


1. Introduction
Depression is one of the many diagnostic categories that are believed to be influenced by sociocultural components [1]. It was also acknowledged that culture may influence the incidence and prevalence of depression as well as the patterning of symptoms and a patient’s recognition of it as illness [2]. According to the National Institute of Mental Health (NIMH)[3], studies using measures of depression as indicators of the impact of sociocultural adjustment and other environmental processes on mental health are popular. There have been quite a number of studies examining depression in Latinos and Mexican Americans in particular, which generally addresses the extent to which ethnicity increases or reduces risk for depression.
Most of the empirical research on mental health of Korean Americans has been conducted since 1976 [4]. Korean Americans have levels of stress, depressive symptoms, and other mental health problems, that are higher than white Americans [5-7]. Studies have generally found that stressful experiences, such as family violence, alcoholism, juvenile delinquency, alienation of the elderly, marital and intergenerational conflicts contribute significantly to the mental health problems of Korean immigrants [8-10].
Acculturation, a major component of “migration-induced adaptation [11]” is indicated as a cultural change process that occurs when two or more cultures interact as individuals attempt to adapt to their new milieu [12]. A general view formerly held was that the experience of acculturation inevitably brings about a decline in the mental health status of individual [13]. However, such a broad general relationship is now no longer supported due to the variation in forms of acculturative experiences. Berry and Kim listed the variables such as phase and modes of acculturation, type of acculturating group, nature of larger society, sociocultural characteristics of acculturation group, and psychological characteristics of acculturating individual, that may affect the relationship between acculturation and mental health [13, p. 219].
Although the studies that have examined acculturation and depression have reported somewhat equivocal results; either lessening or increasing the intensity of depression [14], research has generally recognized the adaptation process can be potentially stressful and the process of acculturation may increase risk of psychological disorder [15, 16]. When individuals are exposed to a new environment, a critical process of cultural learning and behavioral adaptation takes place [15, 17-19]. Therefore, empirical research has shown a significant impact of acculturative stress on the mental health of international migrants [20, 21].
One of the issues related to the mental health of ethnic minorities pertains to the study of psychological and behavioral research on acculturation among immigrant groups in U.S., which has tended to revolve around two concepts: ethnic attachment (ethnic identification) and acculturation. Ethnic attachment refers to an individual’s identification with and maintenance of the original ethnic identity [22,23]. On the other hand, acculturation refers to the acquisition of cultural traits of the host society [12].
Many researchers tried to investigate whether the experiences of stressful life events among immigrants' would be improved with these two concepts. Researchers found that components of ethnic identification may help to prevent numerous psychological dysfunctions related to identity confusion [24, 25]. Also, ethnic social support (unique adjustment) has been reported as a buffer against the negative impact of stressful situation [26]. Zuniga (1988) mentioned that the process and components of ethnic identification are valuable since an integrated ethnic identity is believed to precede bicultural competence [27].
Although there are contradictory findings by different researchers, in general studies reported that those who are the least acculturated experience the greatest stress [28]. They are also most likely to be the first-generation group. The most acculturated individuals tend to be those who experience the least stress and are more likely to be third/ later generation students who were born in U.S. With respect to length of residence, anxiety tends to decline as length of residence increases: "As the difficulties are ironed out, as the economic conditions improve, the anxiety diminishes down to the level of the surrounding population" [29, p. 54]. The primary goal of the current inquiry is to test the hypothesis that while controlling for length of residency immigrants with greater acculturation to the U.S. will report fewer depressive symptoms.
2. Theoretical Background
In order to effectively adapt to the host society, immigrants either retain their parent culture or adopt the host culture or demonstrate characteristics of both cultures. Historically, the adaptation process was viewed as a unidirectional process, based on the premise of a theory of replacement which contends that as time passes, immigrants gradually replace their parent way of sociocultural life with that of host cultures [30,31]. When acculturation is considered as the immersion of the immigrant culture in the new culture, there is an assumption that mainstream culture and the culture of origin are mutually exclusive [11]. However, much of the traditional work in acculturation has been criticized for its simplicity, and displayed in a unidimensional perspective [32,33].
Current models, however, stress the selective and multidimensional nature of the immigrant process [32, 34]. Specifically, immigrants do not simply shed their old or parent values for new ones, but rather select, shift, and modify to adapt to the new environment. There is no one uniform, static, traditional culture that is carried by immigrants from their ethnic country. In fact, there are various forms that are constantly modified and reshaped by a host of factors, including the demands and pressures of the immigrant experience. Such models assert the interactive nature of both cultures, instead of emphasizing the loss of one to the other.
Researchers found groups and individuals may acculturate in various ways; all results in cultural and psychological changes following culture contact, but the extent and nature in cultural and psychological changes vary greatly. For instance, Mendoza and Martinez [34] identified four typological patterns of cultural adjustment: 1) cultural resistance; 2) cultural shift; 3) cultural incorporation; and 4) cultural transmutation. Similarly, Berry and Kim [35] also identified four distinct varieties of acculturation: integration, assimilation, separation, and marginalization. They assumed mental health status of individuals may vary across these four modes, both as a function of the mode itself, and as a function of the congruence between an individual’s preferred mode and that of the majority of his or her group [35].
In particular, it was expected that the integration mode (i.e., bicultural), where selective involvement in two cultural systems, may provide the most supportive sociocultural base for the mental health of the individual, while the poorest mental health outcomes were speculated to result from marginalization, followed by separation and assimilation mode [35].
In an other study, Kim studied a group of Korean immigrants to Toronto, using a 20-item mental health questionnaire devised by Cawte [36], and scales developed to assess ethnic identity and the attitudes held toward the four modes of acculturation [37]: pluralism, assimilation, separation and marginalization. A series of multiple stepwise regression analyses were employed in a sample of 150 respondents, who varied by age, sex, and length of residence. The general picture emerged that high stress was present among those who reported using both the Korean and the English languages less, who were not Christian, and who had high scores on the marginalization mode of acculturation. These variables suggest that those who are isolated or marginal from both the heritage and host communities are more likely to experience acculturative stress.
The study by Padilla also recognized the bicultural mode [19]. This research, along with a few other studies, clearly demonstrates selective bicultural patterns among immigrants. It is consistent with another recent investigation of Brewer’s (1991) view of the social self, with two opposing needs: need for assimilation and need for differentiation [38]. It was found that bicultural individuals suffer less distress, although biculturalism threatens the stability of one’s social network and exposes the individual to cross-pressures [16]. Researches found that people in a situation of marginalization showed poorest mental health while an individual who is in integrated (bicultural) mode suffered least distress.
The purpose of the study was to investigate the association between acculturation and ethnic attachment factors (using multidimensional measures proposed) with depressive symptoms among Korean immigrants has examined. Multidimensional measures of acculturation and ethnic attachment as well as overall summary measures will be statistically examined for their association with depressive symptoms. Specifically, the relationship will be addressed by testing five hypotheses:
Hypothesis 1: All acculturation constructs will be negatively associated with depressive symptoms, such that the higher the degree of acculturation (i.e., greater identification with mainstream culture) becomes the lower the degree of total CES-D scores.
Hypothesis 2: All ethnic attachment components will be negatively associated with depressive symptoms, moreover the higher the degree of their ethnic attachment, the lower total CES-D scores will be.
Hypothesis 3: Acculturation is not accompanied by a weakening of ethnic attachment; they are independent of each other. Therefore, the effect of either one variable will not depend on the value of the other variable.
Hypothesis 4: (If we conceptualize the ideal type of integration mode as bicultural and bisocial adaptations), bicultural adaptation strategy will be associated with the lowest CES-D scores, while marginalized mode is associated with the highest CES-D scores.
Hypothesis 5: Compared to overall acculturation/ethnic attachment measures, those measured by multidimensional approaches will better predict depressive symptoms.
3. Methods
3.1 Data Collection
The data set was obtained from the Chicago sample conducted by Hurh and Kim [10, 11]. The study was a cross-sectional epidemiological survey (diagnostic interviews for assessing the degree of psychosocial adjustment) of Korean immigrants. Data were obtained through interviewing a random sample of 622 firstgeneration Korean immigrants (age 20 and older) residing in the Chicago area. Twenty-five interviewers trained by the investigators in intensive training sessions conducted the interviews. A two step procedure was used for sampling. Data collection was described in detail by the original investigator [11].
3.2 Major Variables
Demographic and control variables: To provide demographic information for the study, the questions used were those on sex, marital status, education and age. No measure for income was available. Two possible proxy measures for income were home ownership and job status. However, wide variability in household income levels can be expected in each category of the job status. Likewise, income could not be well approximated by the dichotomous home ownership item. Therefore, income could not be included as a control variable in this study. Researchers have found that length of residence is a proxy or pervasive indicator of immigrants’ acculturation, social assimilation, and economic improvement [39]. As length of residence extends, the immigrants’ acculturation progresses, and economic condition improves. Hence, length of residence in the U.S., a possible confounder, was used as a major control variable throughout the analysis. Table 3.1 in the result section presents the mean score of overall depressive symptoms (by the CES-D scale) for demographic variables and length of stay in U.S.
In addition, major sets of variables for acculturation and ethnic attachment (as a measure of social/cultural adaptation) were included in the analyses. The author yielded summary measures for various dimensions of acculturation and ethnic attachment. Acculturation is multidimensionally measured by a set of 14 variables representing 4 constructs, while ethnic attachment is measured by a set of 15 variables having 6 constructs. In summary, predictors that were incorporated into the analyses include sex, marital status (married vs. single or other), education (4 categories), age, the years of residency in U.S., and ten constructs measuring acculturation and ethnic attachment. More descriptions for measuring instruments for the major predictors (acculturation and ethnic attachment measures) and the dependent variable follow below.
Independent variables: Acculturation was measured by the 14 Likert-type items consisting of 6 items concerned with English language familiarity, 3 items on social interaction with Americans, 3 items on individualistic values, and 2 items about adoption of American appearances. Ethnic attachment was measured by 15 total items: 4 items on proximity to Koreans, 2 items on interaction with Korean relatives, 2 items on attitude towards Korean heritage, 3 items on interaction with Korean friends, 2 items on exposure to Korean print media and 2 items on Korean community ties. Several factors showed inadequate reliability as measured by Cronbach’s alpha. Nonetheless, these predictors were conceptually thought to represent dimensions of acculturation and ethnic attachment, thus all predictors were utilized in the analyses for exploring the effect of acculturation and ethnic attachment factors and their impact on the level of depressive symptoms.
Each construct used as a predictor is an average of standardized items, which were conceptually related and were identified through factor analysis. For example, the factor score for English language familiarity was the average of standardized items regarding fluency of reading, writing, and speaking English (1 to 5 scales); and frequency of reading English newspapers and magazines (1 to 3 scales). Because the scales were different, the variables were standardized individually before taking the average.
In addition, an overall measure for acculturation was computed from all acculturation variables (: a total score computed by summing scores of the individual items); similarly an overall measure for ethnic attachment was computed from all ethnic attachment items. Cronbach’s alpha for these measures was .75 (n=570) and .53 (N=602), respectively.
Dependent variable: The present study is based on subjective report of depressive symptoms as a dependent variable, specifically measured by the Center for Epidemiological Studies Depression (CES-D) Scale, a 20 item self-report measure of the frequency of occurrence of depressive symptoms. Respondents were asked to check an answer on a scale from 0 (rarely or none of the time) to 3 (most or all of the time) to indicate how often they had felt the way each item described during the past week. CES-D scores need to be interpreted as an index of respondents’ subjective mental health. In scoring the CES-D scale, a total value is obtained by summing the answers for all 20 items. Therefore, its scores range from 0 to 60 points, with higher scores indicating more depressive symptoms. The continuous CES-D scores were used instead of “cut-points.”
Previous researchers have noted that Korean populations tend to show unexpectedly low levels of positive affect [40]. For this reason, sometimes the four positively worded items on the CES-D battery are excluded when measuring depression in Koreans [41]. In our data, however, the 16-item and 20-item standardized CES-D means were virtually indistinguishable. Furthermore, Cronbach’s alpha was 0.86 with all 20 items and 0.88 with only 16 items; a negligible difference. Therefore, all 20 items from CES-D were used. Radloff (1977) reported internal reliability coefficients ranging from .84 to .90 for the 20-item scale [42]. The alphas of this scale were .86 for the Chicago sample (n=591).
3.3 Statistical Analysis
Individual acculturation and ethnic attachment measures were initially examined for association with depressive symptoms (CES-D) using bivariate Pearson correlations. Further analysis involved the computation of OLS regression estimates of the effects of several predictors on depressive symptoms (CES-D). The associations between change in CES-D scores and sets of variables representing acculturation and ethnic attachment were examined using linear regression models.
Overall summaries were also considered as alternatives to sets of distinct constructs in a separate regression analysis. Comparing the adjusted R-squares between the overall and multi-dimensional approaches will show the possible benefits of considering acculturation and ethnic attachment to be multi-dimensional. Also, dividing respondents into tertiles for each acculturation and ethnic attachment created the bicultural scale.
The final model for sociocultural adaptation and depressive symptoms among Korean immigrants included sex, age, education, marital status, length of residency in U.S., 4 constructs measuring acculturation and 6 constructs measuring ethnic attachment. SPSS version 8.0 for Windows was utilized throughout [43].
4. Results
4.1 Demographics
Slightly more men than women participated in the study and most of the respondents were married (84.7%). The age range of respondents was from 20 to 82 years old with mean age of 41.6. The most common education level was a bachelor’s degree (37.7%). All5 participants were first-generation Korean immigrants, who had lived in the United States for an average length of residency of 8.4 years, with a range from 3 to 29 years. For more detailed description of the Chicago study, refer to Hurh and Kim (1988) [20].
5 This also includes “1.5” generation, those who were born in Korea or another country and immigrated to the U.S. before age 20 (8.4 %), due to their parents’ immigration.
As seen in Table 1, females scored higher than males in the mean overall score of depressive symptoms measured by the CES-D scale, although the difference was not statistically significant. The mean CES-D score for the 591 CES-D completers was 12.6 (12.3 for males and 12.9 for females), which was 3-5 points higher than White Americans and other Asian-Americans [6,42]. The married group showed the least depressive symptoms, and those who were never married showed the most. No notable trend was found for education. As expected, age appeared to be negatively related to depressive symptoms. It was found that the younger the respondent, the higher the mean CES-D score. Additionally, a longer length of U.S. residency indicated substantially lower CES-D scores.

residency for first generation Korean immigrants in Chicago.
4.2 Bivariate Correlations
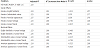
The relationships of continuous predictors to self-reported depressive symptoms are first examined by Pearson correlation. Table 2 presents the Pearson correlations for variables of interest with CES-D score, based on combined (all respondents), male only, and female only models. In the preliminary bivariate correlations, women and men showed roughly equivalent associations between all continuous predictors and CES-D score. All effects were in the same direction for significant predictors in the three models. This lack of interaction between predictors and gender was further illustrated in the regression analyses, which follow. Since respondents of both genders show no significant differences, further analyses were not stratified by gender. Therefore, the results will focus on correlations for the combined sample.

Significant Pearson correlations were observed between depressive symptoms and all acculturation dimensions. Two acculturation measures, English language familiarity and social contacts with Americans showed a negative correlation with depressive symptoms. However, individualistic values and adoption of American appearances were positively related with depressive symptoms. English fluency showed a stronger correlation (r = -0.163, p < 0.001) while social contact with Americans showed a weaker correlation (r = -0.095, p < 0.05). On the other hand, negligible and non-significant correlations were observed between depressive symptoms and all ethnic attachment dimensions except for interaction with Korean friend. As expected, this construct showed a negative correlation (r= -.139, p < 0.001) with depressive symptoms. The more interactions with Korean friends, the lower the CES-D score, indicating fewer depressive symptoms.
The control variable, length of residency in the U.S. showed an expected negative correlation with depressive symptoms (p < 0.001). The longer the U.S. residency, the lower the CES-D scores. In addition, non-significant Pearson correlations were observed between depressive symptoms and overall acculturation and ethnic attachment scales. A multidimensional approach, by considering the factors as separate predictors, appears to give a clearer picture than averaging over all dimensions.
4.3 Multiple Regressions
Table 3 presents the results of the multiple regression analysis predicting depressive symptoms on the predictors. The association between acculturation and ethnic attachment constructs with the depressive symptoms did not differ by gender. Initially, models were tried for men and women separately and also for the sample as a whole. Interaction terms between gender and each of the significant acculturation and ethnic attachment constructs were tested individually in the full model, but none was statistically significant. Therefore, none of the analyses was stratified by gender. All results below are reported based on the findings from the total sample.

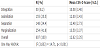
The systematic investigation of the correlates with the respondents’ depressive symptoms began with regressing CES-D scores on demographic variables and length of residency in U.S. (Model 1 in Table 3). This includes the regression coefficients to determine the significant demographic variables. Marital status (single, other, married) was a significant predictor of depressive symptoms among Korean immigrants. Regardless of gender, the single and other categories showed positive regression coefficients, indicating increased CES-D scores. Specifically, both single and other respondents had CES-D scores, which were about 5 points higher, on the average, than scores from married respondents. Also, length of residency showed a significant and negative association with depressive symptoms, indicating decreasing levels of depressive symptoms over time, after immigration. Four years of additional time spent in the U.S. was associated with a one-point decrease in CES-D scores. Regardless of the statistical significance of the predictors in Model 1, all demographics and length of residency were controlled for in all subsequent models.
Model 2 in Table 3, included all four acculturation constructs, three of which were significantly related to depressive symptoms. Marital status remained a significant predictor, but length of residency in U.S. was no longer significant. Among the three significant acculturation predictors, English language familiarity was negatively associated with CES-D scores. On the other hand, individualistic values and adoption of American appearances were associated with higher CES-D scores. Regarding regression coefficients, English language familiarity was more strongly associated. Specifically, linguistic acculturation was associated with an additional 0.7 points high in regression coeffcients on the average, compared to two other significant acculturation constructs.
Model 3 in Table 3 included all six ethnic attachment dimensions, only one of which was significantly related to CES-D scores. For the ethnic attachment variables in the Chicago sample, there appeared, at the bivariate level, to be two significant predictors of depressive symptoms: proximity to Koreans (beta=1.369, p < .05), and the Korean friend score (beta=-1.606, p < .01). However, when we controlled for the length of residency in the U.S., the proximity score became insignificant. Because Korean proximity and length of residency in U.S. are correlated (r=-0.292, p < .01), Korean proximity tells us something about the length of residency. Because length of residency was such a significant predictor of depressive symptoms in this model, Korean proximity may have been significant simply due to its correlation with length of residency. The final conclusion would be that only the Korean friend score provides some information about depressive symptoms among Korean immigrants, given the length of residency is known. It showed a significant and negative association with depressive symptoms, lowering 1.5 points in CES-D scores with a unit increase in interaction with Korean friends.
Finally, the full model is presented in Model 4. This regression model including the demographic variables, length of stay in U.S., acculturation measures and ethnic attachment measures had an adjusted R2 of .123. All significant predictors from the previous models were shown to be also significant predictors in the final model. Marital status, education, three acculturation measures and two ethnic attachment measures were significantly associated with depressive symptoms. Consistently, marital status was a significant predictor for depressive symptoms in all models.
Education was positively associated; respondents with some college, a college degree, or some graduate school were about two points higher on CES-D scores compared to the reference group (high school or less). However, only the “some college” category was significant at the p value of .05. There is a possible explanation for this finding. It has been reported that Koreans have the highest proportion of advanced degrees (36 %) of any ethnic group in the U.S., including Japanese-, Chinese-, and Anglo-Americans [44]. However, they are often unable to find jobs appropriate to their skill level and generally operate small businesses catering to various ethnic groups [45]. This might be a contributing factor in the higher CES-D scores found among educated Koreans.
Three acculturation measures were significant predictors of depressive symptoms at p < 01. The significance of these predictors suggests some underlying construct exists which relates to depressive symptoms. Two ethnic attachment measures: attitude towards Korean heritage and interaction with Korean friends, were also significant predictors and negatively associated with CES-D scores. These two ethnic attachment constructs were beneficial for the immigrants’ depressive symptoms. Same as in Model 2, length of residency was not a significant predictor of depressive symptoms in full model, although it was a significant predictor of depressive symptoms in Models 1 and 3 (where the acculturation measures are not included). It could be that length of residency predicts CES-D only because it is linked with acculturation measures.
In addition, the full model was tested without controlling for length of residency in U.S. Importantly, three significant acculturation measures came out significant, regardless of controlling for length of residency. Also, the estimated effects of the significant acculturation constructs were almost identical, regardless of the presence of length of residency in the model. Therefore, one might conclude that these acculturation effects are consistent, even when comparing individuals with differing lengths of stay in the U.S.
Models 2 and 4, which included the acculturation measures, showed the highest adjusted R-squares: 0.113 and 0.123, respectively. For Korean immigrants in the present study, acculturation measures are more important predictors of depressive symptoms than ethnic attachment measures. In addition, acculturation and ethnic attachment are independently associated with depressive symptoms, since effects of acculturation were similar in models 2 and 4 (regardless of presence of ethnic attachment measures).
Additional analyses include regressing CES-D scores on overall summaries of acculturation and ethnic attachment measures, instead of sets of distinct constructs. When overall measures of acculturation and ethnic attachment were considered, these were no longer significant predictors. Also, adjusted R2 using the overall approaches were smaller than the multi-dimensional approaches (see Table 3). It decreased the variance explained in CES-D score in the full model by half. These indicate the possible benefits of considering acculturation and ethnic attachment measures as multi-dimensional.
There were no acculturation or ethnic attachment measures that showed significantly different effects for men and women. Model 4 in Table 3 was the baseline model against which all other interaction models are evaluated. The five significant acculturation or ethnic attachment predictors were included in interaction terms with gender, to test whether their effects differ between men and women (refer Table 4). Each of the five terms was added into the full model individually, but the addition of interactions did not increase the variance explained over the baseline model, and none was statistically significant.
Another question of interest was whether or not acculturation and ethnic attachment are independently associated, or whether they interact to predict depressive symptoms. Accordingly, six interactions between each of three significant acculturation measures and the two significant ethnic attachment variables were tested individually by inclusion in the full model. No interactions were significant. Also, the results showed no increases in the explained variance in CES-D scores. Therefore, it is concluded that acculturation and ethnic attachment are independently associated with depressive symptoms among Korean immigrant respondents in this study.
The graph (Figure 1) was created to illustrate how acculturation and ethnic attachment relate to predicted CES-D scores, using the overall acculturation and ethnic attachment measures. As seen in Figure 1, there was little difference between low and medium for either acculturation or ethnic attachment. The lines in the graph are roughly parallel, indicating that acculturation and ethnic attachment are independently associated with CES-D. This is consistent with the previously noted non-significant interactions in the regression analyses.
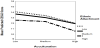
To further clarify these differences statistically, an ANOVA and post-hoc tests were conducted. The results indicated that some of the nine groups, e.g., low ethnic attachment along with low acculturation was very similar to low ethnic attachment with medium acculturation (p=0.981), indeed showed no significant differences in CES-D scores. It was always appropriate to combine medium and low for either acculturation or ethnic attachment; therefore these were merged to create the four modes of acculturation discussed by Berry and Kim (1986). In this manner, four distinct varieties of acculturation were created; 1) Biculturalism6 (high on both acculturation and ethnic attachment), 2) Assimilation (either low or medium ethnic attachment with high acculturation), 3) Separation (either low or medium acculturation with high ethnic attachment), and 4) Marginalization (either low or medium acculturation with either low or medium ethnic attachment) Figure 2.

6Berry and Kim (1988) used the term “Integration.” This paper conceptualize the ideal type of “integration” mode as bicultural and bisocial adaptation, and therefore uses “biculturalism” instead.
Level of depressive symptoms varied across these four modes. Being highly acculturated and ethnically attached is associated with fewer depressive symptoms; “Bicultural (integration)” mode of adaptation had the lowest predicted CES-D score (see Table 7). An ANOVA revealed that the bicultural mode (M=10.6) scored significantly lower than assimilation (M=12.0, p < 0.05), separation (M=12.5, p < 0.05), and marginalization (M=13.5, p < 0.001). While “biculturalism” scored significantly lower than all three other modes, “marginalization” scored significantly higher than all three other modes (p<0.05 in all cases). However, an ANOVA revealed that modes of assimilation and separation had similar means on the CES-D score (p=0.57). This pattern of differences (except between separation and assimilation) is consistent with the pattern found by Berry and Kim [35].
5. Tests of Hypotheses
In light of the consistently reported association between high acculturation and depressive symptoms, the author hypothesized that highly acculturated respondents in all acculturation constructs would be more likely to associate with decrease in CES-D scores. This hypothesis was supported in part by the data. Correlation analysis between two acculturation constructs: 1) English familiarity and 2) social contact with Americans with CES-D scores, revealed the significant negative correlation, indicating the higher these acculturation scores the lower the CES-D scores (see Table 2, combined column). However, this hypothesis was supported by regression analysis only for linguistic acculturation measure, but not for social contact with Americans. The measure of linguistic acculturation indicated the negative regression coefficients after adjusting for demographic variables, length of residency and ethnic attachment constructs. Therefore, Korean immigrants who acquire traits of the dominant culture through fluency and regular use of the English language reported fewer depressive symptoms.
On the other hand, the opposite was found to be true for two other dimensions of acculturation constructs: adoption of American appearances and individualistic values. These presented significant positive correlations with CES-D, as well as the significant positive regression coefficients in predicting depressive symptoms. The data indicated that respondents who are more acculturated in these dimensions of acculturation are more likely to experience depressive symptoms.
The second hypothesis predicted that the respondents with a higher degree of ethnic attachment would be more likely to experience fewer depressive symptoms. The analysis showed congruent results for this hypothesis. Both the significant ethnic attachment constructs were negatively associated with CES-D scores according to regression analysis and correlational analysis (Tables 2 and 3). Regression analyses indicated that respondents who had strong attitudes towards Korean heritage and more interactions with Korean friends were associated with decreased level of depressive symptoms.
The third hypothesis was also supported; the interactions between acculturation and ethnic attachment variables were not statistically significant (Table 4). The acculturation-ethnic attachment relationships with depression were independent; neither was influenced by the other. If acculturation and ethnic attachment as the opposite ends of the scale (based on unidimensional model), a stronger negative correlation would be expected. However, the correlation coefficient between overall acculturation measure and overall ethnic attachment measure was –0.323. This coefficient is not large enough to support the unidimensional model. There was much more variability than this simpler model would explain.
Fourth, it was hypothesized that bicultural adaptation mode would be associated with the lowest CES-D scores. As found in table 5, predicted CES-D scores of biculturalism mode was 10.6, which was significantly lower than assimilation (12.0), separation (12.5) and maginalization (13.5) modes.
Finally, it was posited that compared to overall acculturation/ethnic attachment measures, a multidimensional measurement approach would be better at predicting depressive symptoms. This hypothesis was also supported. A greater statistical significance using individual constructs compare to the overall measures (Table 3) was found. Also, the adjusted R2 was greater when individual constructs were included in the model.
6. Discussion
This study examined the multidimensional measures of acculturation and ethnic attachment and their effects on depressive symptoms among Korean immigrants. As initially hypothesized, ethnic attachment dimensions were associated with decreased reports of depressive symptoms. Thus, the results indicated that respondents who are more ethnically attached to Korean heritage (-0.82, p < .05) and Korean friends (-1.26, p < .05), expressed a lower level of depressive symptoms.
On the other hand, opposite associations were found among some acculturation constructs. Although language acculturation was associated with decreased reports of depressive symptoms (-2.25, p < .01), the opposite was true for individualistic values and adoption of American appearances. Contrary to the original hypothesis, these two dimensions of acculturation were associated with increased reports of CES-D scores (1.43, p < .01 and 1.48, p < .01, respectively). (These findings are independent from length of residency.)
Development of individualistic values may be confused with egoism by first generation immigrants, whose Korean cultural background emphasizes the importance of interpersonal harmony and concern for others beyond concern for oneself. The adoption of American first names or attendance at an American church may introduce separation or distance from others who emphasize their Korean identity by maintaining their Korean first names and Korean church membership. Acculturation along either of these dimensions may increase tension in relationships with other Koreans, or produce feelings of guilt. Therefore, some aspects of acculturation may contribute to a higher level of depressive symptoms, while linguistic acculturation is associated with fewer depressive symptoms.
The results support the findings from Mendoza (1984), who proposed that acculturation is multidimensional process and “therefore not a construct that can be effectively analyzed by a single measurement or necessarily generalized from a cluster of correlated variables” [46, p.64]. Not overall measures but a multidimensional measure of acculturation and ethnic attachment was found to be predictive when assessing the depressive symptoms of Korean immigrants.
It was also hypothesized that a bicultural identification would be associated with a decreased level of depressive symptoms, possibly because of increased ethnic social support and enhanced adaptive limitations by acquisition of cultural traits of the host society [26,47]. The data were consistent with these hypotheses. When acculturation was measured from a multidimensional view that assessed simultaneous involvement in both cultures, bicultural respondents were least depressed than other respondents followed by assimilated, separated, and marginalized respondents. There were no interactions between acculturation and ethnic attachment; however bicultural individuals have the lowest CES-D scores in this study population.
Some researchers have found that acculturation scores are good predictors of ethnic self-identification [48-50]. A person who believes that ethnic attachment and acculturation are two sides of the same spectrum (the one-dimensional model) would expect that only one or the other would be significant. However, the present study explored the confluence of ethnic attachment and acculturation on mental health. The important finding is that some aspects of ethnic attachment and acculturation are significant even when they are in the model together. This means that we need to know about both ethnic attachment, and acculturation, in order to predict depressive symptoms of Korean Americans. In this respect, immigrants’ depressive symptoms are subjected to the interplay between acculturation and ethnic attachment [51].
Some researchers have found that acculturation scores are good predictors of ethnic self-identification [48-50]. A person who believes that ethnic attachment and acculturation are two sides of the same spectrum (the one-dimensional model) would expect that only one or the other would be significant. However, the present study explored the confluence of ethnic attachment and acculturation on mental health. The important finding is that some aspects of ethnic attachment and acculturation are significant even when they are in the model together. This means that we need to know about both ethnic attachment, and acculturation, in order to predict depressive symptoms of Korean Americans. In this respect, immigrants’ depressive symptoms are subjected to the interplay between acculturation and ethnic attachment [51].
In summary, the results of this study indicated that acculturation/ ethnic attachment measures composed of several correlated dimensions were predictive of depressive symptoms. In detail, linguistic acculturation along with acculturation measured by individualistic values and adoption of American appearances were predictive of depressive symptoms. Also, ethnic attachment measures by attitude towards Korean heritage and interaction with Korean friends were predictive.
Given the relatively few large-scale systematic studies of the Korean immigrant population, future studies, both those conducted on college campuses and within the larger community, must make a concerted effort to examine not only more dimensions of acculturation, but also acculturative stress, which is defined as a conflict in values, beliefs, assumptions, and behaviors that may lead to tensions between two or more cultures [52]. Future research should also include more heterogeneous samples of Korean Americans and be conducted in various geographic locations to control for community support factors and influences.
To our knowledge, no previous studies have explored the relationship between multidimensional measures of acculturation and ethnic attachment and their effects on depressive symptoms among Korean immigrants. Through this study, the author attempted to establish an empirical link between two measures and depressive symptoms. These findings will help our understanding of the mental health implications of international migration. It will also help to design intervention of mental and behavioral disorders among Korean immigrant population in particular and Asian immigrants in U.S. in general. When providing the services or designing interventions to Korean immigrants, the level of acculturation and ethnic attachment cannot be overlooked. This suggests that culturally sensitive strategies for this population may need to reflect issues of cultural learning and the behavioral adaptation that takes place as individuals are exposed to a new culture.
Competing Interests
The author declare that there is no competing interests regarding the publication of this article.
Acknowledgments
I would like to sincerely thank to original investigator Hurh and Kim for conducting a cross-sectional epidemiological survey (diagnostic interviews) and collecting the data. I also thank to all Korean immigrants who took part in this survey.