



1. Introduction
Sarcopenia is defined as age-related loss of muscle mass [1] . It has been reported that more than 15% of the total skeletal muscle mass would be lost when a person reached 75 years of age which is significantly more than the age related muscle loss of 8% between 40 and 50 years of age [2] . The age-related loss of skeletal muscle mass is a major causative factor to strength decline in the seniors. Around 50% of muscle strength decreased between 60 and 80 years of age [3] and the greatest decline is with concentric dynamic contraction at high speed [4] . It has been well documented that age-related loss of skeletal muscle mass and strength would lead to decrease in balance, mobility and daily independence [2,5] , which are important predisposing factors for functional impairment and physical disability among the seniors [6] .
Physical exercise has been shown to be effective for improving muscle mass, strength and daily life activity in the elderly [7,8] . Sipilä and Suominen [8] reported the cross-sectional area (CSA) of quadriceps increased by 4.5% in the elderly subjects after 18 weeks of lower limb resistance training. Recently, a study with meta-analysis has concluded that medium-term exercise training programs would have positive effects on muscle strength development in the very old age group [9] . On the aspect of physical performance, a randomized controlled trial with 246 elderly people has reported a significant improvement in the timed up-and-go (TUG) test after 18 months of resistance and aerobic training program [10] .
Recent studies have used whole-body vibration (WBV) as a therapeutic intervention to improve muscle size, strength and functional performances in the elderly subjects [11,12] . Machado et al. [11] reported 10 weeks of lower extremity training with WBV could improve the muscle size of biceps femoris and vastus medialis in older women by 15.5% and 8.7%, respectively, and they also found concomitant improvements in muscle strength and functional reported a significant increase in isometric knee extension strength after 72 sessions of WBV training in the old people. Whereas, Raimundo et al. [14] reported no significant improvement in muscle strength after 96 sessions of WBV training program, but it should be noted the intensity of the training program in that study might be too light to induce an observable effect despite having 96 sessions of training. For the physical performance, Pollock et al. [15] reported after 24 sessions of WBV training in the frail elderly subjects, the time taken for them to complete TUG had decreased by 38% and the walking speed had increased by 36%.
Considering the positive effects of WBV training on muscle and physical performance in the normal and frail elderly subjects, this mode of exercise could also be beneficial for the senior subjects with sarcopenia. However, no study had examined the effectiveness of WBV training in people with sarcopenia. Therefore, it is necessary to investigate the efficacy of applying WBV training to improve muscle size, strength and physical performance of senior subjects with sarcopenia.
2. Methods
2.1 Subjects
Community dwelling individuals aged 65 years and above were recruited from a local elderly health center. The older individuals without metal implants, uncontrolled heart problem, neurodegenerative diseases, peripheral vascular disease, vestibular disorders and severe osteoporosis with fractures within one year prior to the study were invited to undergo a bioelectrical impedance assessment to estimate the skeletal mass with an established formula: Skeletal mass (SM) = [0.401 * (height2/bio-impedance) + (3.825 * gender index) – (0.071 * age) + 5.102].
In which the height is in centimeters; bio-impedance is in ohms; gender index for male = 1 and female = 0.
Skeletal mass index (SMI) was calculated as SM/height2 [2,4] . Male and female subjects with SMI less than 8.87kg/m2 and 6.42kg/ m2, respectively, were classified as sarcopenic [16] and randomly assigned into either a WBV group or a control group with a computer program (Research Randomizer Form v4.0). This study was approved by the Human Ethics Review Board of the administrating institution according to the Declaration of Helsinki. All subjects gave their informed written consent before participating in this study.
2.2 Procedures
The vibration training was only conducted in the WBV group in a sports training laboratory of our institution and supervised by a researcher. The training was done 3 days/week for 12 weeks making a total of 36 training sessions. Extra sessions catering for missing appointments were arranged to make sure all subjects have completed the same number of training sessions.
The vertical mode of WBV was used in the present study. The frequency of WBV was set at 40 Hz with a peak-to-peak amplitude at 4mm and one WBV session comprised 4 bouts of 90-second vibration exercise [17] . During training, the subjects stood on the platform of a WBV machine (Fitvibe excel, GymnaUniphy NV, Bilzen, Belgium) without shoes. The knees were kept at 60° of flexion and hands placed onto the rail in front for support. No intervention or training was conducted in the control group. All subjects were asked to maintain their normal lifestyle and physical activity level during the study.
The outcome measurements included muscle size, strength and physical performance. Assessments were conducted at pre- (baseline), mid- (18 sessions) and post- (36 sessions) intervention.
The CSA of VM of the dominant leg was measured with ultrasound imaging. Subjects were positioned supine with a custom-made ankle stabilizer applied to the foot and ankle to keep the leg in neutral rotation. The B-mode of An Aixplorer® ultrasound unit (Supersonic Imaging, Aix-en-Provence, France) was used to capture the CSA of VM at 1/3 of the leg length (measured from anterior superior iliac spine to the medial side of joint line space) above the base of patella [11] . Three images were captured for calculating the average CSA of VM.
The isometric and isokinetic knee extension peak torque of the dominant leg was measured with an isokinetic dynamometer (Cybex Norm, Henley Healthcare, Nauppauge, NY, USA). The isometric peak torque was measured at a knee angle of 90° and isokinetic testing was done at two angular speeds of 60°/s and 180°/s. Subjects were positioned on the testing machine with hip at 80° of flexion and knee axis aligned with the dynamometer axis of rotation. With the trunk and the tested leg firmly secured by straps onto the testing chair, each subject performed two submaximal contractions for familiarization and three maximal contractions for the actual data collection. A 1-minute recovery period was given between testing sessions. The maximum peak torque in the three trials was used for data analysis.
The functional performance test batteries included TUG, 5 times sit-to-stand (5STS) and 10-meter walk (10MWT), as these tests have been recommended to be valid, reliable and suitable assessments for physical function in older people [18,19] . Subjects performed TUG test with their regular footwear and normal walking aid (none, cane, walker). They were to stand up from an armchair, walk a distance of 3 meters, turn and walk back to sit down on the chair with their normal pace without help from another person. Two practice trials were given before the actual test.
For the 5STS test, the subject sat on a chair of 43-47cm high with arms crossed on the chest and feet comfortably placed on the floor. When the researcher said“start”, the subject would rise from the chair to assume a full erect standing position and return to sitting for five times without rest in between. The time taken to complete the test was recorded and the average time of three tests was calculated.
Test-retest reliabilities for all the assessments were established with a 7-day interval with 7 age-matched subjects. All the assessments showed good test-retest reliability (ICC3,1=0.90-0.99).
2.3 Statistical Analysis
Kolmogorov-Smirnov test was used to examine whether the data followed a normal distribution. To compare the baseline characteristics of the two groups, independent-sample t-test or Mann Whitney U-test was conducted. Two-way repeated measures ANOVA (time × group) was used to analyze the raw data for examining the effects of WBV on muscle and physical function. If time effect was significant, contrast analysis would be conducted to analyze the raw data to examine the within-group changes of each group.
Percentage changes from baseline (mid minus pre; post minus pre)/pre × 100 in outcome variables were calculated. Between-group difference at each time point was tested using independent-sample t-test. The last observation carried forward method (LOCF) of intention-to-treat (ITT) analysis was used for data analysis.
Descriptive analyses were reported as means ± standard deviation. SPSS 20.0 (SPSS Inc., Chicago, Illinois, USA) was used for statistical analysis. Significance level was set at p<0.05, unless otherwise state.
3. Results
Forty subjects were recruited in this study (Figure 1). No adverse effect was reported by any of the subjects during the study. The outcome variables of subjects at baseline are summarized in Table 1. No between-group difference in physical characteristics and outcome variables was found at baseline (p>0.05) (Table 1).

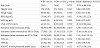
WBV: whole body vibration group; CON: control group; CSA: cross-sectional area; VM; vastus medialis; TUG: Timed up-and-go test; 5STS: Fiverepetition sit-to-stand test; 10MWT: 10-meter walking test. The p values were for between group comparisons.
Significant time × group interaction effects were found for the 180o/s isokinetic knee extension (F2,76=6.216; p=0.003), TUG (F2,76=8.161; p=0.001) and 5STS tests(F2,76=9.220; p<0.001). Subjects in the WBV group showed significant within-group improvements after 36 training sessions in most outcome variables, except for VM size. After 18 training sessions, the TUG and 5STS performances were only significantly improved in the WBV group. Table 2 listed the within-group difference in all outcome variables.

Mid: completion half training session (18 sessions); Post: completion all training session (36 sessions); WBV: whole body vibration group; CON: control group; CSA: cross-sectional area; VM; vastus medialis; TUG: Timed up-and-go test; 5STS: Five-repetition sit-to-stand test; 10MWT: 10-meter walking test. The p values were within-group comparisons versus baseline; * p<0.05 and ** p<0.01.
Significant between-group differences in percentage changes from baseline were found in isokinetic knee extension at 180°/s and 60°/s (Figure 2 & 3), TUG and 5STS at mid-intervention. At post-assessment, significant between-group differences were found in isokinetic knee extension at 180°/s (Figure 2), TUG, 5STS and 10MWT.
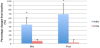
WBV: Whole-body vibration training group; CON: Control group; Mid: completion the half of all training sessions (18 sessions); Post: completion all training sessions (36 sessions); * p<0.05 vs. CON

WBV: whole body vibration group; CON: control group; CSA: cross-sectional area; VM; vastus medialis; TUG: Timed up-and-go test; 5STS: Fiverepetition sit-to-stand test; 10MWT: 10-meter walking test. The p values were for between group comparisons.
4. Discussion
This is the first report of WBV training program on muscle size, strength and physical function in the community dwelling individuals with sarcopenia. The findings of this study suggested that WBV training could effectively improve muscle strength and physical performance in these subjects.
Despite the difference is not statistically significant, the muscle size increased 1.53% in the WBV group. Considering the subjects were community dwelling individuals with sarcopenia who were prone to lose their muscle mass, it would be difficult for the muscles to grow significantly with only 36 sessions of training. For muscle performance, there were significant increases in isometric and isokinetic knee extension after the training in the WBV group, which is comparable to some previous studies that reported the beneficial effects of WBV training for muscle performance in the elderly [11,22,23]. Interestingly, we found the between-group difference in isokinetic strength at 180°/s was significant at both mid- and postassessments but the 60°/s only showed a significant between-group difference at mid-intervention. Furthermore, when compared with 60°/s, the within-group improvement in 180°/s was greater. It is speculated that the fast-twitch fibers in our subjects might have been preferentially stimulated with WBV training because Pollock et al. [24] had demonstrated a lowering in recruitment threshold of fasttwitch motor units after a single session of 6-minute WBV training. If a long-term WBV training program could facilitate the fast-twitch fibers recruitment, it will be extremely important for the management of sarcopenia and frailty in elderly people because the fast twitch muscles are significantly weakened with these conditions. Further research is warranted to shed more lights on this issue.
Increase in muscle strength is associated with better physical performance [25] . Subjects in the WBV group had significant improvements in TUG, 5STS and 10MWT with self-preferred walking speed. The performance in TUG and 5STS had improved after 18 training sessions, which echoed with previous studies that reported significant improvements in 5STS and TUG after 18 and 24 sessions of WBV training [15,23] .
Unlike the TUG and 5STS which had improved after 18 training sessions, the 10MWT did not improve in the first half of the training but it improved within the WBV group after the entire 36 training sessions. It is well known that TUG contained several action components of standing up, walking, turning and sitting down. Therefore, it is possible that the improved completion time of TUG in the first half of training is due to less time spent in standing up. Also, the coordination and balance have a significant role in TUG. A systematic review with meta-analysis reported that WBV could improve balance in the elderly [26] and this could help explain the improved performance in TUG of this study.
There are some limitations in this study. First, the control group had not any intervention. It would have been better to include a sham group to distinguish the effect of static squatting from the effects of WBV training. Second, although all our subjects suffered from sarcopenia, some of them were still quite physically active. The subjects who had difficulty in daily activity could not endure the 36 training sessions and dropped out. Thus, the results of this study may not be generalized to the population with very poor physical condition.
5. Conclusion
A 12-week WBV training program with 36 sessions of 40Hz/360s per session of exercise has positive effects on muscle strength and physical performance in the community dwelling individuals with sarcopenia. The present findings suggested that WBV training is a suitable therapeutic component for improving muscle and physical performance of the community dwelling individuals with sarcopenia.
Competing Interests
The authors declare that they have no competing interests.
Author Contributions
Gabriel YF Ng, Shamay SM Ng and Marco YC Pang: study design
and critical review.
Ruby SY Lee and Mary CK Lau: data collection.
Ning Wei: data collection, data analysis and drafting.
Acknowledgments
I would appreciate the contributions of the elderly subjects from Shatin Elderly Health Center of Department of Health, HKSAR. I would also like to thank Mr. Anson NG, Mr. Ping Kwan, Mr. Siu Sik Cheung, Mr. Man Cheung, Dr. Raymond Chung for their assistance and advices.
References
- Rosenberg IH (1997) Sarcopenia: origins and clinical relevance. J Nutr 127: 990S-991S [CrossRef] [Google Scholar] [PubMed]
- Janssen I, Heymsfield SB, Baumgartner RN, Ross R (2000) Estimation of skeletal muscle mass by bioelectrical impedance analysis. J Appl Physiol (1985) 89: 465-471 [CrossRef] [Google Scholar] [PubMed]
- Aniansson A, Grimby G, Hedberg H, Krotkiewski M (1981) Muscle morphology, enzyme activity, and muscle strength in elderly men and women. Clin Physiol 1: 73-86 [CrossRef] [Google Scholar] [PubMed]
- Poulin MJ, Vandervoort AA, Paterson DH, Kramer JF, Cunningham DA (1992) Eccentric and concentric torques of knee and elbow extension in young and older men. Can J Sport Sci 17: 3-7. [Google Scholar] [PubMed]
- Roubenoff R (2001) Origins and clinical relevance of sarcopenia. Can J Appl Physiol 26: 78-89 [CrossRef] [Google Scholar] [PubMed]
- Janssen I, Heymsfield SB, Ross R (2002) Low relative skeletal muscle mass (sarcopenia) in older persons is associated with functional impairment and physical disability. J Am Geriatr Soc 50: 889-896 [CrossRef] [Google Scholar] [PubMed]
- Landi F, Marzetti E, Martone AM, Bernabei R, Onder G (2014) Exercise as a remedy for sarcopenia. Curr Opin Clin Nutr Metab Care 17: 25-31 [CrossRef] [Google Scholar] [PubMed]
- Sipilä S, Suominen H (1995) Effects of strength and endurance training on thigh and leg muscle mass and composition in elderly women. J Appl Physiol (1985) 78: 334-340 [CrossRef] [Google Scholar] [PubMed]
- Stewart VH, Saunders DH, Greig CA (2014) Responsiveness of muscle size and strength to physical training in very elderly people: a systematic review. Scand J Med Sci Sports 24: e1-10 [CrossRef] [Google Scholar] [PubMed]
- Kemmler W, von Stengel S, Engelke K, Häberle L, Mayhew JL, et al. (2010) Exercise, body composition, and functional ability: a randomized controlled trial. Am J Prev Med 38: 279-287 [CrossRef] [Google Scholar] [PubMed]
- Machado A, García-López D, González-Gallego J, Garatachea N (2010) Whole-body vibration training increases muscle strength and mass in older women: a randomized-controlled trial. Scand J Med Sci Sports 20: 200- 207 [CrossRef] [Google Scholar] [PubMed]
- von Stengel S, Kemmler W, Engelke K, Kalender WA (2012) Effect of wholebody vibration on neuromuscular performance and body composition for females 65 years and older: a randomized-controlled trial. Scand J Med Sci Sports 22: 119-127 [CrossRef] [Google Scholar] [PubMed]
- Verschueren SM, Roelants M, Delecluse C, Swinnen S, Vanderschueren D, et al. (2004) Effect of 6-month whole body vibration training on hip density, muscle strength, and postural control in postmenopausal women: a randomized controlled pilot study. J Bone Miner Res 19: 352–359 [CrossRef] [Google Scholar] [PubMed]
- Raimundo AM, Gusi N, Tomas-Carus P (2009) Fitness efficacy of vibratory exercise compared to walking in postmenopausal women. Eur J Appl Physiol 106: 741-748 [CrossRef] [Google Scholar] [PubMed]
- Pollock RD, Martin FC, Newham DJ (2012) Whole-body vibration in addition to strength and balance exercise for falls-related functional mobility of frail older adults: a single-blind randomized controlled trial. Clin Rehabil 26: 915-923 [CrossRef] [Google Scholar] [PubMed]
- Chien MY, Huang TY, Wu YT (2008) Prevalence of sarcopenia estimated using a bioelectrical impedance analysis prediction equation in communitydwelling elderly people in Taiwan. J Am Geriatr Soc 56: 1710-1715 [CrossRef] [Google Scholar] [PubMed]
- Marín PJ, Rhea MR (2010) Effects of vibration training on muscle strength: a meta-analysis. J Strength Cond Res 24: 548-556 [CrossRef] [Google Scholar] [PubMed]
- Paul SS, Canning CG (2014) Five-repetition sit-to-stand. J Physiother 60: 168
- Podsiadlo D, Richardson S (1991) The timed "Up & Go": a test of basic functional mobility for frail elderly persons. J Am Geriatr Soc 39: 142-148 [CrossRef] [Google Scholar] [PubMed]
- Cruz-Jentoft AJ, Baeyens JP, Bauer JM, Boirie Y, Cederholm T, et al. (2010) Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing 39: 412-423 [CrossRef] [Google Scholar] [PubMed]
- Wolf SL, Catlin PA, Gage K, Gurucharri K, Robertson R, et al. (1999) Establishing the reliability and validity of measurements of walking time using the Emory Functional Ambulation Profile. Phys Ther 79: 1122-1133 [CrossRef] [Google Scholar] [PubMed]
- Roelants M, Delecluse C, Verschueren SM (2004) Whole-body-vibration training increases knee-extension strength and speed of movement in older women. J Am Geriatr Soc 52: 901-908 [CrossRef] [Google Scholar] [PubMed]
- Sitjà-Rabert M, Martínez-Zapata MJ2, Fort Vanmeerhaeghe A3, Rey Abella F4, Romero-Rodríguez D3, et al. (2015) Effects of a whole body vibration (WBV) exercise intervention for institutionalized older people: a randomized, multicentre, parallel, clinical trial. J Am Med Dir Assoc 16: 125- 131 [CrossRef] [Google Scholar] [PubMed]
- Pollock RD, Woledge RC, Martin FC, Newham DJ (2012) Effects of whole body vibration on motor unit recruitment and threshold. J Appl Physiol (1985) 112: 388-395 [CrossRef] [Google Scholar] [PubMed]
- Pisciottano MV, Pinto SS, Szejnfeld VL, Castro CH (2014) The relationship between lean mass, muscle strength and physical ability in independent healthy elderly women from the community. J Nutr Health Aging 18: 554- 558 [CrossRef] [Google Scholar] [PubMed]
- Lam FM, Lau RW, Chung RC, Pang MY (2012) The effect of whole body vibration on balance, mobility and falls in older adults: a systematic review and meta-analysis. Maturitas 72: 206-213 [CrossRef] [Google Scholar] [PubMed]