


1. Introduction
Attention deficit hypertension disorder (ADHD) is characterized by inattention, impulsivity and hyperactivity [1]. A mean worldwide prevalence of ADHD is 2.2% (range: 0.1-8.1%) which has been estimated in children and adolescents (aged <18 years). The mean prevalence of ADHD in adults (aged 18-44 years) from a range of countries in Asia, Europe, the Americas and the Middle East was reported as 2.8% (range: 0.6-7.3%) [2]. In Taiwan, the prevalence of ADHD was 19.8% for boys and 12.3% for girls in elementary students with a boy and girl ratio of 3:1 [3]. Moreover, the problems of inattention and hyperactivity continue to occur in adulthood in more than three-quarters of cases [4].
The etiology of ADHD is complicated, including genetic factors, the abnormal metabolism of neurotransmitters, heavy metal toxicity, food sensitivities, or nutritional problems etc. [5]. Recently, it is assumed that oxidative stress may play an important role in pathology of ADHD [6]. Therefore, antioxidant supplements have been reported to assist the classical treatment of ADHD by psychostimulants and antidepressants because of the side effects of these psych-medicaments [6].
The bark extract of French maritime pine (Pinus pinaster) contains abundant oligomeric procyanidins (OPCs) that are considered as the potent antioxidants with strong antioxidative capacities, such as catechin, epicatechin, gallic acid, caffeic acid, ferulic acid, p-coumaric acid, taxifoliol, ferrulate glucoside etc. [7]. Heimann collected case reports about beneficial effects following treatment of polyphenolic extract (PE) from pine bark in French children with ADHD [8]. Our previous study also showed that ADHD children who received 1 mg/ kg BW/day of PE showed the improvement effects on inattention and impulsivity, and reduction of plasma lipid peroxidation levels during a 4-week experimental period [9]. Therefore, we hypothesized that PE also could improve symptoms of inattention and impulsivity in adults with ADHD, which are well-correlated with elevated antioxidative status. This study was carried out to verify this hypothesis.
2. Methods
2.1 Participant recruitment
The study was approved by the Taipei Medical University (TMU)- Joint Institutional Review Board (protocol ID: N201706026, ClinicalTrails.gov ID: NCT03368690). All procedures were conducted according to principles expressed in the Declaration of Helsinki. Written informed consent was obtained from all participants.
Recruitment was conducted in the psychiatric department of Taiwan Adventist Hospital, Hsuang Ho Hospital from September 2017 to June 2019. Participants, who were aged 20~64 years and attended a preliminary screening session using ASRS (Adult ADHD Self-Report Scale) score (more than 17), SPM+ (Raven's Standard Progressive Matrices Plus; excepted for D level), BDI-II (Beck Depression Inventory, second edition) score (less than 13) and BAI (Beck Anxiety Inventor, second version) score (less than 7). Finally, participants were recruited into the study after being diagnosed with ADHD by a psychiatrist using Diagnostic and Statistical Manual of Mental Disorders, 4th Edition, Text Revision (DSM-IV-TR). The exclusion criteria were as follows: medications, dietary supplements, or neurological disorders which included brain or other central nervous system functions such as epilepsy and intellectual disabilities. Mental disorders (autism, psychosis, bipolar disorder, major depressive disorder, anxiety, personality disorder, conduct disorder, tic disorder etc.) and chronic diseases (liver, kidney, gastrointestinal, cardiovascular diseases, etc.) were also listed as exclusion criteria.
2.2 Intervention
It was a randomized, double-blind, placebo-controlled crossover study. The randomization was perform by drawing lots. Neither the participants nor researchers knew which person was in which group. There were two experimental periods such as including placebo and PE supplementation separated by 2-week washout period. In the first experimental period, ADHD subjects were randomly provided with placebo or PE supplementation for 4 weeks. After the washout period, all ADHD subjects were provided with the other supplement in the second period for 4 weeks. The dosage of PE capsules was modified from the previous literature [10-12]. ADHD participants were provided 2 capsules (body weight more than 40 kg and less than 60 kg) or 3 capsules (body weight more than 60 kg) of PE (each capsules contained 50 mg PE) per day. One capsule contained 50 mg PE (Oligopin®, DRT, Dax, France) including of 67%~75% OPCs, 4%~10% catechin, 4%~10% ferrulate glucoside, 3%~8% taxifoliol glucoside, 1%~5% ferulic acid etc. [7]. Placebo supplements contained maltodextrin and magnesium stearate.
3. Measurements
3.1 Psychological examination
A psychological examinationwas carried out at baseline, 4, 7 and 10 weeks. The evaluation process was assisted by psychiatrists. ASRS and continue performance test III (CPT-III) were used to evaluate the inattention and impulsivity in ADHD participants [13,14]. ASRS included 18 questions which 1 to 9 is for the evaluation of inattention and 10 to 18 is for the evaluation of hyperactivity and impulsivity. The score ranges from “0” (never) to “4” (very often).The higher score indicateshigher levels of ADHD symptom using 17 as a cut-off point for ADHD diagnosis [13].The Conners’CPT-III was also used in this study to evaluate ADHD symptoms. It is a 14-min computerized assessment tool which involves rapid presentation of visual stimuli. During the test, respondents are required to respond when any letter appears, except the non-target letter "X" [14].Wechsler Memory Scale, 3rd edition (WMS-III) was used to assess immediate memory, working memory and delay memory for the ADHD participants [15,16]. Wisconsin Card Sorting TestTM, computer version 4 (WCSTCV4) was used to evaluate executive functions [17].
3.2 Blood collection and analysis
The blood of participants was collected after 8h of fasting at baseline, 4 and 10 weeks in TMU Hospital. The ratio of erythrocytic reduced form of glutathione (GSH) to the disulfide form (GSSG) was measured as an indicator of antioxidative capacity according to the previous study [18]. The GSH/GSSG ratio was calculated as (total GSH - 2GSSG) / GSSG. The lipid peroxidation of plasma samples was determined with a commercial enzyme-linked immunosorbent assay (ELISA) kit including 2-thiobarbituric acid-reactive substance (TBARS) (no. 10009055, Cayman Chemical, Ann Arbor, MI, USA) and 8-isoprostane (no. 516,351, Cayman Chemical, Ann Arbor, MI, USA) [19,20].
In order to monitor the safety of supplements, biochemical parameters were determined including blood cell analysis, liver function indicators (aspartate transaminase (AST) and alanine transaminase (ALT) activities), blood lipid profiles, nutritional status indicator, renal function indicator and iron nutrition status. All items were evaluated with an automated clinical chemistry analyzer (SYNCHRON CX System 7170, Hitachi, Tokyo, Japan).
3.3 Dietary intake assessment
Three-day dietary record was performed in every period. All data were analyzed by Nutrients Analysis Software (2018) established by the Taiwan Dietitian Association. Participants were instructed by dietitians, such as meal portion size and cooking method etc.
3.4 Statistical analysis
Statistical analyses were performed with SAS version 9.4 (SAS Institute, Cary, NC, USA). All values are expressed as the mean ± standard deviation (SD). Differences among groups were compared by the Wilcoxon sign-rank test. P value less than 0.05 was considered statistically significant.
4. Results
4.1 General characteristics
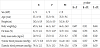
Eleven ADHD subjects, including 2 males and 9 females, were fully engaged in this study (Figure 1), and their general characteristics are shown in Table 1. The mean age at baseline was 35.1±9.6 years. According to the criteria of obesity in Taiwan (BMI>27; fat mass>25% for male, >30% for female), participants were overweight based on BMI and obesity based on fat mass. Blood pressure values were within normal ranges under 120/80 mmHg. When compared to baseline, the fat mass of participants was significantly increased after placebo supplementation.

4.2 Effect of PE supplementation on the psychological examination
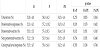
AS shown in Table 2 no difference was found in the inattention item among groups. However, the item of hyperactivity and impulsivity was significantly decreased in PE groups than that of baseline (p<0.05). After 4 weeks of supplementation with PE and the placebo, results of CPT-III are shown in Table 3. No significant difference was found among groups. Only the T-score of commissions showed the lower trend in PE supplementation period (lower values reflected more desirable scores). For the evaluation of memory function, there are some items were significantly increased including word test I and auditory memory span, whereas verbal paired associates I was significantly increased during placebo supplementation period compared to baseline (Table 4). However, no difference was found during PE supplementation period. On the other hand, there are no differences among groups in WCST scores for the evaluation of executive functions (Table 5).


4.3 Effect of PE supplementation on the antioxidative status
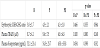
After 4 weeks of PE supplementation, the erythrocytic GSH/GSSG ratio didn't change (Table 6). The plasma TBARS and 8-isoprostane levels showed the lower trend after PE supplementation (Table 6), although the significance wasn’t found.
4.4 Effect of PE supplementation on biochemical parameters
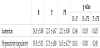
Changes in biochemical parameters of ADHD participants during the experimental period are shown in Table 7. During the placebo supplementation period, the total cholesterol and LDL-cholesterol levels were significantly increased when compared to baseline (p<0.05). On the other hand, during the PE supplementation period, the plasma creatinine level was significantly higher than during the placebo supplementation period (p<0.05), and the potassium level was also significantly higher compared to the baseline (p<0.05). PE supplementation period showed the significantly lower platelet number than placebo supplementation did (p<0.05). However, all values were still within normal ranges.

4.5 Effect of PE supplementation on dietary intake
Dietary intake during the experimental period is shown in Table 8. When compared to placebo supplementation period, the carbohydrate intake was significantly decreased in PE supplementation period (p<0.05).
5. Discussion
5.1 Physiological status
As shown in Table 1, ADHD participants maintained physiological status during the experiment period, although fat mass was significantly increased during placebo supplementation period (Table 1). For monitoring the safety of supplementation, blood biochemical parameters were measured (Table 7). Higher plasma creatinine and potassium levels were found during PE supplementation, but these values were still within the normal range. In addition, participants did not report any adverse events such as nausea, vomiting, poor appetite, etc. The 50% lethal dose (LD50) of PE was >2000 mg/kg BW, and the no-observed-adverse effect level (NOAEL) was 1000 mg/kg BW based on a 90-day study of male and female rats [21]. Only one ADHD patient was reported to have moderate gastric discomfort after PE supplementation in the previous study (1 mg/kg BW/day) [10].
5.2 Neuropsychological function
ASRS was developed in conjunction with the World Health Organization (WHO) and the Workgroup on Adult ADHD to help professionals to screen adult ADHD. In this study, ASRS also used to screen the adult ADHD and used as a indicator for evaluating the beneficial effects of PE. In this study, CPT-III was also used to evaluate inattention and impulsivity in ADHD participants in order to quantitatively analyze data [22]. Tenebaum et al. indicated that no statistically significant difference was detected for the self-reported data including ASRS and CPT after 3-week PE supplementation [23]. In this study, the item of hyperactivity-impulsivity in ASRS was significantly, but no improvement was found in CPT-III, WMSIII, and WCST-IV after 4-week PE supplementation. The length of treatment and dosage of supplements may have contribute the absence of significant differences on the improvement of ADHD symptoms.
5.3 Antioxidative status
Several works on different levels including cell cultures, experimental animal models, and human studies which was deal with effects of PE on brain functions or mental health [24]. These results indicated that PE inhibited oxidative stress, such as increased GSH/ GSSG ratio by normalizing catecholamine levels in ADHD subjects, which may reduce hyperactivity and increase attention [25]. In this study, after 4-week PE supplementation, only plasma TBARS and 8-isoprostane decreased slightly compared to the baseline and placebo but did not reach significance. The relatively small number, dosage and the length of supplementation may be the possible reasons for unobvious influences. Additionally, more evaluation indicators for oxidative stress is necessary for the future study, such as total oxidative status (TOS), total antioxidant status (TAS) and total antioxidant capacity (TAC) and could be useful for identification of redox imbalance in patients with ADHD.
5.4 Dietary intake
Dietary intake did not change during the entire experimental period except lower carbohydrate intake during PE supplementation period (Table 8). Previous research pointed out that dietary intake and nutrition-related factors are associated with symptoms of ADHD [26-28]. Nutrient insufficiency may affect neurocognitive abilities, for example iron as a coenzyme of dopamine and norepinephrine, and zinc as an endogenous neuromodulator in synaptic transmission [29]. In this study, it was also indicated that higher fat intake and lower intake of vitamin A, calcium and zinc compared to DRIs in Taiwan. Therefore, determining food consumption and dietary patterns of ADHD children may be helpful in clarifying relationships between nutritional factors and ADHD symptoms.

5.5 Strengths and limitations
This study evaluated improvements in ADHD symptoms using both an administered questionnaire and quantitative analyses after PE supplementation. Moreover, all ADHD participants were diagnosed without other psychiatric comorbidities and medical treatment. However, this study still has several limitations. First, the sample size was small because of the complicated screening process and assessments. Second, compliance of taking the supplement was 80.2%, which should be increased in future studies. Lastly, more oxidative damage biomarkers should be measured in future study.
6. Conclusions
This study indicated that 4-week supplementation with pine bark extract significantly decreased the hyperactivity-impulsivity based on adult ADHD Self-Report Scale, which represented pine bark extract may have the potential for ameliorating the symptoms of ADHD; however plasma TBARS and 8-isoprotstnae levels only showed the decreased trend in ADHD adults.
Competing Interests
The authors declare no conflicts of interests. Neither Formosa Produce Corporation (Taipei, Taiwan) nor DRT (Dax Cedex, French) has any further role in study design; in the collection, analysis and interpretation of data; in the writing of the report; and in the decision to submit the paper for publication.
Author Contributions
Cheng-Dien Hsu and Suh-Ching Yang designed the study. Cheng-Dien Hsurecruited ADHD participants, and Li-Hsuan Hsieh contacted ADHD participants. The psychiatric evaluation was conducted by Cheng-Dien Hsu, I-Cheng Lin, Ying-Ru Chen and Chih-Chi Chen. Li-Hsuan Hsieh and Ya-Ling Chen also completed blood measurements and statistical analysis of the data. Suh-Ching Yang wrote the manuscript.
Acknowledgments
We thank Formosa Produce Corporation (Taipei, Taiwan) for providing the funds and DRT (Dax Cedex, French) for supplying the pine bark extract. We also thank Dr. Yannick Piriou who provided the professional information and analyzed the composition of the pine bark extract.