


1. Introduction
Developing an understanding of the concept positivism is helpful before conducting the concept analysis. What is positivism? The question originally asked by Auguste Comte, the founder of positivism, who embraced the philosophical and political movement [1]. The positive method came in different forms depending on the science where a positive method was applied; for example, in astronomy, a positive method was regarded as observation, in physics as experimentation, and in biology as acomparison [1]. The term positivism was used to express the scientific approach to the world [2]. Positivism classifies into three categories of identifiable scientific methods, which were understood to be unitary and positivistic [2]. In addition, another characteristic of positivism was the elimination of metaphysics from philosophy [3].
In Japan, the incidence of breast cancer is increasing, with this malignancy ranking as the most relevant regional cancer for women in 2016 [1]. Treatment of breast cancer is generally performed using a multi-modality approach by combing surgery, radiotherapy, chemotherapy, and/or hormonal therapy [2-4]. Adjuvant therapy is typically administrated to patients with advanced stage breast cancer. The therapeutic agents suitable for treating advanced stage breast cancer include adriamycin cyclophosphamide (AC), fluorouracil epirubicin cyclophosphamide (FEC), docetaxel cyclophosphamide (TC), paclitaxel (PTX), docetaxel (DTX), cyclophosphamidemethotrexate- 5-fluorouracil (CMF), or trastuzumab (HER).
One of side effects of such anti-cancer drugs is lower limb edema and is often induced by DTX. Many patients suffering from such a side effect are frequently complaining of fatigue and difficulty in walking due to this adverse event. The cause of lower limb edema related to breast cancer chemotherapy consists of: excessive fluid administration [5], drug-induced insufficiency of renal function [6], aging, obesity, and decreased activity due to other side effects. To treat lymphedema and lower limb edema in patients undergoing chemotherapy, intermittent pneumatic compression (IPC) is a therapeutic option. Although there has been a report of IPC therapy for lymphedema in breast cancer patients decreasing the volume capacity of the upper extremities [7], the evidence concerning treatment protocols and drainage effects on the lower limb edema are not fully established.
The 5-year survival rate of breast cancer is 90.47% [8], with many patients living with this malignancy for a long time. Therefore, there have been many studies examining the quality of life (QOL) in breast cancer patients [9-11]. The lower limb edema also decreases the health-related QOL (HRQOL) in patients undergoing chemotherapy. Therefore, if IPC is an effective treatment option for the lower limb edema, an improvement in patient HRQOL could be achieved. However, such investigations have not yet been conducted.
The aims of this study were: (1) to clarify the effects of IPC on lower limb edema and HRQOL; and (2) to determine the relevant factors in the breast cancer patients who received adjuvant chemotherapy and IPC for treating the lower limb edema, in an effort to optimize nursing care for such patients in outpatient clinics.
2. Methods
2.1 Study design and sample
A prospective, longitudinal research design was used in this study.
The target population was individuals who: (1) were breast cancer patients undergoing adjuvant chemotherapy; and, (2) had been recommended to treat the lower limb edema in a lymphedema outpatient clinic by a surgeon. The data were obtained at a municipal hospital in Osaka, Japan, between June 2010 and September 2011. This hospital is the regional cancer treatment center: hospital mainly treating the cancer patients in the region. The lymphedema outpatient clinic is operated by a nurse who completed their training on lymphedema under the guidance of a breast surgeon.
There were 32 patients during the study period. All of them were asked to participate in the study, all of which agreed and gave the informed consent.
2.2 Ethics
One of authors in this paper clearly stated the aims and methods of this study, the personal information and answers to the question items were protected, study participation was voluntary, there was no disadvantage in not participating in this study, data usage was limited to this study, and absolute confidentiality of the patients in both oral and written forms was maintained. All study procedures were approved by the Ethics Committee of the Nursing Department of Yao Municipal Hospital.
2.3 Procedure and setting
We confirmed that the participants had no vein thrombosis of the lower extremities via leg echocardiography before implementing the IPC therapy. According to the review of Szolnoky et al., there are many variations to the number of cuffs for IPC, with various thicknesses, total treatment time, number of cycles, and pressing force [12]. In this study, we used the course mode, with a pressure of “4”, for 30 minutes once per week. The course mode means the wave mode is used twice, and the squeeze mode is used twice, with pressurization from the toes to the thighs, and the hyper mode is used once, with all pressurizing chambers activated simultaneously.
Data were obtained at 4 different time points: (1) on the first day of IPC therapy (D); (2) 1 week after implementing IPC therapy (1W); (3) 4 weeks after implementing IPC therapy (4W); and, (4) 12 weeks after implementing IPC therapy (12W). The timing of the measurements was decided by the breast cancer surgeon in consideration of the patient's visit during their hospitalization period.
2.4 Instruments
The participants were interviewed to obtain demographic and clinical data using a questionnaire designed for this study. Each interview was usually no more than 30 minutes.
The collected data included information regarding gender, age (at the initial measurement), employment status, height and body weight, living conditions, stage for breast cancer, operation method, whether or not axillary lymph node (ALN) dissection was performed during surgery, time since surgery, whether or not hormonal therapy was administered, whether or not radiotherapy and/or chemotherapy were administered, and the types of chemotherapy used.
The QOL was estimated using the Japanese version of the World Health Organization Quality of Life Instrument-Short Form (WHOQOL-BREF) assessment [13]. Internal consistency of the Japanese version was sufficient: Cronbach’s α-coefficients ranged from 0.66 to 0.84 [14]. This assessment consists of 26 items and 4 domains: “physical health” (7 items), “psychological health” (6 items), “social relationships” (3 items), and “environment” (8 items). Two additional items measuring overall QOL and general health were used as the “global QOL” domain. Items were rated on a 5-point Likert scale. Cumulative scores for each domain were calculated to make domainspecific scores, with higher scores indicating a better HRQOL [14].
Researchers measured the calf circumference at 5 cm below the knee joint, with ankle circumference also measured using a measure [15]. They also measured the range of motion (ROM) of hip abduction and the flexion of the ankle using a medical angle gaze in the standing position [16].These measurement was performed by a single nurse, who had been trained under the guidance of a physical therapist in advance, in order to minimize measurement error.
2.5 Statistical analysis
All analyses were completed using the Statistical Package for the Statistical Package for the Social Sciences 24 (SPSS, Tokyo, Japan IBM Corp., Armonk, NY, USA). Body mass index (BMI) was calculated from the height and weight of a patient at each measurement session. For multiple comparisons of measured values of the lower limbs, the one-way analysis of variance (ANOVA) was used. If the results of ANOVA indicated significant differences, post hoc analysis was performed with the Dunnett test.
The 5 domain-specific scores of WHOQOL assessment were normally distributed and treated as continuous variables. They were described using the values of mean and standard deviation. Mean domain-specific scores of participants were compared with those of community-dwelling Japanese individuals at the ages of 50-59 years [14] using a non-paired t-test. Those at 12W were compared with those at D using a paired t-test.
We intend to clarify the factors related to the changes in the scores at 12W from the one at D. Therefore, the changes between these two points, 12W-D, were calculated. The relationships between these changes were evaluated using Spearman rank correlation coefficients.
The values subtracting the score at D from the one at 12W were divided into two categories: better improvement (more than the average) and worse improvement (less than the average). These two categories (better improvement: 1, worse improvement: 0) were assigned to the dependent variables in a multiple logistic regression analysis. Table 1 shows the independent variables used to select the variables significantly related to the dependent variable. Dummy variables were created for the independent variables. The independent variables were divided into 2 categories: older than 57 years, employed, overweight (having BMI ≥25), living alone, having stage IIB and more, breast-conserving surgery, undergoing ALN dissection, time after surgery being greater than 1.7 years, undergoing hormonal therapy, undergoing radiotherapy, undergoing chemotherapy using with AC, undergoing chemotherapy with DTX, undergoing chemotherapy with PTX, undergoing chemotherapy with CMF, and undergoing chemotherapy with HER, were all allocated 1 point each. As for calf and ankle circumference, abduction of hip, and flexion of ankle, and the HRQOL scores, values showing a change greater than its average were allocated 1 point each. The other conditions were set to 0 points.

P-values less than 0.05 were considered statistically significant.
3. Results
Table 2 summarizes the demographic and clinical characteristics of the study participants. All participants were females, with ages of 40–60 years-old accounting for 84.3% of the patients. The average age at the time of the initial measurement was 56.3 years. In regards to employment status, 37.5% of the participants were employed. Proportion of participants with BMI over 25 kg/m2 were 56.2%. Those living alone was 34.4%. For the stage, 71.9% of the participants were at advanced stages; stage IIB, IIIA, IIIB and over. For the operation method, 75.0% of the participants received the breast-conserving surgery and 21.9% received ALN dissection. The median time since surgery was 1.7 years. A total of 46.9% of participants received hormonal therapy, and 59.4% of patients received radiotherapy. All participants received chemotherapy, with AC administered to 9 patients (28.1%), DTX to 8 (25.0%), and PTX to 7 (21.9%).

Table 3 shows the changes in the measured values of the lower limbs. The calf and ankle circumferences were larger than the reference values of Japanese women in their 50’s [17] on the first day of IPC therapy, but they were significantly smaller at 1 week after initiation, and the values decreased significantly at 12 weeks after implementing treatment. There was no significant change in abduction of the hip for either side. Ankle flexion for both sides improved significantly at both 1W and 12W.

Table 4 summarizes the change in scores of the 4 domains of the WHOQOL assessment and the global QOL domain. The 4 domainspecific scores of the WHOQOL assessment at D were significantly lower than the mean scores of community-dwelling Japanese individuals at the ages of 50-59 years-old. Scores of all domains were significantly higher at 12W than those at D. However, two domainspecific scores, physical health and global QOL, were still significantly lower than the scores of community-dwelling Japanese individuals.
There was no significant correlation between the 4 measured values and the change in WHOQOL score for 12 W-D.
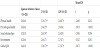
Table 5 summarizes the results of the odds ratios of different factor and their effect on the efficacy of IPC therapy. In regards to the change in ankle circumference, time since surgery and patient age were significant factors. A longer time since surgery was a promoting factor and older age was an inhibitory factor. In respect to the change in “social relationships” and “global” QOL domain scores of the WHOQOL assessment, being overweight was a significant inhibitory factor.

4. Discussion
In this study, we attempted to clarify the effects of IPC on the lower limb edema and WHOHRQOL in 32 breast cancer patients undergoing adjuvant chemotherapy. The lower limb edema was significantly reduced after the first week of IPC therapy. Scores of all domains of WHOQOL were significantly higher at week 12. Time from surgery to the initiation of IPC was a promoting factor and older age was an inhibitory factor for a decreasing ankle circumference. Obesity was an inhibitory factor for the social relationships and global QOL domains of the WHOQOL.
Edema in patients undergoing DTX-based chemotherapy has been reported as a side effect of anti-cancer drugs [18]. In this study, 1/4 of the participants were received chemotherapy using DTX. However, there were also many patients undergoing chemotherapy treatment with AC and PTX. AC is noted to have neuropathy and myalgia as side effects [19]. However, these two anti-cancer drugs have not been reported to cause edema. Even if the frequency of edema caused by chemotherapy is unclear, nurses should pay attention to such possibilities.
In this study, the size of the IPC boots was fixed, and we set pressure of “4,” for 30 minutes once per week. These setting were effective in decreasing edema at the calf and ankle, along with an increase in ankle flexion one week after implementation, although the size of calf and ankle were larger than the reference values of Japanese women after 12 W. The increase in ankle flexion may result in an additional decrease in swelling at this location (Spearman rank correlation coefficients: r=0.268 p=0.138). Although there is no difference between total pressurization and sequential pressurization [20], it is necessary to consider more effective methods, such as IPC settings and treatment duration.
A previous study reported an improvement of QOL, as measured using the Quality of Life Questionnaire for Cancer Patients treated with Anticancer Drugs for Breast Cancer (QOL-ACD-B, version 1.0), 1 year after surgery [21]. However, the HRQOL of our patients, as measured by the WHOQOL assessment, except for the “environmental” domain, were significantly lower than the average of communitydwelling Japanese individuals at the same age although over 1 year after surgery had passed in participants of this study. This might result from the fact that the participants had the lower limb edema due to adjuvant chemotherapy from advanced stage breast cancer.
At 12 weeks after implementing the IPC therapy, patient HRQOL increased to the same levels, except for the “physical health” and “global health” domains. These results were inconsistent with a study that reported the mental and psychological recovery of breast cancer patients was slower than physical improvements [22]. Further study is necessary to clarify the reasons of these inconsistent results.
If the effects of IPC therapy can be predicted for a given patient before implementation, then nurses will be enabled to provide more suitable care. The effectiveness of ankle circumference reduction was related to the time since surgery and patient age. In patients who had the received surgery over 1.7 years, IPC therapy was more effective. Franks et al. found that IPC therapy for lymphedema is more effective in patients with higher skin thickening [23]. Patients who had a long duration between surgery and IPC therapy were assumed to have stronger skin thickening [24]. Since elderly people may spend more time at home, older patients tend to be less active [25]. As physical function decreases over time, IPC therapy might be less effective on the lower limb edema in older patients than in younger patients, though future studies are needed to examine this effect.
Peripheral edema is not a life-threatening side effect, but it does impact patient HRQOL. However, there was no relationship between the change in calf or ankle circumference, hip abduction, or ankle flexion and the domain-specific scores of the WHOQOL assessment. It is difficult to determine if improvement in edema directly affects HRQOL. Therefore, we attempted to find the factors related to an increase in the domain-specific scores of the WHOQOL assessment.
In the “social relationship” domain, obesity was an inhibitory factor, which is intuitive since the obese tend to avoid going out [26]. If obese patients have lower limb edema, this would exacerbate a sedentary lifestyle [27]. In the “global” QOL domain, obesity was also an inhibitory factor for higher QOL scores. Obese patients are usually administrated large amounts of chemotherapy agents; a larger amount of these drugs tends to have more prominent side effects, which may affect the global QOL score.
Based on our findings, it is difficult to predict the effectiveness of IPC therapy. In this study, the same setting was used. It is necessary to devise a setting such as size, pressure, and times. Since obesity is an inhibitory factor to obtain higher HRQOL scores, nurses should provide such patients with continuous support for better HRQOL, including outdoor activities.
The IPC therapy used in this study is a widely distributed product designed for the treatment of lymphedema and lower limb edema in general osteopathy clinics [28]. It may be beneficial for nurses to discuss IPC therapy with patients prior to treatment to build a good nurse-patient relationship, which may improve HRQOL.
5. Limitations
This study had a few limitations. First, this survey was conducted between 2010 and 2011, which may induce some bias as treatments may have been optimized over time. However, the current anti-cancer drugs for breast cancer are still widely used and IPC remains a useful therapy for improving edema of the upper and lower limbs.
Another limitation was that our study population comprised of 32 patients from a single hospital. The measurement was stopped because the nurse who had been trained under the guidance of a physical therapist was moved to another section. Therefore, it is not possible to conclude that our data is representative of most breast cancer patients who were treated with adjuvant chemotherapy. In the future, it is necessary to continuously carry out nursing care using IPC, and to accumulate data for the purpose of establishing the most effective usage of this method.
When the anti-cancer drug used would be different, the condition of the lower limb edema would be different. Further study is necessary with more number of subjects and depending on the kinds of anticancer drugs used.
6. Conclusion
The lower limb edema was significantly reduced after the first week of IPC therapy. Scores of all domains of WHOQOL were significantly higher at week 12. Time from surgery to the initiation of IPC is a promoting factor and older age is an inhibitory factor for a decreasing ankle circumference. In addition, obesity is an inhibitory factor for the social relationships and global QOL domains of the WHOQOL assessment. Nurses in outpatient clinics should be cognizant these factors of a patient’s before implementing IPC therapy to provide optimal nursing care.
Competing Interests
The authors declare that they have no competing interests.
Author Contributions
Chie Furukawa, Ikuharu Morioka were responsible for the study design and manuscript preparation. Chie Furukawa, Takashi Morimoto were responsible for data collection. Chie Furukawa, Takashi Morimoto, Ikuharu Morioka were responsible for analysis of data and discussion of findings.
Acknowledgments
We would like to express our deep gratitude to the participants of this study.