


1. Introduction
Amid a situation with a rapidly aging population, it is an urgent issue to maintain the quality of life (QOL) for older persons. Physical activity, especially walking, is an important QOL factor which is essential for humans to lead healthy and independent lives [1, 2]. With the growing interest in physical and walking activities for older persons, a substantial amount of research has recently been reported on [3-5].
When compared to studies on young individuals, however, only a few studies have been done on the walking manner of older persons. Additionally, most of these studies have examined the walking functions of older persons from a group perspective. It is necessary to consider the same participants in a longitudinal design. Particularly, older persons vary in their abilities and physical condition, so that examination on a group basis has limitations which makes it difficult to clarify the characteristics of individual older persons.
This situation surely requires a longitudinal study that tracks the same individual continuously on a long-term basis. However, such a study is rarely seen. In addition, almost no studies have been found which focused on and tracked the same older person regarding his/her physical activities along with walking on a long-term basis. Consideration based on the perspective of nursing care surely has significant meaning in order to increase the number of healthy older persons who live in local communities.
For this reason, in this study, we conducted a six-year longitudinal intervention study by measuring the physical activities and walking levels of the older persons that participated in a health class on a continual basis. The goal of this study was to have the older persons become interested in their own physical activities and annual changes in their walking functions. With respect to the timing of the intervention, there was a report that the physical activities and walking focusing on older persons would be affected by seasonal variability [6]. In this study, therefore, we decided to focus on the summer and the winter seasons where the physical activities and walking might be significantly affected.
The present report was about a longitudinal study program of healthy older persons in a community in a mid-latitude area and intended to form the basis of an examination of the effects of seasonal changes on physical activity and the manner of walking in older persons. Two extreme seasons were chosen: mid-summer from the middle of July to the beginning of August and mid-winter from the middle of January to the beginning of February. The study area was a snowy area in the Hokuriku District, Japan.
2. Methods
2.1 Subjects
Of 23 participants who joined the walking support project for older persons, 8 subjects (follow-up rate: 34.8%) in the summer and 7 subjects (follow-up rate: 30.4) in the winter. Their data was collectable even though it was 6 years after for the summer and 5 years after for the winter (from the summer season of 2004 to the summer season of 2010). Of these participants, 6 subjects were the participants both in the summer and the winter. The average age of the participants at the beginning of this survey in the summer was 69.8 ± 3.0 years (6 males and 2 females), while in the winter it was 69.7 ± 2.8 years (5 males and 2 females). All participants were 65 years of age or older. None were inpatients in hospitals or residents of a long-term health care center. All members were active and healthy enough to visit the study venue independently. None of the participants had severe difficulties with their gait nor used walking aids.
2.2 Walking assistance support
We conducted basic physical measurements, along with measurements of physical fitness, daily-life movements, and walking functions twice a year (summer and winter). After these measurements, nurses offered personalized health instructions regarding the changes in the measurement values and daily health conditions. Actions connected with daily life activities, and walking functions, which need extra data analysis from measurement values, were returned to each subject in written form with comment at a later date. This was done in order for the subjects to enhance and maintain their own level of health consciousness by confirming the results they received.
2.3 Measurement parameters and analysis methods
The parameters for the physical measurements and measurement of body fitness included height, body mass, body mass index (BMI), fat ratio, grip strength, and single-leg stance with eyes open. As for daily-life movements, the average steps measured by a pedometer, considered as the average activity amount of a day, along with the ADL ability evaluation parameters. The walking function was evaluated based on analysis of video recorded by using a high-speed camera, with respect to cycle duration, stride, speed, and relative standing time (average of right and left).
Details of the measurements have been described elsewhere [7]. The following is our brief report on the measurement methods. The basic physical parameters and performance measurements were: height, body mass and fat ratio, body mass index; grip strength; and single-leg stance with eyes open. For gait analysis, participants were asked to walk freely to and fro at their preferred usual speed on a level wooden walkway 7 m long in a gymnasium. They were barefoot and wore dark clothing with white ball markers 30 mm in diameter attached at the following points: vertex, acromion (shoulder joint), radiale (elbow joint), trochanterion (hip joint), merionlaterale (knee joint), supratarsalefibulare (ankle joint), and dorsal center of the interphalangeal joint of the big toe. Kinematics while walking in the middle 3 m on the walkway were recorded and analyzed using two charge-coupled device video cameras (MotionMeter 250, Redlake, Tucson, USA) and motion analysis software (FrameDias II, DKH, Tokyo, Japan). Only movements in the sagittal plane are reported on in this current paper. All methods were noninvasive. The study duration for each individual was limited to less than half an hour. The research was performed mainly in the afternoon from about 13:30 to 15:00. From the day following the trial, participants were asked to wear a pedometer (KenzLifecorder EX, Suzuken, Nagoya, Japan) on their waist during waking hours for a week. The mean step count per day was calculated automatically. We used the ADL ability evaluation parameters (ADL score: Demura, 2000) [8]. Single-leg stance duration ended at 60 seconds. Each participant performed two trials and the best score was recorded.
2.4 Statistical analysis
Due to non-normal distribution, differences measurement parameters at the beginning and endpoint of this survey were evaluated using the Wilcoxon signed-rank test.The Wilcoxon signedrank test was applied using the IBM SPSS Statistics 18.0 software (IBM Japan, Tokyo, Japan). A probability (p) value of <0.05 was considered statistically significant.
2.5 Climatic environment
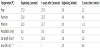
The location of the gymnasium was in Kahoku City of the Hokuriku District, Japan (36˚46.8’N, 136˚44.0’E; altitude, about 35 m) [9]. Climate records for study days are shown in Table 1 [10, 11]. The gymnasium had no air-conditioning, and was warmed by kerosene stoves in the winter and cooled by electric fans in the summer. As no data for snowfall was reported on in Kahoku, we used the data of snowfall at nearby Kanazawa Local Meteorological Observatory (36˚35.3’N, 136˚38.0’E; altitude, 57 m).
2.6 Ethical consideration
All participants for this study received information to explain the purpose of this study, signed a letter of consent, and participated in this survey voluntarily. We also explained to them how data would be handled and that they would have a right to stop participating in this survey any time they wanted, and that their rights to do so would be free from any undue influence due to their participation in this survey.
All study protocols were performed in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Ishikawa Prefectural Nursing University.
3. Results
Table 2 shows changes in the median (25 percentile - 75 percentile) of the measurement parameters of each measurement index at the beginning of this survey and after 6 years of summer and after 5 years of winter.
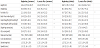
In the summer, there were significant differences in the following five parameters, body fat ratio, grip strength of their right and left hands, single-leg stance, and cycle duration. In the winter, significant differences were observed in the following four parameters, body fat ratio, single-leg stance, cycle duration, and (walking) speed. The body fat ratio decreased in the summer, while increasing in the winter. The grip strength of both hands declined only in the summer. The value of the single-leg stance with eyes open significantly decreased both in the summer and the winter at the end of the intervention. As for walking data, cycle durations were both decreased in the summer and the winter, and the walking speed was increased in the winter. In addition, although no statically significant differences were observed, we saw a tendency that the walking speed could become faster in the summer (p=0.069).
4. Discussion
There were no significant changes in the weather during the survey and no changes in ADL of the subjects were observed before and after intervention were offered. Amid such circumstances, depending on the season, a completely converse result was obtained with respect to increase and decrease of the body fat ratio. It was impossible for us to clarify and determine what actually produced this result in this current study. However, difference in basal metabolism between the summer and the winter and the low temperature in the winter might have influenced this result.
Statistically significant differences were observed in grip strength in the summer. On the other hand, there was almost no change in this value in the winter, while the grip strength of the left hand actually increased although it was not a significant result. It was reported that the grip strength might be affected by the temperature on the skin surface when it comes to seasonal changes in the grip strength [12]. This might affect and make the results of a long-term follow-up small in the winter. As for the result of single-leg stance with eyes open, this parameter value significantly decreased 6 years later for the summer and 5 years later for the winter. The grip strength and single-leg stance are general physical measurement parameters [13,14]. The results of this current study actually demonstrate that the physical fitness of older persons gradually declines as they age.
On the other hand, as for walking functions, there were significant differences in cycle duration in the summer, cycle duration in the winter, and walking speed. Given the possibility that the walking speed parameter in the summer increases based on the comparison with the starting point, which is p=0.069, the same tendency probably continues both in the summer and the winter. When considering these results and the fact that the stride length value stayed almost relatively the same from the beginning of the survey, we can say that these changes in the walking functions of the older persons are unlikely to indicate their unstable walking conditions with a high risk of falling due to wavering steps. Rather, these changes actually show the enhancement of their walking functions. Although the results differ, there is one previous study reporting that older persons became able to walk faster by continuing a 30-minute walking exercise three times a week at their own pace for a year [15]. There was another report that mentions that walking speed could serve as an important prediction factor for physical functions of older persons [16]. Moreover, although no statistically significant differences were obtained, the amount of activity a day (steps a day) increased both in the summer and the winter. This result also shows that there is enhancement of the level of consciousness of older persons for their daily lives, in other words, the effect of the intervention offered by this study. The decrease of the amount of activity a day in the winter when compared to that of the summer showed similar results as other studies [17]. It has been known that the amount of physical activity a day could be affected by temperature [18]. Judging from this fact, we can consider that snow and low temperatures in the winter in the area of the survey might have had an influence.
Based on the above-mentioned results, through data used 5 years and 6 years later, we confirmed that the physical measurement parameters, which are the grip strength and single-leg stance with eyes open, were actually decreased as the subjects aged, while their walking functions were conversely enhanced. Furthermore, it was also confirmed that these results were not affected by seasonal factors. This study demonstrated the possibility that older persons that participated in the walking assistance project can enhance their consciousness for their own health and walking functions so that they can not only maintain their walking functions, but also enhance their walking ability.
One limitation of this study was that we could only follow up on about 30% of the older persons who participated in this project both in the summer and the winter. We can say that these older persons can be referred to as the healthy elite [19]. These could be individuals with extremely good health. However, even amid significant decreases in the values of physical fitness, the grip strength and single-leg stance with eyes open, the walking condition was improved even though these older persons were 70years of old or older. We consider that this result can serve as significant and meaningful data as we consider the future health education of older persons.
5. Conclusion
Our long-term follow-up survey (6 years) confirmed that while some physical measurement parameters were decreased, their walking functions including the cycle duration and the walking speed could be enhanced by the continuous intervention. Maintaining high consciousness in regard to walking can lead to expected improvement in the walking functions of older persons.
Competing Interests
The authors declare that they have no competing interests.
Author Contributions
All the authors substantially contributed to the study conception and design as well as the acquisition and interpretation of the data and drafting the manuscript.
Acknowledgments
We wish to thank all the participants for their time and patience, all the students who helped us, the staff of the Community Care Center in the Ishikawa Prefectural Nursing University, and T. Hashimoto of Kanazawa Medical University.