


1. Introduction
Diabetes mellitus (DM) is characterized by chronic hyperglycemia caused by impaired insulin secretion, peripheral insulin resistance, or both [1].
Type 2 DM has been shown to increase the risk for cognitive function [2,3]. People with DM have been shown to have a lower performance on the Mini-Mental State Examination (MMSE) [4].
Vitamin D is a secosteroid associated with peripheral calcium homeostasis and nervous system function [5]. Vitamin D is available in two forms, vitamin D2 from plants and D3 from animals. Both vitamin D2 and D3 are biologically inert and require activation through two hydroxylation processes involving 25-hydrooxylase (CYP2R1) and 1α-hydroxylase (CYP27B1), located in the liver and kidney, respectively [6]. 1, 25-dihydroxyvitamin D (1, 25OHD) is a biologically active metabolite produced by two hydroxylation reaction steps in the nervous system [7].
It has been suggested that vitamin D reduces the risk of type 2 diabetes. In one cohort study, the intake of vitamin D supplements was inversely associated with the development of type 2 diabetes [8]. However, prospective studies have not found an association between 25OHD concentration and cognitive function in DM patients.
Recent evidence has identified a beneficial role of vitamin D in maintaining cognitive functions [9]. Vitamin D receptors and CYP27B1 have been found in the brain (hippocampus) [10]. Low 25-hydroxy vitamin D (25OHD) levels were recently associated with greater risk of cognitive impairment in older as well as younger adults using the Montreal Cognitive Assessment (MoCA) Arabic version [11]. Vitamin D supplementation caused significant improvement in cognitive performance assessed by MMSE score in Alzheimer’s disease [12-14]. In our latest study, a significant positive correlation was found between urinary 25-hydroxy vitamin D (25OHD)/creatinine and MMSE or the Montreal Cognitive Assessment-Japanese version the Montreal Cognitive Assessment-Japanese version (MoCA-J) [15].
There are no data suggesting that vitamin D supplementation may be associated with improved cognitive function in DM patients. Therefore, the present study was designed to investigate the effect of vitamin D3 supplementation corresponding to twice the daily requirement for 9 months on cognitive impairment in elderly diabetic patients in Japan.
2. Materials and Methods
2.1 Subjects and Setting
Prior to the study, approval was obtained from the ethics committee of Kyoto Bunkyo Junior College (project registration number in 2016: 7) and Aichi Medical College for Physical and Occupational Therapy (Project registration number in 2016: 468). We enrolled 6 male and 9 female Japanese patients (age: 74.4 ± 6.2) with controlled diabetes mellitus who attended an outpatient clinic. The researchers were present at the clinic to assure the proper management of safety and confidentiality in the study. The manager of the clinic invited patients to participate in the study, and all the subjects whose participation was requested from September in 2018 to May in 2019 were selected. All subjects took vitamin D supplements (500 IU/day of vitamin D3 purchased from UHA Mikakuto Co., Ltd., Osaka) for 9 months.
2.2 Cognitive function test
MoCA-Jmay be better at detecting early cognitive dysfunction [16] and was used for the cognitive function test. The maximum score for the MoCA-J is 30 points and individuals with a score of 26 points the recommended [12]. The MoCA-Jmay be better at detecting early cognitive dysfunction [16] and was used for the cognitive function test in DM patients [17]. The test was performed by verbal questioning of 5- to 10-min duration by skilled occupational and physical therapists.
2.3 Serum 1, 25OHD, 25OHD and HbA1c Assay
Blood was collected by venipuncture and serum 1,25OHD, 25OHD and HbA1c concentrations were measured bySRL Inc.(Osaka, Japan).
2.4 Statistical analysis
The differences between before and after intervention with vitamin D3 supplements were evaluated using two-way ANOVA or the Friedman test followed by Bartlett analysis for homoscedasticity. A p-value of < 0.05 was considered to be statistically significant. Analyses were carried out using SPSS 21 for Windows (IBM, Japan).
3. Results and Discussion
3.1 Study subjects
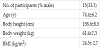
Characteristics of the study subjects are shown in Table 1. Mean age was 71.7 years for males (n = 6) and 76.2 years for females (n = 9). Mean HbA1c was 6.3% for males and 6.9% for females. These values indicated good glycemic control. Obesity was defined as a body-mass index (BMI) of ≥ 25.0 kg/m2. The prevalence of obesity defined by BMI was 16.6% in males and 44.4% in females.
3.2 Change in serum 25OHD, 1, 25OHD and HbA1c
Serum 25OHD was classified as normal (>= 30 ng/ml), insufficient (>20 to 29.9), or deficient (<= 20). In this study, the level was deficient in all except one patient (insufficient). The results from a two-way ANOVA showed that individual 25OHD levels varied significantly from each other (P = 0.004) and by supplementation duration (P = 0.002) (Figure 1). Three month intake of vitamin D3 supplements increased serum 25OHD concentration significantly (p = 0.04) and 9 month intake increased serum 25OHD within the insufficiency and sufficiency levels (5 subjects: > 20 ng/mL and <30 ng/mL, 1 subject: > 30 ng/mL). These results suggest that vitamin D3 supplement intake maintained serum 25OHD levels. A multiple linear regression study revealed an inverse significant association between HbA1c and 25OHD levels [18]. These results suggest that screening for vitamin D status may be beneficial in DM patients.
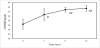
Data are expressed as mean ± SD. # <0.05 vs. 0 time. ##<0.01 vs. 0 time.
Serum HbA1c and 1, 25OHD did not significantly by supplementation duration in the Friedman test. This was assumed to be because all participants had their HbA1c levels checked once a month and was taking medications for treatment of DM.
3.3 Cognitive function
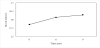
MoCA-J did not vary significantly between individuals (P = 0.12) or by supplementation duration (P = 0.79) in a two-way ANOVA. However, we observed an increase in MoCA-J score after supplementation in 60% of the patients (Figure 2).
Many epidemiological studies have shown that diabetes is a risk factor for cognitive impairment. Recent evidence suggests a potential beneficial role of vitamin D in maintaining cognitive function [8]. In the present study, daily supplementation of 500IU vitamin D3 (serum 25OHD ≤ 30 ng/mL) was associated with a change in cognitive function.
Low vitamin D has been associated with the risk of developing Alzheimer’s disease [12,14]. In the current study, dementia patients treated with vitamin D for 6 months improved their performance on a cognition test (MMSE score) [19]. Over expression of reactive oxygen species (ROS) stimulated by disruption of cerebral blood flow was shown to be one of the main causes of vascular dementia-induced cognitive deficits in a rat model [20]. 1, 25OHD was reported to have significant physiological antioxidant activity [21]. These results suggest a potential role of vitamin D in treating patients with cognitive dysfunction in DM.
Further study of optimal 25OHD levels for maintaining physical and cognitive functions and preventing falls in DM patients is needed.
4. Conclusion
These findings indicate that vitamin D supplementation might improve cognitive function.
Competing Interests
The authors declare that they have no competing interests.
Author Contributions
Dr. Hasegawa was responsible for the study conception, design, and
analysis, interpretation of data, and drafting of the manuscript.
Ms. Mochizuki was responsible for data acquisition and proof
reading of the manuscript, and she participated in the data analysis.
Dr. Yamada was responsible for the data acquisition and proof
reading of the manuscript.
Acknowledgments
The author acknowledges Dr. Yasuaki Fukumoto and Michiko Iwata for then kind help.