


1. Introduction
Several epidemiological and animal studies are known to demonstrate the adverse health effects and toxicity of anesthetic gases in personnel in the operating room. Vaisman in 1967 [1] published first that fatigue, exhaustion, headache and spontaneous abortion frequently occurred among anesthetic nurses. Fink at al. [2] conducted animal studies showing that nitrous oxide (NO) exposed pregnant rats had embriotoxic and teratogenic effects, ie. increased incidence of sceletal abnormalities and resorption of fetuses. Recently after the detailed analysis of these articles and literature data some experts concluded, that there are no relevant data showing any risk of adverse health effects to personnel in operating rooms [3,4]. In contrast Rowland et al. [5] published cases of reduced fertility and spontaneous abortion among female dental assistants, although in their cases the anesthetic gases were used without proper ventilation and scavenging system. Consequently, there is a need for more epidemiologic studies on health risk of anesthetic gases. Our study shows a new highlight of this problem, approaching the health effect of working conditions on the cytogenetic changes measured on peripherial blood lymphocytes among anesthetic personnel.
2. Material and Methods
2.1 Subjects
Altogether 128 subjects exposed to anesthetic gases were investigated. Their results were compared to 137 healthy controls, occupationally not exposed to known substances. All subjects were interviewed by a physician to collect data on age, medication, smoking and drinking habits, as well as medical and work histories including exposure to known or suspected toxicants, occupational history including duration of exposure, and the use of protective devices during work. The anesthetic gases used in operating theaters were Sevoflurane, Isoflurane, Nitrous oxide, and in some cases Halothane. Additionally, some of the subjects could be exposed to X-rays as well. Active smoker and ex-smoker subjects were considered “Smokers”. “Drinkers” consumed no more than 80 g pure alcohol regularly (a liter of beer or equivalent). With the informed subjects' written permission, blood samples were collected by venipuncture. The samples were processed for genotoxicological analysis and, to assess health status, for a routine clinical check-up including hematology, liver and kidney function tests.
2.2 The determination of UV induced unscheduled DNA synthesis (UDS) in PBLs
The measurement of UDS was made according to Bianchi et al [6], as previously described [7]. Briefly, the separation of PBLs of citrated blood samples was performed by Ficoll-Hypaque density centrifugation. PBLs were irradiated in open petri dishes by UV light (24 J/m2) and then incubated for 3 h with 10 μCi/ml 3H-TdR (activity: 37 MBq/ ml, Amersham) in the absence or presence of 2.5 mM hydroxyurea. The degree of ‘de novo’ UDS was measured by scintillometry based on 3H-TdR incorporation in separated lymphocytes. UDS was calculated as the difference between radioactivities of the incorporated 3H-TdR in UV irradiated and control cultures (relative units). Normal values of UDS are in the range of 4,0-9,0 relative units.
2.3 Determination of the frequencies of chromosome aberrations (CA) and sister chromatid exchanges (SCE) in PBLs
Whole blood samples were processed for studies of CA and SCE. The cell culture methods were identical in both protocols: samples of 0.8 ml heparinized blood were cultured in duplicate at 37°C, in 5% CO2 atmosphere, in 10 ml RPMI-1640 (Sigma-Aldrich) supplemented with 20% fetal calf serum serum (Gibco Invitrogen Corporation) and 0.5 % PHA (Gibco Invitrogen Corporation), without antibiotics. For CA and SCE analyses, the cultures were incubated for 50 hr and 72 hr, respectively. 5-Bromo-2,-deoxyuridine (BrdU, Sigma-Aldrich) used in SCE analysis to identify the first and subsequent metaphases, was added at a concentration of 5 μg/ ml at 22 hr of culture. Culture harvest, slide preparation and staining were made following the standard methods using 5% Giemsa stain (Fluka) for CA [8], and according to the Fluorescent-Plus-Giemsa method of Perry and Wolff [9] for SCE. All microscopic analyses were blindly performed by permanent staff. CA characterization was carried out in 100 metaphases with 46 ± 1 chromosomes per subject according to Carrano and Natarajan [10]. Mitoses with 45 or 47 chromosomes were considered as aneuploid cells. Mitoses containing only achromatic lesions (gaps) and/or aneuploidy were not considered aberrant. Scoring of SCEs were performed from 25 metaphases of second divisions.
2.4 Determination of the frequencies of chromosome aberrations (CA) and sister chromatid exchanges (SCE) in PBLs
For the measurement of the percentage of apoptosis, PBLs were separated from the blood samples on Histopaque 1077 gradients (Sigma-Aldrich) and cultured in RPMI-1640 medium (Sigma- Aldrich) supplemented with 20% fetal calf serum (Gibco Invitrogen Corporation) and 0.5 % Phytohemagglutinin-P (PHA, Gibco Invitrogen Corporation) for 50 hours without antibiotics in a standard thermostat at 37°C in humidified atmosphere containing 5% CO2. One hour prior to the termination of the cultures, 5 μg/ml BrdU (Sigma-Aldrich) was added to the cultures. Cells were washed twice with PBS, and fixed in 1 ml of ice-cold 70% ethanol and stored at –20°C until further processing.
DNA denaturation prior to propidium iodide (PI, Sigma-Aldrich) and fluorescein isothiocyanate (FITC)-labeled monoclonal anti-BrdU (Becton-Dickinson) staining was performed at room temperature with 2M HCl containing 0.2 mg/ml pepsin (Sigma-Aldrich), according to the method of Piet van Erp [11]. DNA was stained with PI and the incorporated BrdU was detected immunocytochemically with FITC-labeled monoclonal antibody.
Flow cytometric analysis was performed on a FACS Calibur (Beckton- Dickinson) flow cytometer. Data for at least 10000 lymphocytes per sample were acquired; CellQuestPro Software was used for the analysis. The percentages of spontaneous apoptosis of PBLs were calculated with the CellQuestPro software.
3. Statistical Analysis
Statistical analysis was made using the GraphPad Prism 3.02 software (GraphPad Software, Inc.), differences between the studied groups and the control were tested using the Student’s t-test, p < 0.05 was considered as statistically significant.
4. Results
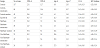
In our study we examined 128 personnel exposed to anesthetic gases, with more than 10 years in operating rooms in different medical units in Hungary. Majority of these workers were nurses in intensive care units (106) and 22 male surgeons. The control group consisted of 54 men and 83 women. Because of the small number of the male group, the cytogenetic data will be demonstrated together, without selecting gender. The working conditions were controlled each year and the safety level of nitrous oxide (NO) or Halothane were not exceeded, but in some cases the ventilation and the scavenging of these substences were not properly used. The average age of the controls and exposed was 37.0 years and 39.6 years respectively. The most important demographic data are included in Table 1.

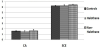
46.8% were smokersamong the exposed personnel, while only 36.2% of the controls were smokers.The study excluded those individuals who were heavy drinkers, but in the exposed group the regular, but moderate drinkers’ ratio was higher (64.8%) than in controls (44.4%). The cytogenetic, DNA-repair and apoptosis data of exposed groups divided into Halothane and Non-Halothane exposure and subdivided into smokers and non-smokers are summarized in Table 2. The average level of chromosomal abberations varied between 1.28 to 1.72%, measured 50h after culturing whole blood samples. The frequency of sister chromatid exchanges (SCE) was elevated in smokers compared to respective non-smokers in all groups, reaching significance in the Halothane exposed and control groups (Table 2). Apart from the significant difference in SCE between smokers and non-smokers, there were no significant differences in CA or SCE frequencies between the groups (Figure 1).
In our present study, the frequencies of low (<4 relative units) and high (>9 relative units) individual values of UDS, as alterations from the normal range values (between 4 and 9) were calculated.
These frequencies were calculated as percentages of all UDS values. Low values of UDS represent an exhaution of repair, and high values of UDS represent an induction of repair, respectively.
Frequencies of low UDS values were elevated in all subgroups of the exposed subjects, in comparison to controls (Figure 2). Frequencies of high levels of UDS were decreased in all subgroups of exposed, in comparison to controls. These decreased values were less frequent in the subgroups of Halothane exposed.

In the present study, similarly to UDS (see above), the frequencies of low (<3%) and high (>7%) individual values of spontaneous apoptosis, as alterations were calculated. These frequencies were calculated as percentages of all individual apoptosis values.
Frequencies of the percentages of low spontaneous apoptosis were elevated in all subgroups of the exposed subjects, with the exception of Halothane exposed nonsmokers, in comparison to the corresponding control groups (Figure 2 and Table 2). These elevated values were more frequent in the subgroups of non-Halothene exposed. Frequencies of high levels of apoptosis were decreased in all subgroups of the exposed, with the exception of Halothane exposed nonsmokers, in comparison to the corresponding control groups. These decreased values of the frequencies of higher levels of apoptosis were less frequent in the subgroups of Halothane exposed. In contrast, in case of the Halothane exposed nonsmokers even an increase in the higher frequencies of apoptosis was observed, in comparison to the corresponding control group.
5. Discussion
Several other studies have been designed to demonstrate toxicity of volatile anesthetics in experimental animals to demonstrate the adverse effects of these agents in carcinogenicity, mutagenicity and teratogenicity assays [12], as well as the analysis of human epidemiology [13,14]. Previously Chloroform,Trichloroethylene and Fluroxene was found to be mutagenic and carcinogenic in rodents [15], although these substances are not used anymore in everyday surgical practice. Currently used anesthetics (Isoflurane, Halothane, Enflurane, Methoxyflurane, nitrous oxide) were found not to be mutagenic or carcinogenic in animal models, or toxic to the operating room’s personnel if they were handled carefully [16,17].Indeed, our results reflect the same: in the examined working conditions, anesthetic gases were not mutagenic/clastogenic, based on cytogenetic data (CA, SCE). Maximum workplace concentrations of nitrous oxide (NO), Halothane, Enflurane and Isoflurane have been established by national agencies and it is varied between 25-to100 ppm. The safety level of theses halogenated agents is 2 ppm, which is generally accepted by many industrialized countries [18]. In our previous study [19]there was a statistically significant increase in the ratio of CD25+/ CD8+ cells - activated cytotoxic T cells - compared to the control. In workplaces where protective measures were strictly adhered to (with quality assurance) the activation of lymphocytes was at control level.However, where there was no quality assurance, activation of lymphocytes increased significantly compared to the control. In the anesthetic gas exposed smokers, there was a statistically significant shift in the T cell subpopulations: the percentage of helper T cells increased, while the percentage of cytotoxic T cell decreased, leading to an elevated Th/Tc ratio compared to the nonsmokers. During the 15 years following our study the exposed individuals developed malignant diseases in twelve cases (9,3%). Halothane exposed developed 3 breast cancers, which developed more than 10 years after our study, and within this group we found 3 more cancer cases, 1 colon, 1 skin, and 1 nasal cavity cancer. In the Non-Halothane group 6 malignant diseases developed (colon, urinary bladder, melanoma, skin and chronic lymphoid leukemia (CLL)). These tumors were not present at the time of genotoxicological investigations, except one colon tumor, and the CLL. In contrast, in our matched controls no malignancies were not found during this time.
6. Conclusions
Our present study found minimal cytogenetic damage, which may be related to the decreased apoptotic rate of peripheral blood lymphocytes due to the low risk of misrepair from a decreased DNArepair capacity. Further study is needed to explore the relationship between environmental anesthetic gas exposure and DNA damage in immuncompetent cells caused by oxidative stress of nitrous oxide( NO) and Halothane.In the group of anesthetic exposed personnel the found malignant diseases can’t be closely related to the exposure, because these types of tumors are the most common in the general female population in Hungary.
Conflicts of Interest
The authors declare that they have no competing interests.
Author Contributions
Anna Tompa was responsible for the conception and design of the studies, took part in the analysis and interpretation of the data, wrote most of the manuscript. Anna Biró took part in the analysis and interpretation of the data, wrote some parts of the manuscript. Mátyás G. Jakab took part in the analysis and interpretation of the data, wrote some parts of the manuscript.