


1. Background and Significance
Pediatric nurses frequently teach caregivers to care for their ill child in the home environment. When this care involves learning how to operate medical equipment and perform treatments and procedures, it can be very challenging and intimidating for a caregiver. In the majority of hospitals, caregivers are given written materials upon discharge to reinforce education received from a hospital nurse educator. While written materials alone are acceptable for many caregivers, they do not always meet the needs of a growing population of 21st century learners.
A large number of the pediatric family caregivers are falling into the “millennial” generational category. The millennial learners, birth years ranging from 1982 to 2004, have grown up in an era of rapid technological growth [1,2]. They are adept with computers, cell phones, and video games and they connect with friends and family through social networking, text messaging and other technologymediated approaches [1,3]. The repeated exposure to technology has resulted in a group of young adults who have developed an enhanced visual and auditory orientation to learning [1,4,5].
Video instruction is an effective tool to enhance learning and retention of material for the millennial generation. Today’s millennial caregivers embrace engaged learning techniques that are self-paced in contrast to the traditional lecture style methods of instruction [6-9].
The learning styles of the millennial parents, coupled with the growing illiteracy rates are raising concerns about the contemporary relevance of existing methods of skill reinforcement used in patient education [10]. Research indicates health literacy rates are remarkably low in the United States, significantly impacting health care outcomes [11]. Approximately 14 percent of the population is unable to read or understand any written material, with an additional 21 percent reading below a 5th grade level [12].
Health literacy, therefore, is an important predictor of a patient or caregiver’s ability to provide proper care outside the hospital environment [10]. Research supports that low literacy levels are associated with higher mortality rates and more frequent hospital readmissions [13,14]. When video instruction was introduced to groups with low literacy levels there was improvement in the retention of education material [13,15-17] when compared to the use of written instruction alone. The use of video has been found to be an effective learning medium for many patients with a low level of health literacy [18,16,19].
Having a child with a medical need for medical technology is extremely stressful for caregivers and raises anxiety levels. Research has shown that in times of stress and anxiety a person’s IQ score can drop 10-15 points [20]. Consequently, nurse educators must educate the caregiver when they are not at their optimal level of functioning. Numerous studies examined the retention of educational material provided to caregivers of ill children. Key findings were that the caregivers who watched instructional videos had a greater retention of the material. Furthermore, caregivers who watch instructional videos had a higher confidence level in implementing care for their children when compared to caregivers who had received written instructions only [21-23].
Research has shown that videos are useful in parent caregiver education because it increases retention of the educational material [24-26], but no research was found that examined what the caregivers thought about the use of video in parent caregiver education and if they thought it was an appropriate media to learn. The purpose of this study was to examine the use of short video skill clips in discharge education and examine the feasibility, acceptability, and effectiveness of video skill clips to reinforce one-on-one instruction related to the child’s care with the nurse educator and to determine if they increased a caregiver’s confidence in performing medical procedures. Two research questions were addressed: (1) What is the effect of viewing the video skill clips on a caregiver’s confidence to perform the required skill; (2) What is the (a) acceptability, (b) feasibility, and (c) effectiveness of integrating video skill clips in caregiver education prior to the child’s discharge?
2. Design and Methods
The setting for this one- group pretest-posttest designed study was a large urban tertiary care pediatric hospital in the Midwest region of the United States. The hospital serves a diverse population of multiple ethnic and racial groups and a variety of socioeconomic backgrounds. The intervention was twenty one medical procedures performed according to hospital policy were videotaped using an iPad; peer reviewed by pediatric registered nurses and caregivers who served on the hospital Family Advisory Board. The iPad allowed the nurses to produce and edit the medical procedures without the need of an expensive camera crew and the time that would be required for such an endeavor. This method will make future updating of the video skill clips when a procedure change occurs less cumbersome. These video skill clips were made available for caregiver viewing on iPads or the hospital’s inpatient educational learning management system. The video skill clips averaged about two minutes in length, allowing the caregivers to learn the information in small doses.
After obtaining institutional review board approval, the study was conducted in the Family Learning Center (FLC) that provides the majority of complex patient discharge education. Participants were recruited from caregivers that were scheduled to meet with the nurse educator in the FLC for an education session. The participants included primary (n=40) caregivers (biological, adoptive or foster parent, legal guardian, grandparent or any other person who functioned in the role of being the primary caregiver of the child). Study inclusion criteria were caregivers: (a) 18 years of age or older; (b) able to speak and understand English; and who (c) had a child requiring a medical procedure included in the video skill clip collection. Exclusion criteria: caregivers who: (a) were unable to complete the required educational sessions with the nurse educator in the FLC; (b) had viewed a video skill clip or had educational sessions during a previous hospital admission; (c) were professional adult or pediatric healthcare providers themselves. Informed consent was obtained and, study participants were given a five dollar gift card that could be used in the hospital coffee shop as an incentive.
3.1 Measures
No instrument could be found to measure the caregivers’ perception of the feasibility, acceptability, and effectiveness of the video skill clips and their confidence to perform the required medical procedure. A paper and pencil instrument was created by the investigator to gather demographic and pre and post intervention qualitative and quantitative data.
The Caregiver Survey Demographics instrument given prior to viewing the video skill clips included closed ended nominal and open ended questions. The demographic instrument included questions about the caregiver’s sex, age, race/ethnicity, educational level, and previous caregiver experiences.
The Caregiver Video Skill Clip Survey had a pretest and posttest that used a Visual Analog Scale (VAS) format to gather responses of the caregivers. The scale was selected as a measurement tool for this study because it allows for measurement of a characteristic or attitude that is believed to range across a continuum of values or feelings that is difficult to measure. The VAS scale is an unnumbered 100 millimeters line. Each end point of the line was clearly marked description of “a little” at the left of the line and “a lot” at the right end of the line. Each question provided space for caregiver comments. The pretest consisted of only the VAS style questions while the posttest included VAS style questions plus dichotomous yes/no questions.
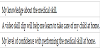
The pretest survey included three questions (Table 1) that queried caregivers about the usefulness of the video skill clips in the care of their child, previous knowledge about the skill and their confidence level in regards to performing the medical procedure on their child in the home environment.
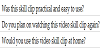
The posttest included questions (Table 2) about the usefulness of the medical skill clip, caregiver opinion about the length and effectiveness of the video skill clip in discharge teaching and caregiver confidence to perform the medical procedure after viewing the video skill clips.
2.2 Data collection procedures
An appointment was made with the caregiver, at their convenience, to meet for the research session with the Principal Investigator (PI). Survey completion took an average of 15 minutes of the caregiver’s time. During this meeting consent was first obtained verbally for participation in the study. The Caregiver Survey Demographics instrument and the Caregiver Video Skill Clip Survey Pretest. The caregiver then viewed the video skill clip that pertained to the medical procedure that they would be required to perform on their child at home. After viewing the video skill clip the Caregiver Video Skill Clip Survey Posttest was administered.
Following the intervention session using the video skill clip with the PI, the caregiver partook in an educational session with the FLC nurse educator to assure that educational needs and concerns had been met. The FLC educators offered written instruction and provided demonstrations of the required medical procedures for all of the caregivers involved in the study.
2.3 Analysis
Data were entered and analyzed using SPSS Statistics 24 Premium software. Data were cleaned and checked for accuracy. A paired T – test was used to compare the means for the first three questions of the pretest/ post-test. Qualitative data from comment sections for each survey question was extracted and analyzed using content analysis to provide participant insights to the video skill clips and ways they might be improved. The quantitative data was analyzed using the descriptive statistics (mean, mode, median, standard deviation).
2.4 Conceptual Framework
The middle -range theory of Facilitated Sense- Making by Judy Davidson guided this study [27]. Davidson purports that illness interferes with the normal functioning of a family unit [27]. When a family experiences a crisis such as one of its members experiencing illness, it may result in a disruption of family functioning. Family members need to make sense of the situation and the role changes that may occur in the family unit due to the illness. In addition, family members need to discover what their new roles will be in regards to this disruption and how they will function and cope with changes [27]. Sense-making is facilitated when the nurse provides information to the family so that they can interpret the situation and find solutions that allow them to adjust to what is happening around them. The video skill clips can be used as an intervention to assist caregivers in making sense of their new roles by providing them with visual educational materials that are concrete and focused on the necessary medical procedures needed to care for their child.
3. Results
Participants in the study (N= 40) were primarily biological mothers/fathers (n= 35, 87.5%) of children who were experiencing their first hospitalization and had no past knowledge of the medical procedure featured in the video skill clip (n=32, 80%). The age of the mothers/fathers ranged from 21 to 54 years (M= 32.7, SD= 1.5).
Other caregivers in the study represented (n=5, 12.5%) and were composed of aunts and grandparents. The race of the caregivers was predominately Caucasian- non -Hispanic (n=26, 65%); however, the percentage of caregivers from other races represented were African American (n=12, 30%) and Biracial (n=2, 5%).
Most of the caregivers were married (n=18, 45 %,) but others identified as single and or never married (n=15, 37.5%), single and living with a partner (n= 5, 12.5%), divorced (n=2, 5%). A majority said the child’s other parent would assist with care of the child (n=37, 92.5%).
The caregivers represented a variety of educational backgrounds, but a majority (n=15, 37.5%) had at least a High School Education or GED, whereas other caregivers in the study listed their education as having attend some college courses (n=8, 20%), Vocational School (n= 2, 5%), Bachelor degree (n=6, 15%) and Graduate degree (n=9, 22.5%).
The mean age of the children requiring the medical procedure was 2.48 years (SD= 1.32), ranging in age from 4 days old to 15 years of age. The primary diagnosis for the majority of children was related to Gastrointestinal conditions (n=10, 25%) or new onset Diabetes (n=7, 17.5%). Other conditions included complications associated with preterm births (n=6, 15%), cardiac conditions (n= 5, 12.5%), respiratory conditions (n=4, 10%), neurological issues (n=3, 7.5%), muscular disorders (n=3, 7.5%), cancer (n=1, 2.5%) and unknown (n=1, 2.5%).
Twenty-one video skill clips were available for viewing; nasogastric tube insertion was the most frequently viewed in this study (n=10, 25%). Other video skill clips viewed were PICC line flushing (n=7, 17.5%), subcutaneous injections (n=7, 17.5%), gastric tube care (n=7, 17.5%), hand washing (n=4, 10%), intra-tracheal suctioning (n=4, 10%) and central line dressing change (n=1, 2.5%).
Caregiver level of confidence in performing the medical procedure at home on their child was measured before and after watching the video skill clips. The survey results (Table 3) indicate that the video skill clips significantly increased the confidence of the caregivers (p<.001). Pretest comments related to confidence included: “eek! So not sure about taking the best care of my lil one.” Posttest comments reflected the increased confidence of the caregiver, “The clip made me feel more confident. I like the idea of being able to review the procedure before I do it. Even after doing something like this several times, it’s probably easy to forget the exact steps.”



Caregiver knowledge of the medical procedure was examined before and after the video skill clip intervention. There was a significant increase in their knowledge of the skill they were required to learn (p=<.001). Comments included that, “Nurses have begun to show me how to listen for the air pop after feeding,” indicating teaching had begun on the patient unit prior to viewing the video skill clip (Table 3). Other comments were positive, “After watching the clip I can do that.”
Caregivers were also asked if the video skill clip assisted them in learning the skill (Table 3). The paired T-test scores indicate that after viewing the video skill clips there was significant increase in how the caregivers felt their learning to care for their child in the home environment (p=.045) improved.
Acceptability and feasibility (Tables 4 & 5) was assessed by examining the results of the post-test which showed that caregivers would use the skill clip at home (n=36, 90%), thought the video clip length was just right (n=40, 100%), and thought the skill clip was practical and easy to use (n=40, M= 94.15, SD 6.84).
In this study, the video skill clips were available in the hospital to view via iPad or on the hospital learning management system. Plans were in the works for caregivers to take the video skill clip home on a DVD for repeat viewing. Participants in the study suggested that the video skill clips be e-mailed or texted so that the procedure could be watched over a smart phone or iPad verses the DVD for home use. The use of e-mailed video skill clip links is currently being investigated by the hospital legal department.
4. Discussion
Methods used to educate patients should be evidence -based and relevant to today’s learner with documented effectiveness. This study contributes to the state of the science related to the use of video skill clips to reinforce pediatric patient education. One of the goals of family-centered care is to provide caregivers with the tools and confidence needed to care for their child in the home environment.
The study results will aide nurse educators in viewing discharge education from the perspective of the caregiver and encourage the use of video skill clips as a feasible, acceptable and effective teaching method for patient instruction.
While previous research focused on the use of video instruction in caregiver education, there is a paucity of pertinent literature that examines the use of the video skill clips to increase caregiver confidence in performing medical procedures for their child as well as the feasibility, acceptability, and effectiveness of video skill clips. It has been well documented that the use of video instruction in patient education has assisted in the acquisition and retention of knowledgewhen compared to written materials alone [21,23,16,26], but little was found in the literature to support if the caregivers found the method of instruction acceptable, feasible, or effective. This study gathered information from caregivers to address what they thought of the feasibility, acceptability, and effectiveness of video skill clips to learn medical procedures.
There were several limitations to this study. First, study participants were recruited from one hospital which limits the generalizability of the findings. Second, the study sample included mostly Caucasian female caregivers with at least a high school education. Another limitation was the small sample size (n=40).
Future studies could be performed to explore the long term impact of using video skill clips. Caregivers could be followed over time to examine if utilizing the video skill clip sat home to perform medical procedures lessened the likelihood of an extra doctor’s office visit, emergency room trip or readmission to the hospital.
5. Practice Implications
Video skill clips are an excellent teaching tool for caregivers who learn best through visual and auditory methods; particularly those with low literacy levels. They are a highly accessible and efficient tool for caregiver review and self-paced learning, especially during times of stress when learning is not optimal. The use of video skill clips can also be a helpful tool in patient education situations with caregivers who do not speak English. Translation of the video skill clip in other languages would increase caregiver success in performing the medical procedure for their child at home.
The video skill clips would make a wonderful education tool that health care providers could utilize when a quick refresher of a procedure is needed before performing or educating patients about a procedure. They could also serve as an instructional tool for nursing and medical students new to the area of pediatrics.
Competing Interests
The author declare that there is no competing interests regarding the publication of this article.