


1. Introduction
According to the concept analysis of Henneman, Lee, and Cohen [1], ‘collaboration’ is defined as members considering each other to be a team and participating in planning and decision-making towards a common aim, and contributing as equals.
Recently, as the concept of the team-based medical care spreads, positive Nurse-physician collaboration has been linked to quality of care [2]. As nursing education shifts to university education, the nurse in particular comes to recognise a physician to be a collaborating team member [3].
Conventionally, it was thought that the relationships of healthcare workers had strict hierarchy characteristics by type of job. Freidson [4] named this the ‘hierarchy characteristics of an institutionalized specialized skill’. It is the physician who dominates the top of this hierarchy, and lower-ranked jobs are dependent on a physician for authority and expertise, and relate to the judgement associated with the position in their duties. The perception of collaborative relationships is low for a physician standing at the top of these hierarchy characteristics. Many previous studies point out the following: physicians do not perceive ‘nurse-physician collaboration’ as highly as nurses, and nurses have more value than physicians [5-8].
Regarding the influence on nurse-physician collaboration in patient care, Baggs et al. [9] compared three ICUs and showed that the outcome of the patient was good in the units where nursephysician collaboration was also good. Nurse-physician collaboration is effective, in terms of fewer hospital -acquired infections and shorter length of stay [10,11]. When nurse -physician collaboration is good, it is possible to provide patients with high-quality medical care such as safe care. Furthermore, nurse-physician collaboration has the effect of raising the job satisfaction of nurses and reducing nurses’ turnover rate [12,13].
Nurses can offer high-quality medical care to the patient w h e n the collaborative relationships of nurses and physicians are good. The perception of collaborative relationships of nurse and physician depends on the characteristic of the unit. Nurses practising in surgical units and in emergency departments had positive perceptions of nurse-physician collaboration [14,15].
In this way, while nurse-physician collaboration has been shown to have a large impact on acute medical care, in emergency care in Japan, little research has been performed. Therefore, this research aims to clarify the issue of nurse-physician collaboration in emergency medical care; nurses working in emergency medical centres will be able to clarify when they perceive that a cooperative relationship with the physicians is established.
The Japanese emergency care system is characterised by three levels of care. Primary emergency care treats slightly injured patients, who do not need hospitalisation. Secondary emergency care treats patients who need hospitalisation, but are not in critical condition. Tertiary emergency care treats seriously ill patients in life-threatening emergencies, including ischaemic heart disease, serious trauma, and cerebrovascular disorders.
Tertiary emergency care is the most characteristics of emergency medical care. This study clarified the characteristics of nurse-physician collaboration from the perspective of nurses in a tertiary care facility.
Nurse-physician collaboration is as follows. Nurse and physician relationships are in parallel as experts; they decide to be active in considering each other to be a team, and they participate in planning and decision-making towards a common aim to solve the patient’s problem.
2. Materials and Methods
Before this study, we performed a preliminary investigation for designing the questionnaire.
2.1 Summary of the preliminary investigation
An interview investigation was performed by semi-constitutive questionnaire. The subjects worked in a tertiary care facility and consisted of 19 nurses with more than three years of emergency nursing experience. The questionnaire contents were designed to determine when the nurse-physician collaboration is established. We extracted the situation and made a word-for-word record then expressed nurse-physician collaboration from the interview contents. As a result, 607 sentences were extracted. Having classified 607 sentences based on similarity, 155 threads were found, which formed the basis of the contents of the questionnaire in this study.
2.2 Participants and procedures
2.2.1 Participants
This investigation was conducted on a sample of 1318 nurses from 160 facilities in 32 emergency care centres in Japan, who agreed to participate in the study.
2.2.2 Procedures and data analysis
This was a quantitative, exploratory study performed by a selfcompleted inventory survey that was made based on the preliminary investigation, and the answers were returned by mail. Responses to the items were arranged on a five-point Likert scale ranging from 1 (low collaboration) to 5 (high collaboration). Exploratory factor analysis and reliability testing were conducted on the questionnaire. The analysis software used IBM SPSS Statistics (version 21).
This investigation was undertaken in 2010. The study was approved by the Department of Nursing, Osaka Prefecture University Ethics Review Board. Participants were informed of the purpose and methods of the study, as well as the risks/benefits of participation, the confidentiality of their data, and the voluntary nature of their participation. Return of the anonymous questionnaires was taken as informed consent.
3. Results and Discussion
Participants: We received replies from 561 people (42.6% recovery rate), and 461 of those provided effective answers (34.9%). The summary of the participants is shown in Table 1. Of these, 92.19% were female; the average age of the participants was 34.3 years (SD: 8.0); and the mean years of experience at an emergency care centre were 4.6 years (SD: 3.99). The nursing educational background consisted of 347 technical schools (75.27%), 45 junior colleges (9.76%), and 61 four-year university degrees (13.23%).

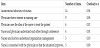
Nurse-physician collaboration perceived by nurses at emergency care centres in Japan: An exploratory factor analysis was implemented, using principal factor analysis with promax rotation in 155 threads. These records were made avoiding abstraction as much as possible, so that many records were produced. Therefore, in this study, the minimum factor loading was set at 6.0. As a result, the records finally became 39 characteristic items in 6 factors (Table 2). The six factors explained 64.807% of variance. The first factor comprised 14 items and was named ‘Autonomous behaviour of nurses’. The second factor comprised 9 items and was named ‘Physician shows interest in nursing care’. The third factor comprised 6 items and was named ‘Physician uses the idea of the nurse to treat the patient’. The fourth factor comprised 4 items and was named ‘Nurse and physician understand each other through conferring. The fifth factor comprised 3 items and was named ‘Nurses and physicians understand organisation management’. The sixth factor comprised 3 items and was named ‘Nurse is concerned with the physician so that the situation improves’. Cronbach’s Alpha coefficient, according to the whole of 39 items standard and the lower standard is shown in Table 3. Its range was identified as having a reliability of 0.94 from 0.89.

3.1 Results
Six characteristics of the nurse-physician collaboration were perceived by nurses; the factors were expressed at four sides. The first aspect is ‘Autonomous behavior of nurses’. The second is ‘Physicians’ attitude towards nurses’. Included in this are the indicators ‘Physician shows interest in nursing care’ and ‘Physician uses the idea of the nurse to treat the patient’. The third aspect is ‘Nurses’ attitudes towards physicians’. Included in this is ‘Nurse is concerned with the physician so that the situation improves’. The last aspect is ‘Attitude as a team of physician and the nurse’. Included in this are the indicators ‘Nurses and physicians understand each other through conference’ and ‘Nurses and physicians understand organisation management’.
3.2 Autonomous behaviour of nurses
The results show when and how nurses positively propose their ideas and are working in teamwork with physicians. Particularly, the autonomous behaviour related to physical assessment. What is described about respiratory management is a scene where nurses frequently intervene on a daily basis. Benner [16] described an opinion as follows. Rather than mechanically carrying out the physician’s orders, the nurse is expected to assess what they should do to provide the best possible care for a patient. There are many seriously ill patients in emergency care centres; therefore, the fact that nurses are able to act autonomously, without a physician’s instructions, affects the patient’s life. It is a characteristic of emergency care centres that there are many autonomous behaviours and codes related to physical assessment. The nurse-physician collaboration is most effective in this area.
Georgiou, Papathanassoglou and Pavlakis [17] reported that nurse-physician collaboration and nurse autonomy are related. ‘Collaboration’ is defined as members who together plan care towards common goals; so, the autonomy of nurses is necessary. However, in Japan, as a nurse practices under the supervision of a physician, the autonomous behavior of nurses is dependent on the ability of individual nurses.
3.3 Physicians’ attitude towards nursing
In this study, what the physicians showed interest in concerned ease, pain, living, family, etc as perceived by nurses. According to the Japanese Medical Practitioner Act, the role of the physician is the diagnosis and treatment of an illness. The role of nurses is, according to the ‘Act on Public Health Nurses, Midwifes and Nurses’ in Japan, assistance to the practice of the physician and the support of the existing medical treatment. Robinson, Gorman, Slimmer, and Yudkowsky [18] pointed out that a physician may only recognise a nurse in the role of implementing a physician’s instructions. There is a lack of understanding about the unique professional role of nurses. The unique role of the nurse is to support the patient as a living person and to improve the patient’s quality of life; for the nurse, treatment assistance is only a part of their role. Considering the results of this study, it seems that the physicians were interested in the QOL of the patient, so they came to understand the care provided by the nurse.
3.4 Nurses’ attitude towards physicians
The following two categories became clear once nurses’ attitudes towards physicians were investigated. One of these was the situation for nurses to act to read physician’s mind. Regarding this, the occupational power balance resides in the different authority of nurses and physicians [19,20]. Stein [21] mentioned a unique communication style between the physician and the nurse, a ‘physician-nurse game’, in which nurses follow rules that do not threaten the authority structure of physicians.
Specifically, though nurses give opinions and advice to the physician, the nurses maintain a passive attitude and behave as if they are respecting the authority of the physician. When the nurse adheres to such rules of the game and the game goes well, as a reward of the game, they gain confidence and satisfaction, and the physician’s authority is not challenged and gains useful information.
Based on this rule, nurses behave like to make the situation better. It may be that nurses are demonstrating autonomous behaviour as much as possible within their power balance position. Although this is not unusual in Japanese healthcare settings, in emergency care centres, nurses and physicians communicate well, so there are many opportunities for ‘doctor-nurse games’.
3.5 Attitude as a team of physician and the nurse
One of the elements demonstrated here is the communication between nurses and physicians. A communication error between the nurse and the physician may lead to a medical error [22]. Communication is an important and influential factor of the cooperative relationship between physicians and nurses [23]. Good communication is indispensable for team medicine. Schmalenberg and Kramer [24] reported that face-to-face communication between the nurse and the physician improves the communication process. Physicians and nurses conferring, as shown in this study, is an active communication method, the importance of communication was shown.
In addition, it can be understood that physicians and nurses who are members of an organisation understand the organisation’s policies and philosophies, and that the instruction system is clearly a part of the effective management of the organisation. Organisation management can be considered to have an effect on cooperation. In the case of a nurse, there are reports that commitment to the care unit has a significant positive effect on the attitude towards collaboration among professionals [25], so that nurse-physician collaboration should be regarded as a concern for the whole organisation.
3.6 Issues of ‘nurse–physician collaboration’
From the characteristics of these six collaborations, three issues are pointed out in the research of nurse-physician collaboration at emergency care centres. The first issue is that the relationship between nurses and physicians is still dependent and dominant. This is affected by the autonomy of the nurse. If the autonomy of the nurse is low, they have to depend on the physician to perform their duties (excluding legal subordination), but, if the ability of nurses to perform autonomous behavior increases, they can work together with physicians as team members. In a sense, ‘concern’ for a physician performed by a nurse is, in a sense, a negative autonomy. Nurses need more education to further strengthen their professionalism and autonomy.
Secondly, along with changes to society, it is difficult to respond at the field level. Certainly, health policy is improving, but people practising are not yet fully aware of the changes. With the ageing rate now increasing, the way people think about the value of health has changed; it is no longer possible to deal with only acute care in this way. When patients receive emergency medical care, it is necessary to practise emergency medical care with a focus on the quality of life of patients, both during hospitalisation and after the emergency medical care has ended. Collaboration is established by the professionalism of individual experts. Both nurses and physicians need to reaffirm the basics, that an intention to combine each other’s professional qualities has benefits to improve the QOL of patients.
The third issue is that autonomy alone is not enough for nurses to be able to collaborate fully with physicians. There are problems in the education and legal systems, which must be improved. An educational programme has already begun in collaboration with nursing students, medical students, new nurses, and resident physicians [26,27]. There are a few places in Japan that still need work; from now on, education on collaboration will need to be addressed throughout the country. In addition, nurses need to promote reform in the education and legal systems, to strengthen their professionalism and autonomy.
4. Conclusions
In this study, the characteristics of nurse-physician collaboration were clarified from the perspective of nurses in tertiary care facilities. We distributed 1,318 questionnaires, using a questionnaire with 155 items of nurse-physician collaboration, made from the results of a preliminary investigation. We collected answers from 561 people; the analysis object was 461 people who provided effective answers. We performed a factor analysis by the main factor method, with a promax rotation of about 155 items. Because there were a large number of items, we set and analysed the factor loading to 6.0. As a result, 6 factors became clear.
Six characteristics of nurse-physician collaboration, as perceived by nurses, were expressed into factors at four sides. These were nurses, nurses’ attitudes towards physicians, physicians’ attitudes towards nurses, and attitudes of physicians and nurses’ teams. Regarding issues facing nurse-physician collaboration, there are still dependent dominant relationships between nurses and physicians. In order to encourage the autonomous behaviour of nurses and to enhance practical nursing ability to strengthen expert knowledge and autonomous behaviour, it is necessary to promote reform in the education and legal systems. From the viewpoint of QOL of patients, nurses and physicians must carry out education on collaboration and speciality as students.
5. Limitations
This study captured the relationship of nurse-physician collaboration from the perspective of the nurse, and there is a limit to capturing the situation of collaboration in a tertiary care facility. In the future, it will be necessary to clarify nurse-physician collaboration from the perspective of the physician.
Competing Interests
The authors declare that they have no competing interests.
Author Contributions
Kanako Honda, Emiko Takamizawa were responsible for the study design and manuscript preparation. Kanako Honda were responsible for data collection. Kanako Honda, Emiko Takamizawa were responsible for analysis of data and discussion of findings.
Acknowledgments
We would like to thank the nurses who participated in this study, and to thank the senior nursing officer of each facility that cooperated in this study.
One author, Kanako Honda, who is independent of the commercial funder, had full access to all the data and takes responsibility for the integrity of the data and analyses.