


1. Introduction
The rise in life expectancy is a great success of recent years and presumably the percentage of older people will further increase in many European countries [1]. Forecasts published by the European Commission show a wide margin of people being dependent on help in the longer term as the risk of functional decline is expected to rise from 30% to 100% by the year 2050 [2]. Health promotion and measures to prevent or reduce functional decline in elderly people in Europe are provided through a long-standing public health policy goal [3]. This makes the identification of risk groups an important strategy to establish the basis for assessing the need of care and assistance, for example, in the domestic setting by district nurses.
In Austria, people’s need for nursing care has been assessed based on the seven levels of care allowance since 1993. Care need is a demand for care and assistance which must amount to at least 65 hours per month and “will presumably last for at least six months” [4]. In 2014, a total of 5.3% of approx. 8 million Austrians were in one of the seven care levels and received care allowances amounting to a total sum of approx. 2.5 billion euros [5]. In Austria, the assessment of the care level is part of the care allowance assessment and is primarily body- and functionality-related, resulting in the fact that limitations and resources for preventing functional decline in the domestic setting are not recorded sufficiently in this context. An individual need for consultation and/or intervention, with a view towards health promotion and prevention and with the aim of influencing functional decline, cannot be deduced here sufficiently. To enable an effective identification of risk groups, WHO recommends [6] a combined approach which focuses on recording the resources as well as the deficits. This gives an essential role to people’s subjective judgement and assessment of their own living situation since there is a correlation between functional decline and subjective quality of life [2]. One important component of quality of life for elderly people, in particular, is the ability to perform activities of daily living independently [7].
Functional decline describes the loss of independence in self-care activities (ADLs) or a deterioration thereof [8]. The consequences of functional decline are prolonged hospital stays, nursing home placement, hospital readmissions, and increasing mortality [9,10]. Thus, the question arises how to assess or even measure functional decline in order to be able to identify the appropriate preventive measures.
Besides the Katz ADL scale [11], the Functional Independence Measure (FIM) [12], and the Ranking Score, the Barthel Index (BI) [13] is considered an internationally standardized ADL assessment tool which has proven its worth over the past 50 years. The index, which has been translated into eight languages [14], is primarily used in acute care and in the rehabilitation of stroke patients [15] since suffering a stroke is the main reason elderly people lose their independence in the ADLs [16]. This is why primarily stroke patients, and in particular people from outside the clinical setting, were used for the verification of the quality criteria instead of elderly people with other health problems [15].
The great importance of the BI in nursing practice can be seen in its simple, fast, and feasible applicability [17] for evaluating a person’s ten activities of daily living (feeding, grooming, bathing, dressing, bowel and bladder care, toilet use, ambulation, transfers, and stair climbing). This satisfies the demand for the development and evaluation of models in home-based primary care which can improve the care of elderly people with risk factors in a time-efficient manner.
The BI expresses the degree of independence of a person by means of a total score (TC) [18]. The scale ranges from zero (0) to 100, whereby 0 means total dependence and 100 complete independence in the assessed dimensions. In the literature, different cut-off scores have been defined as indicators for interventions or for the identification of a risk [19,20]. The subject of this study was the BI according to the Hamburg Classification Manual. The Hamburg Classification Manual ensures the standardized use of the items in geriatrics in the German-speaking world. Pursuant to the manual [22], the following interpretation of BI cut-off scores is recommended: 95 to 100 points – completely independent; 85 to 90 points – partly in need of care; 35 to 80 points – in need of care; 0 to 30 points – totally dependent.
For a systematic evaluation of independent living and as a basis for planning target-oriented support, however, the WHO’s activity theory [22] indicates that the activity of a human being is embedded processlike in further health components of functionality (body functions and participation) as well as in contextual factors (environmental factors and personal factors). The degree of independence or functional decline is thereby described according to a biopsychosocial framework model. Due to the body- and performance-related assessment of independence or functional decline of a human being – as is the case in the assessment of the care allowance level in Austria – it is not possible to sufficiently identify risks to prevent functional decline that justify specific needs for health promotion and prevention for the group of elderly people living at home.
1.1 Objective
It was the aim of this study to show whether the BI according to the Hamburg Classification Manual is an adequate basic assessment tool to identify a risk group in elderly people aged 70+ living at home and to determine the correlating risk factors.
2. Material & Method
2.1 Study design
In this study, we conducted a secondary analysis of data collected in an explorative-quantitative cross-sectional study with the title “Preventive Senior Counselling in Tyrol”. The study was conducted on behalf of the Tyrolean state government by UMIT’s Department of Nursing Science in the period from 2011 to 2013.
2.1.1 Sampling and data collection
Recruitment of the study participants was based on a convenience sample of 344 people aged 70+ living at home in Tyrol. The subjects gave their consent to participate in the study themselves. Inclusion criteria were: age 70+, no cognitive impairments1, a written declaration of consent, and no legal care provider (in Austria: adult guardianship).
The nurses who collected the data during the project “Preventive Senior Counselling in Tyrol” were all registered nurses [23] with at least three years’ work experience in mobile care and nursing.
Prior to conducting this study, the study protocol was presented to the Research Committee for Scientific and Ethical Questions (RCSEQ) at UMIT – Private University for Health Sciences, Medical Informatics and Technology and was classified as ethically unobjectionable.
2.2 Measurements and variables
Our survey instrument was a computer-assisted multidimensional nursing assessment to subjectively assess functional health (see Table 1 and Table 2 ), based on a questionnaire that was used in the project “Senior Counselling in Tennengau/Salzburg” (Q-FHS) for 516 people aged 80+ [24]. This was further developed and subjected to content validity by a group of experts.

The nursing assessment consisted of three parts [18]. Based on the theoretical model of the WHO-ICF classification [22], part 1 of the nursing assessment focused on the activities which were measured with the BI [13] according to the Hamburg Classification Manual and the IADL Index [25]. Part 2 outlined the ICF components body functions with 22 health indicators and participation with five health indicators. Together with part, they represent the functionality of an individual. Part 3 examined the following factors: environmental factors, for example, the current utilization of home help and/or nursing care and the current care allowance level, as well as personal factors, such as age, sex, family status, and living arrangement.
2.3 Data analysis
In this analysis, the authors decided to summarize the four categories ranging from completely independent to totally dependent living according to the Hamburg Classification Manual in two categories. Thus, subjects “in need of care” (35 to 80 points) or “dependent on care” (0 to 30 points) were classified as “non-independent” and subjects who were “completely independent” (95 to100 points) or “partly in need of care” (85 to 90 points) were classified as “independent”. The authors combined subjects who were in need of care and those dependent on care into one group – non-independent – based on the assumption that living without external support is virtually impossible or very difficult for members of both these groups. However, people aged 70+ who are totally independent or partly in need of care are certainly able to live an independent life.
All statistical analyses were performed with SPSS 20.0 for Windows. The characteristics of the elderly people were analyzed with descriptive statistics (measures of location and dispersion: mean value, standard deviation, minimum / maximum). As a measure of association, we used odds ratios (OR) with 95% CI. We used the Mann-Whitney U Test or the t-test for two independent samples for the correlation calculation of interval-scaled data and the χ2 test for nominal-scaled data. A p-value of <.05 was considered statistically significant.
3. Results & Discussion
3.1 Sample characteristics
The majority of the 344 interviewees was female (n=240, 69.6%). The average age was 83.42 years (±4.99). The oldest person was 97 years old. Over half of the people were widowed (n=176, 51%) and 37% (n=127) were married. Under 10% were divorced or not married. 84.3% (n=290) of the sample had children. Slightly more than half of the subjects lived at home alone (n=174, 50.4%). Among the people not living alone, 37.6% (n=130) lived together with a relative and 10% (n=34) lived together with more than one relative. The remainder lived together with a non-relative or more than one non-relative.
Considering the high mean age of the study participants and the high proportion of people living alone, it is remarkable that 58.1% (n=203) were completely independent in the corresponding items of the BI (TS between 95 and 100 points). Only 18% (n=62) of the participants were found to be partly in need of care (TS between 85 and 90 points) and 19.8% (n=68) in need of care (TS between 35 and 80 points). A minority of participants (n=11, 3.2%) showed an extensive level of care dependency (TS between 0 and 30 points).
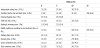
The individual items of the BI are illustrated in detail in Table 1. 34.6% (n=119) of the subjects stated that they had limitations in bathing and showering, 15.4% (n=53) had limitations in grooming, cleaning teeth, shaving or doing their hair (=personal hygiene). Further limitations were mentioned in activities such as climbing stairs (n=77, 22.3%) and in dressing and undressing (n=66, 19.3%). 20.3% (n=70) said that they could not entirely control their bladder (bedwetting or wetting themselves max. once a day), which is a typical phenomenon in this age group, and 9% (n=31) said that on average they were urine incontinent more than once a day.
3.2 Sample Characteristics of the non-independent and independent group
23% (n=79) of the people aged 70+ were classified as non-independent based on the BI results with a TS between 0 and 80 points. 77% (n=265) of the subjects were classified as independent based on a TS of 85 to 100 points.
The following descriptions are based on the details presented in Table 2:
On average, the non-independent participants were two years older than the independent subjects (M=84.95, ±5.74 vs. M=83, ±4.68; z=- 2.91; p=0.007), which was to be expected. This is also reflected in the fact that, in comparison to the independent group, significantly more non-independent people did not live alone (68.4% vs. 43.8%; p<.001). Non-independent persons were more likely to live not alone than subjects from the independent group (OR 2.8, 95% CI [1.63; 4.73]).
3.3 Functionality of the non-independent and independent group
In 21 out of 29 self-assessed health indicators, classified as body functions, activities, and participation by the WHO’s ICF classification (2005), significant correlations were calculated. It became evident that non-independent subjects had 1.4 times (95% CI [1.31; 1.53]) more limitations in instrumental activities of daily living than independent subjects. Furthermore, the health-related results demonstrated, in accordance with our expectations, that non-independent people are more likely to be affected by a disease (OR 4.7, 95% CI [1.83; 12.17]) and to and to suffer from this disease (OR 4.3, 95% CI [1.96; 9.50]). It is therefore understandable that dissatisfaction with the general health status is significantly higher among the non-independent than in the other group (OR 5.1, 95% CI [2.99; 8.71]). The same applies to pain (OR 2.5, 95% CI [1.43; 4.48]), falls in the last year (OR 2.9, 95% CI [1.69; 4.88]), insecurity when walking due to dizziness (OR 7.5, 95% CI [3.14; 17.86]), and difficulties in climbing stairs due to a lack of strength or breathing problems (OR 18.6, 95% CI [6.62; 52.34]).
This results in reduced social participation in terms of restricted mobility (driving the car oneself) (OR 10.3, 95% CI [2.46; 43.30]) and communication with others (phone) (OR 13.6, 95% CI [6.53; 28.38]) among the non-independent group.
3.4 Environmental factors of the non-independent and independent group
For all three environmental factors, significant results for both groups were calculated. Reflecting the effective structures of the Austrian healthcare system, the study showed that, in comparison to the independent group (37.4%), a higher percentage of the nonindependent group (78.5%) received care allowance (p<.001). The odds of being in one of the seven care levels was six times higher (95% CI [3.39; 11.05]) among the non-independent people than among the independent. Nevertheless, independent subjects were also allocated to five out of seven care levels.
A high percentage of the non-independent persons used both home help and/or nursing care (p<.001). Remarkably, the odds of using home help were 19 times higher (95% CI [4.52; 78.4]) for nonindependent than for independent subjects. With regard to the use of nursing care, the numbers were even higher: here, the odds were 35 times higher (95% CI [14.39; 83.03]) for the non-independent than for the independent group. The results also illustrated that a large percentage of the independent subjects (67.2%) used home help and more than one quarter used nursing care (26%).
4. Discussion
The BI is one of the most common clinical assessment tools to assess functional decline. The aim of this study was to focus attention on whether or not the BI, according to the Hamburg Classification Manual, is an adequate basic assessment tool to identify a risk group in people aged 70+ living at home whose capacity for independent living is at risk.
In the present study, independence or functional decline was categorized according to the Hamburg Classification Manual [21]. The state of being completely independent and the state of being “partly in need of care” were summarized in the independent group (BI TS 85–100 pts.). This is based on the authors’ assumption that even elderly people who are partly in need of care are able to compensate by using the existing resources in their familiar domestic setting and that it is widely possible for them to lead an independent life in their homes. The state of being “in need of care” and the state of being “dependent on care” were summarized in the non-independent group (BI TS 0–80 pts.). The results of the present study reinforce the subdivision into two groups. The non-independent subjects with a BI TS of 0–80 points could be identified as a risk group since 25 of 37 possible functional health indicators implied that functional decline was more likely to occur in this group than in the independent group (BI TS of 85–100 pts.)
Although the literature takes a critical view of the significance of the total score due to the ordinal scale [17,26], the use of the BI is recommended as a basic tool or as a global parameter in the daily routine of district nurses since it can be assumed that it can help describe changes in the health status of elderly people [27]. In their study with stroke patients, [28] could ascertain a BI ≤80 as an optimal cut-off score for self-reported dependency. However, Barthel & Mahoney [13] advised that an analysis of the individual items should be conducted additionally to allow for a pinpoint identification of the deficits. Thus, this study could demonstrate that the main problem areas in the activities of daily living in personal hygiene were within the field of locomotion and that, in accordance with the high average age of the sample (83 years), the results are comparable to the study by [29] in which the detected functional limitations in people aged 90+ were identified as risk factors for institutionalization. This suggests dependency in self-care competence since we know that functional decline increases with age, especially with high age, and requires respective levels of medical and nursing care.
The finding that the non-independent group was significantly older than the independent group makes sense; it is to be expected that these people will find it increasingly difficult to lead an independent life. This finding reflectsthe literature [30]. Hoogerduijn et al. [8] show in this context that people with a higher degree of limitations in the ADLs are more likely to develop limitations in the IADLs as well as in physical, psychological and emotional functions. Similar results were achieved by Freitas et al. [31] with regard to a correlation between limitations in the IADLs and an obviously high need for support and care in elderly people living at home. Our findings also reinforced this. For example, the odds of being in one of the seven care levels were sixtimes higher for the non-independent group than for independent group, the odds of using home help were 19times higher, and the odds of using nursing care were35times higher among the non-independent versus the independent group. This can also explain the findings related to lifestyle in this study. They clearly show that 68% (n=54) of the non-independent group did not live alone but were being cared for by their own family (in most cases by the daughter or daughter-in-law) [32]. The fact that relatives play a major role in home help and in the care of people aged 70+ became apparent in the present study since 100% of the non-independent subjects stated that they could rely on the support of relatives and friends in emergency situations. According toAustria’s Federal Institutefor Healthcare [33], relatives provide the major share of care and nursing of elderly people in Austria and, from an economic viewpoint, represent an immense potential for Austria. The enormous number of independent 70+-yearolds living alone (68%) underlines the demographic prognoses that in Austria the number of single households will increase [34]. The reasons for this development are, among other things, the ageing of the population and the related large increase of widowed or divorced people [35]. We can therefore assume that living alone will continue to be an ongoing trend among elderly people. The literature increasingly considers people living alone as a vulnerable group [36,37,38]. Contrary to the literature, a further secondary analysis of this study yielded that, despite their higher age, people aged 70+ living alone subjectively considered their functional health, in accordance with the biopsychosocial framework of the ICF classification, to be better than that of the 70+-year-olds not living alone.
This study also clearly showed that people aged 70+ living at home suffered from many impairments of body functions. In contrast to independentsubjects, especially the non-independent subjects were significantly more likely to suffer from diagnosed diseases, to feel impaired by diseases, to suffer a fall during the last year, to have gait instabilities, to have difficulties climbing stairs, and to need a walking aid. These limitations are consistent with the literature, which proves that independent living is jeopardized by a higher risk of falls [35].
Interesting are the results of this study with reference to care allowance eligibility. It became evident that approx. 22% of the nonindependent 70+-year-olds were in no care allowance level atall. Evaluations in this context confirmed that many elderly people living at home were not sufficiently informed about the intent and purpose of care allowance eligibility, on the one hand, and, on the other hand, were afraid that a possible functional decline implied potential dependence on third parties and a loss of autonomy [39]. In the German-speaking world, furthermore, it is evident that elderly people living alone of their own accord are reluctant to submit new applications for care allowance or request modifications thereto or that during visits to their doctor there is only limited time available to receive sufficient information on this matter [40]. Moreover, the problem is that in Austria there currently exists no valid tool to assess care allowance eligibility and elderly people thus are often not classified accordingly and in line with their individual needs of care and support [35].
For this study, we chose a quantitative cross-sectional design. Data were assessed once, whereby only a snapshot of the current situation of the interviewed 70+-year-olds was reflected. The external validity of the study results may be distorted by the fact that timerelated interfering factors were not included and may be limited due to a lack of temporal generalizability. For older participants, the willingness to participate in a cross-sectional study might be higher than the willingness to participate in a longitudinal study. From this, we derive that we can probably speak of a potential distortion as the group with good general health was possibly overrepresented in the sample. Thus, people with a poor general health status may have been underrepresented in this study. The chosen study design does not allow for causal conclusions. The estimates for some functional health indicators were not precise or show a high variance due to varying group sizes.
5. Conclusion
The findings of this study show that, by subdividing the sample into two groups (independent and non-independent), the BI can identify a risk group for which leading an independent life without support is hardly possible. Categorization with a valid (assessment) tool provides a solid basis for target-group-specific support planning in the field of home-based primary care in Austria under due consideration of biopsychosocial conditions.
Competing Interests
The authors declare that they have no competing interests.
Author Contributions
All authors contributed equally to writing the proposal, data collection, data analysis, writing the manuscript, and figures.
Acknowledgments
We owe a great debt of gratitude to the Department for Social Affairs of the Tyrolean state government for commissioning us to conduct this study. Many thanks are also due to the 13 registered nurses for performing the “preventive home visits”. Sincere thanks also go to Dipl.-Stat. Raffaella Matteucci-Gothe, UMIT, for her statistical advice.