychiatric treatment of adolescents allows children to temporarily leave a difficult situation and live in another environment [2]. In this context, nurses play a central role in inpatient care [3].
In recent years, an increase in the prevalence of autism spectrum disorder (ASD) has been observed in the medical field [4]. Because ASD is atypical development, some individuals may not be able to accept their own characteristics because of the development of metacognition and recognition of the differences between self and others, which makes them perceive themselves as being different and special from typically-developed individuals [5]. Individuals with ASD have poor social skills and are more likely to have difficulty with interpersonal relations. In addition to such difficulty, inpatients with ASD may be under the influence of adverse environments such as a lack of understanding and abuse[1,6], which may result in low self esteem[7,8].
2. Literature Review
ASD, a developmental disorder, is a diagnosis specified in the Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM-5) published by the American Psychiatric Association (APA). The condition is characterized by (1) persistent impairment in interactive social communication and interpersonal interactions and (2) limited and repetitive behaviors, interests, and activities [9].
ASD, a developmental disorder, is a diagnosis specified in the Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM-5) published by the American Psychiatric Association (APA). The condition is characterized by (1) persistent impairment in interactive social communication and interpersonal interactions and (2) limited and repetitive behaviors, interests, and activities [9].
One of the psychological hypotheses concerning ASD is the empathizing-systemizing theory put forward by Baron-Cohen [10], and it is widely supported by researchers [10,16-28]. The empathizing systemizing theory explains the function of the brain using two concepts: empathizing and systemizing [29]. Empathizing is the ability to identify and respond to the feelings and thoughts of others with appropriate emotions, while systemizing is the ability to analyze changes in the system [29]. According to this theory, individuals with ASD tend to be more systemized and less empathizing [17,18,28]. This theory is supported from a cognitive-neurological perspective, as empathizing is positively correlated with the volume of gray matter in the left precentral gyrus, inferior frontal gyrus, superior temporal gyrus, and insula, which are regions responsible for empathy, and systemizing is negatively correlated with the volume of gray matter in the left posterior parietal cortex, which is involved in selective attention [22].
Since ASD is characterized by atypical development [13] and incurability [11], the treatment goal is to promote socially acceptable and supportive behaviors and improve daily life and social functioning while respecting the characteristics of the condition [30].
Interventions for adolescents with ASD have been undertaken with the aims of (1) reducing harmful behaviors, (2) improving social and cognitive skills, and (3) promoting child development[31,32] with a focus on communication and social skills, social imitation skills, cognitive skills, adaptive behavior skills, companionship, acceptance of disability, and employment assistance [33-35]. Against this backdrop, interventions that capitalize on the characteristics of ASD are effective[36,37], and supporters should encourage individuals with ASD to become aware of the strengths associated their condition and build relationships that can help enhance their strengths [11,38].
Puberty is an important period in which the development of metacognition and verbal skills leads to self-control and self establishment [39]. Metacognition refers to the recognition of one’s own thinking and the ability to see oneself objectively [40]. It has been noted that the development of metacognition is slower in individuals with ASD than in those with typical development [30] and that individuals with ASD are not good at metacognition and cannot form self-identity, which leads to confusion.
Since around 2000, a focus on strengths has been gaining attention in regard to understanding an individual’s characteristics, experiences, and talents [41]. Focusing on strength is an alternative to the conventional method of psychiatric care, which focuses only on the negative aspects of patients and society [42]. Everyone has strengths, and they comprise, among other things, talents, knowledge, abilities, and resources [43]. However, some are not aware of their strengths. By working with them to find their strengths and providing assistance, supporters can help them overcome their symptoms and obstacles and live by their own values [42]. Accordingly, for those with ASD to resolve their difficulties in living, it is necessary for them to become aware of their own strengths through metacognition [44].
Individuals with ASD have been reported to have low selfesteem due to their ASD-associated characteristics and poor mental condition and confusion during adolescence [45]. Although it is not easy to increase self-esteem, it has been suggested that self-esteem can be restored by focusing on metacognition and strengths [46].
We therefore conducted a pilot study to evaluate an intervention for adolescents with ASD to improve their self-esteem by promoting metacognition and strength awareness.
3. Methods
3.1 Participants
This study involved adolescents aged 12 to 18 years (IQ ≥ 70) who were diagnosed with or suspected to have ASD according to the diagnostic criteria of DSM-5 at a Japanese hospital with an adolescent psychiatric ward. Thirteen adolescents agreed to the purpose of the study and were eligible to participate, as judged by their treating physicians. Of these 13 adolescents, 12 (6 boys and 6 girls; 5 junior high school students and 7 high school students) completed the program. Although the number of participants in this study is small, there is also a nursing intervention study [47] that verifies the effect with N = 10, so we decided to examine N = 12 in this study.
3.2 Intervention procedure
With a view to reducing the duration of patients’ hospital stays and maintaining the effect, the program consisted of five sessions (45 to 60 minutes each) that were carried out once or twice a week.
The program was performed for each adolescent separately, as individuals with ASD often exhibit uneasiness when finding themselves in an environment where a group of others is present [10].
3.3 First session
The first session, entitled “Understanding the characteristics of the brain,” was aimed at building relationships, making thinking flexible, facilitating the initiation of the program, and recognizing environmental strengths. In keeping with the empathizingsystemizing theory [29], an explanation was given that the brain can be categorized into different types, as exemplified typically by right- and left-handedness [48]. The explanation went on to show that individuals with a certain type of brain may have difficulty living their lives. Specifically, we told them that there are types in the brain, just like gender and blood type, and explained the empathizingsystemizing theory. In this theory, we explained that the brain is divided into types based on the balance of the two axes of empathizing and systemizing. We told them that they could find out about their brain type by administering the questionnaire in the next session. In this way, we motivated them for the next session.
3.4 Second session
The second session, entitled “Understanding your type,” was aimed at encouraging metacognitive activity and raising awareness of the strengths of one’s disposition and character. The Japanese version of the empathy/systemizing quotient (EQ-SQ) questionnaire created by Wakabayashi et al. [25] (originally developed by Baron-Cohen et al. [49] and Baron-Cohen and Wheelwright [50]) was used, with the permission of Wakabayashi et al., to encourage metacognitive activity among the participants. The EQ-SQ questionnaire was formulated in line with the empathizing-systemizing theory, and it allows participants to monitor themselves by answering questions. In this session, after administering the EQ-SQ questionnaire, the participants were asked about the items in the questionnaire that had caught their attention. We then asked the participants about their likes, interests, and concerns. In this way, we tried to externalize the strength of the participants.
3.5 Third session
The third session, entitled “Thinking about hospitalization,” was aimed at encouraging metacognitive activity and raising awareness of the strengths of one’s disposition and character. The results of the EQ-SQ questionnaire were presented visually so that the participants were able to learn their brain type. They were also encouraged to reflect on the event that had led to their hospitalization and discuss with a nurse the relation between the event and their brain type. In this conversation, the participants were informed that atypical development has both favorable and unfavorable characteristics. In this session, we explained the brain type of the participants revealed by the EQ-SQ questionnaire, and asked them if there was any matching part in their behavior and life. They were also prompted to reflect on the circumstances and reasons that led to their hospitalization, based on their own brain types.
3.6 Fourth session
The fourth session was aimed at encouraging metacognitive activity and raising awareness of strengths concerning skills and talents. After an explanation was given on the development of the brain, examples of historical figures with features of ASD were cited, along with their life events and associated strengths, weaknesses, and excellence, with reference to James [51]. In this way, the participants were made to understand that the characteristics of atypical development might serve as excellent talents that can be used to contribute to society [52], and they were made aware of the strengths relating to their own talents and skills so that they could view themselves positively. One of the great historical figures used in this session was Albert Einstein. He is well known to be a prominent and distinguished physicist. On the other hand, he had difficulty with interpersonal interactions during his childhood, and he had the experience of failing the entrance exam. We explained these things using worksheets. The participants were then asked to write down what they felt and thought.
3.7 Fifth session
The fifth session, entitled “Reflect on yourself,” was aimed at encouraging metacognitive activity and raising awareness of the strengths concerning interests and ambition, as well as environmental strengths. While reviewing the worksheets they had worked on, the participants wrote down their own characteristics on another worksheet and noticed that they had strengths as favorable characteristics. They were also asked to talk about their future dreams to help raise their awareness of their strengths concerning interests and ambition. Many participants had dreams of working in the future. For example, system engineers, game creators, robot engineers, railroad workers, librarians, school teachers, nursery teachers, caregivers, beauticians, factory workers, and amusement park workers. The nurse commended them for having their own dreams. We explained that the ward nurses would be their supporters as they pursued their dreams.
4. Measures
4.1 Characteristics of the participants
Information about sex, age, grade, diagnosis, and hospital admission were collected for each participant, as was their autismspectrum quotient (AQ).
4.2 Evaluation of metacognition
The metacognition scale of Abe and Ida [53] was used to measure each participant’s metacognition. Abe and Ida [53] translated the metacognition scale created by Schraw and Dennison [54] into Japanese, conducted exploratory and confirmatory factor analyses, and created a 28-item, three-factor structure covering “monitoring,” “control,” and “metacognitive knowledge.” This is an internally consistent measure, with the reliability coefficients for the three factors ranging from α = .749 to .878. In this six-point scale, higher scores indicate higher metacognition.
4.3 Evaluation of strength awareness
Strengths are the favorable characteristics and advantages of an individual, such as talent, knowledge, and ability, and they represent an individual’s positive aspects [42]. Accordingly, we used the selfdomain of the self-affirmation scale created by Hiraishi [55] to measure strength awareness. It consists of 19 items under three subscales: “selfacceptance,” “self-actualizing attitude,” and “fulfillment.” There was internal consistency, as the reliability of the subscales ranged from α = .69 to .87. In this five-point scale, higher scores indicate higher strength awareness
4.4 Evaluation of self-esteem
The Japanese version of the Rosenberg self-esteem scale (RSES-J), which was originally developed by Rosenberg [56] and has been translated by Mimura and Griffiths [57], was used for self-esteem measurement. The RSES-J was checked for reliability and validity by Uchida and Ueno [58].
This four-point scale is stable and internally consistent, with a reliability of α = .81, as measured in a Japanese survey [58]. Higher scores indicate higher self-esteem.
4.5 Ethical considerations
For the sake of the protection of the participants’ human rights, this study was conducted with the approval of the ethics committees of the Faculty of Medicine at the University of Tsukuba and the study site. Because this study involved minors (junior high and high school students), we first explained the study to their guardians. Only when the guardians gave written consent did we provide explanations about the study to the adolescents and obtain their assent in writing.
4.6 Data collection and analysi
Data were collected between November 2016 and August 2017. The study participants were referred by physicians and nurses in the adolescent psychiatric ward; they were judged by their treating physicians to be eligible for participation, and they provided assent for participation (as did their guardians). Metacognition, selfaffirmation, and self-esteem scales were administered before and after the intervention. Cronbach's α coefficient was calculated to examine the internal consistency of each scale. The Wilcoxon signed-rank test was used to compare the results of the scales before and after the intervention. Absolute values were used for effect sizes before and after the intervention and were calculated as positive values. Statistical analysis was performed using IBM SPSS Statistics, version 24, with the significance level set at 5%.
5. Results
5.1 Description of samples
The mean age of the participants was 15.0 years (SD = 1.7). The mean duration of participants’ hospital stays until the date of the survey prior to the initiation of the intervention program was 14.5 days (SD = 14.4). The mean total AQ was 27.9 (SD = 6.0). The mean number of days required for the program was 19.0 (SD = 8.2), and the mean duration of individual sessions was 42.5 minutes (SD = 11.1).
5.2 Evaluation of the intervention program
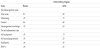
Cronbach's alpha coefficients for each scale are shown in Table 1. The alpha coefficients for the individual scales ranged from α = .65 to .95, indicating that the reliability of the scales was ensured.
On the metacognition scale, the mean total score was 3.3 (SD = 0.8) and 3.8 (SD = 0.8) before and after the intervention program, respectively, showing higher scores after the intervention program (Z = -2.4, p = .02) with an effect size of r = .68. Among the subscales, monitoring and control showed a large effect size, with higher scores after the intervention program, while metacognitive knowledge showed a moderate effect size, without a significant difference (Table 2).
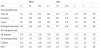
On the self-affirmation scale, the mean score for “self-acceptance” was 11.9 (SD = 4.8) and 14.7 (SD = 3.8) before and after the intervention program, respectively, showing higher scores with a large effect size after the intervention program (Z = -2.1, p = .03, r = .62). The mean score for “self-actualizing attitude” was 22.8 (SD = 7.5) and 25.9 (SD = 6.3) before and after the intervention program, respectively, showing a moderate effect size without a significant difference (Z = -1.3, p = .20, r = .37). The mean score for “fulfillment” was 20.3 (SD = 6.8) and 27.0 (SD = 8.8) before and after the intervention program, respectively, showing higher scores with a large effect size after the intervention program (Z = -2.4, p = .02, r = .70).
The mean RSES-J score was 20.5 (SD = 5.8) and 23.8 (SD = 6.3) before and after the intervention program, respectively, showing higher scores with a large effect size after the intervention program (Z = -2.2, p = .03, r = .65).
6. Discussion
6.1 Characteristics of participants
The gender of the participants in this study was 6 boys and 6 girls, and the grade level of school was 5 junior high school students and 7 high school students, with no gender or grade level bias. Considering that the mean AQ score in this study was 27.92, which was higher than the cutoff score of 25 on the AQ Children's Version, it was inferred that the participants had autistic spectrum disorder characteristics at the clinical range level, but not significantly high.
6.2 Changes in metacognition
Changes in the metacognition scale before and after the nursing intervention program showed that the effect sizes were moderate or higher for the total metacognitive score and all subscales of "monitoring," "control," and "metacognitive knowledge". There was also a significant increase in scores on the total metacognition scale and on "monitoring" and "control". The metacognition scale used in this study was composed of content related to adult learning ability [53]. Although the nursing intervention program used in this study was not an intervention based on learning theory but on a strength model, the intervention was found to be effective. "Monitoring" is a reflective monitoring of cognitive activities during and after the task is completed, through self-reflection, checks and evaluations. In the nursing intervention program, the involvement of self-reflection prompted monitoring behavior. And it was thought that the score increased.
6.3 Changes in strength awareness
As for the self-affirmation scale, an increase in scores was observed in "self-acceptance" and "fulfillment", and the effect size was moderate or higher in all subscales. "Self-acceptance" is an evaluation or awareness of the positive aspects of the self, and is considered to be an evaluation of an individual's awareness of his or her own nature, character, skills, and talents within Strengths. This subscale consists of items that accept and value one's individuality and recognize one's own way of life [55]. It has been noted that individuals with ASD become aware of the differences between self and others as they grow up, perceive themselves as being different from typically developed individuals, and are unable to accept their own characteristics [5]. Before the start of the nursing intervention program, the scores were lower than in the previous study, but after the nursing intervention program, the scores increased to the same level as in the previous study. This was thought to be due to the positive attention the participants received in the nursing intervention program and the nurses' repeated use of praise, which helped the participants to focus on the positive aspects of themselves [42].
6.4 Changes in metacognition
"Fulfillment" was thought to be an evaluation of the emotional aspects of the positive aspects of the self and an evaluation of feelings about Strength as a whole [55]. This subscale consists of items that measure whether one perceives one's life and living as fulfilling. The score before the nursing intervention program was lower than that of Hiraishi [55] and other previous studies. However, after the nursing intervention program, the average scores increased to the same or higher than the previous studies, and the effect size was large. This suggests that those who did not feel fulfilled before the nursing intervention program began to focus on the positive aspects of self and to feel fulfilled by the nursing intervention program.
6.5 Changes in self-esteem
The RSES-J increased before and after the nursing intervention program, and the effect size was large. The RSES-J scores before the nursing intervention program were lower than in previous studies [58-60]. After the nursing intervention program, scores were higher than the average scores of junior high school students receiving treatment in adolescent psychiatry. Self-esteem in adolescence has been shown to be lower with each grade level [59], and it is estimated that the self-esteem of high school students receiving treatment in adolescent psychiatry is lower than that of junior high school students [60]. From these findings, it was inferred that junior high and high school students with ASD who had low self-esteem increased their self-esteem and were able to increase their self-esteem more than other adolescent psychiatric patients due to the nursing intervention program.
6.6 Intervention program for adolescents with ASD
Developmental issues in puberty include “independence from parents” and "self-discovery and self-formation”, and what becomes important in this context is relationships with other children of the same age [61]. However, adolescents with ASD who have a low empathizing ability often do not fit in well with their peers and become isolated. Therefore, in this program, we intentionally treated the participants and took their remarks in such a positive way that they could experience a situation in which they were free to make whatever remarks they desired [42]. This not only created an environment in which metacognition could readily take place, but it also provided the experience of talking to and being affirmed by others (nurses). We believe that this experience was meaningful for the hospitalized adolescents with ASD because they were able to interact with others, albeit not with other children of the same age. In addition, our framework was organized in a way that was suitable for systemization, and it used visualizations in the form of worksheets, which may have been effective for those with ASD since individuals with ASD are good at systemization. During puberty, those with ASD may become aware of differences between themselves and others, which makes them perceive themselves as being peculiar compared with others with typical development, potentially resulting in them becoming unable to accept their own characteristics. In the present study, participants were repeatedly praised within a framework of positive and affirmative communications, and they thus became able to be aware of their strengths while understanding their own characteristics [42].
Our program was thus designed to comprehend the characteristics of ASD based on the empathizing-systemizing theory and to discover the strengths within such characteristics, leading us to conclude that the program is compatible with the characteristics of individuals with ASD.
6.7 Implications
The primary goals in the inpatient care of patients with ASD include improvement of their mental conditions and problematic behaviors, resolution of their inner conflicts and interpersonal relationships, and settlement of their conflicts with family members. Although our program was not aimed at directly achieving these goals, it provided an important intervention, namely enhancing self-esteem, which is crucial for inpatient care, at an early stage of hospitalization. Our results suggest that the intervention program in the present study is useful for treating adolescents with ASD, including those in adolescent psychiatric wards. Individualized care that includes spending ample time with patients and using visual information and tools tailored to the characteristics of individuals with ASD is effective, and giving praise in an affirmative way is important. Based on the characteristics of the adolescent brain, effective nursing interventions can be achieved by stimulating intrinsic rewards and promoting metacognitive activity. This study demonstrated the possibility of using this nursing intervention program in future nursing practice to promote strength awareness and self-esteem of inpatients with ASD.
7. Limitations
As this study enrolled only 12 participants from a single center, the generalizability of our findings is limited. It is necessary to increase the number of study sites and participants to verify the usefulness of the intervention program.
4. Conclusion
This study aimed to determine the usefulness of an intervention program consisting of five sessions to promote metacognition and strength awareness in adolescents with ASD who have been admitted to an adolescent psychiatric ward. The intervention program was implemented in 12 adolescents with ASD, and changes in metacognition, strength awareness, and self-esteem were examined before and after the program. It was found that this intervention program activated metacognition, helped the adolescents become aware of their strengths, and raised self-esteem.
Competing Interests
The authors declare that they have no competing interests.
Author Contributions
TS contributed to the conception of the study and the overall
study process.
ES contributed to the study's program development,
data analysis, and paper writing.
CM oversaw the study's design, data
analysis, paper writing, and the overall study.
Acknowledgments
The authors would like to thank all the participants for their cooperation in this study.