


1. Introduction
Hypoglycemia (hG) , defined as a blood glucose level (BG) less than 70 mg/dL or 3.88 mmol/l [1,2] , is “a true medical emergency that requires prompt recognition and treatment to prevent organ and brain damage” [3]. During the course of diabetes, it is reported that 1 out of 4 patients are at risk of developing hypoglycemia [4]. In the hospital setting, up to 26% of patients have been reported to experience hypoglycemia [5], which can increase hospital stay and the risk of mortality the year following admission [6]. Knowledge and awareness about hypoglycemia is a safety issue in the management of diabetes. Hypoglycemia is considered to be a barrier in the optimal control of diabetes [7] for both inpatient and outpatient diabetic patients.
Our facility (RLANRC) is a tertiary rehabilitation medical center that provides healthcare to patients with brain or spinal cord injuries. Diabetes and associated comorbidities are common among our inpatient and outpatient population. Insulin therapy is frequently used in the management of diabetes for the inpatient population, and standard insulin regimens (preprandial bolus insulin and basal insulin at night) are reported to contribute to iatrogenic hypoglycemia [1-3,8]. Other risk factors that increase the risk of hypoglycemia among diabetic patients include inadequate food intake secondary to dyspepsia, nothing per oral (NPO) status in anticipation of surgery or other procedures, use of standard corrective insulin doses, etc. At our hospital, hypoglycemia is reported via the Patient Safety Network (PSN), which represents a voluntary reporting system of anything that can affect patient safety. This is frequently done anonymously and predominantly by the nursing staff. Analysis of these events helps prevent potential errors and allows the overall improvement of patients’ safety. The purpose of this study was to monitor the PSN for hypoglycemic events, before and after an intervention designed to decrease the frequency of inpatient hypoglycemia among diabetic patients.
2. Materials and Methods
A hospital-wide intervention to prevent hypoglycemia was piloted on March 2013 and included the following four interventions: 1) basal/long-acting insulin (Lantus/Glargine) was switched to morning administration instead of night administration; 2) bolus/short acting insulin (Novolog/Lispro) was used after meals rather than before or with meals; 3) supplemental insulin coverage was modified using lower than standard doses, and 4) insulin administration was withheld if patients' food intake was less than 50%. The outcome of this intervention was done by assessing the number of hypoglycemic episodes reported as PSN events before and after the intervention. The number of hypoglycemic episodes that occurred during 12/2012- 3/2013 (4 months ) before the implementation of this pilot program during, was compared with the number of hG episodes reported in the intervention group during 4/2013 -7/2013 (4 months). We also monitored the use of D50% as a rescue treatment for hypoglycemia based on the data provided by the inpatient pharmacy.
3. Analysis
Descriptive statistics were used to identify the demographic characteristics of the study population. Fisher exact test was used to compare the frequency of hypoglycemic events in patients who received standard insulin regimen vs those in the intervention group . A p value < 0.05 was considered to be statistically significant.
4. Results
4.1 Retrospective PSN review
During the 8 month study period a total of 46 episodes of hypoglycemia were reported in the PSN events. All 46 inpatients (34 male and 12 female patients) who experienced hypoglycemia have type 2 diabetes. Their mean age was 56.7+/- 10.1 years old. The range of blood glucose levels were between 51-69 mg/dL (2.83-3.83 mmol/l) in 17/46 (37%) of patients and < 50 mg/dL (2.77 mmol/l) in 29/46 (63%) of patients. In the latter category, five patients required the rapid response team to rescue them from hypoglycemia.
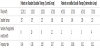
Of the 46 episodes of hypoglycemia, 36 episodes (78%) occurred before the implementation of the pilot project. Changing the time of basal insulin administration was found to be beneficial for both type 1 and type 2 diabetes [12,13]. The frequency rate of hypoglycemia in this control group was 0.16 episodes per patient per year. In contrast, the number of hypoglycemic episodes in patients who participated in the pilot project (intervention group) was 10/46 (22%) episodes, representing a frequency rate of 0.04 episodes per patient per year (Table 1). Using Fisher’s exact test to compare the frequency rate of hypoglycemia among the control group vs intervention group, we found that patients in the control group were 3.66 times more likely to develop hypoglycemia compared to the intervention group (p<0.05).
In monitoring the use of D50% to correct hypoglycemia, the number of patients who received intravenous (IV) D50% was 34 in the control group and 10 in the intervention group. This represents a 70% decrease in the utilization of IV D50% in the intervention group (Figure 1).

5. Discussion
Our pilot study showed that hypoglycemia is common among inpatient diabetic population, and two out of three patients who were reported to have hypoglycemia, have a BG less than 50 mg/ dL (2.77mmol/l). The frequency rate of hypoglycemia among our inpatient diabetic population is in the range reported in the literature [9]. According to Mustafa and Choudhary (2014) one out of four diabetic inpatients may experience hypoglycemia [5,10], which is reported to be a neglected complication of diabetes with multiple negative implications [11]. These implications include increased sympatho-adrenal response, neurocognitive changes, endothelial dysfunction, and blood coagulation abnormalities [11]. These changes underscore the importance of hypoglycemia, as a common complication of diabetes care, and the urgency to recognize it, to treat it, and especially to prevent it.
Based on our clinical observation and the review of data from the monthly Medication Safety Committee meetings, we found that hypoglycemia among the diabetic inpatient population occurred more frequently when basal insulin was given at bedtime and/or bolus insulin was given prior to meals. These represent the standards of insulin administration, and is true for the combination of both NPH/Regular insulins and also for the combination of analog insulins (Glagine/Humalog ). As a result of our observation, our first intervention to prevent hypoglycemia included the use basal insulin in the morning instead of the night time. Changing the time of basal insulin administration was found to be beneficial for both type 1 and type 2 diabetes [12,13]. Our second intervention to prevent inpatient hypoglycemia addressed the administration of bolus insulin (Humalog on formulary) in the postprandial period instead of before meals. Post-meal administration of short-acting insulin was previously reported to reduce the risk of hypoglycemia [14]. According to Maynard, use of bolus insulin postprandial was beneficial in preventing hypoglycemia due to “nutritional interruption” or the discordance between insulin administration and food intake [12]. The authors considered the latter as one of the most important risk factors for drug-induced hypoglycemia [12]. Some examples of nutritional interruption that we have encountered among our inpatient diabetic population are: nausea, vomiting, altered mental status related to drug therapy (i.e. narcotics) or presence of gastroparesis. The latter was reported to be present in 25 to 55% of type 1 diabetics [15,16] and 30%with type 2 diabetes [17]. Gastroparesis is particularly common in our disabled patient population who have a long history of diabetes and multiple micro and macrovascular complications. This form of autonomic neuropathy that affects the gastric motility can be the result of diabetic neuropathy, hyperglycemia [18] or may be a side effect of certain drug therapy (i.e., medication with anticholinergic effect, tricyclic antidepressants, etc.). Gastroparesis is known to increase the risk of hypoglycemia [17,19,20], and administration of the shortacting/ bolus insulin in the postprandial period was reported to reduce this risk [21,22]. The third intervention, to prevent hypoglycemia, involved the adjustment of supplemental insulin doses. Compared to the standard regimen, which uses an average of two units of shortacting insulin for each 50 mg/dL of blood glucose above the target level, we adjusted the supplemental insulin doses using a lower dosage (i.e. 0.5 to 1 unit of insulin for each 50 mg/dL of BG above the target level). The elimination of the high-dose insulin correction scales from the insulin order sets was reported by Pasala et al. (2013) to help decrease the incidence of inpatient hypoglycemia [2]. Our fourth pilot project intervention was to withhold the bolus insulin if the food intake was inadequate. In this sample of type 2 diabetics, we did hold the short acting/bolus insulin if food intake was less than 50%. This intervention was based on Maynard et al (2008) study, which showed that, inadequate food intake without adjustment of insulin dosage can be the “most important risk factor for iatrogenic hypoglycemia” [9].
Implementation of the above changes involved active participation of all stakeholders, including health care providers, nursing, and patients. Inpatient pharmacy played an instrumental role in helping the healthcare providers with the pilot project compliance. The pharmacists called the prescribing physicians and helped by giving instructions regarding the changes in the standard insulin administration protocols. We found that clinicians’ compliance with the use of new insulin regimens required constant education, one -to-one instructions, sharing of preliminary data and continuous reminders of the need to use the newer insulin regimens. Rancho Diabetes Health and Wellness Committee, a multidisciplinary forum created to educate both patients and healthcare providers regarding diabetes, helped by informing the nursing staff, patients and their families regarding the changes in the standard insulin regimens and our efforts to prevent hypoglycemia. The role of educational programs in preventing hypoglycemia was emphasized in several studies [1,23,24] as modalities to help understanding the need of individualized, rational and safe therapies [25]. Insulin is among the high-alert medications [26] and iatrogenic hypoglycemia, despite being prevalent and potentially a cause for serious harm [27] continues to be neglected [24]. To manage diabetes safely, it is essential to address this preventable complication.
6. Limitations
The limitations of this study include: small sample size, short duration of study time, and use of data reported as PSN events, which was conducted anonymously and predominantly by the nursing staff. Hypoglycemic events could be more frequent than what was documented by PSN. In addition few of our patients were on oral agents (n=4) or a combination of NPH/regular insulin (n=3) therefore, the changes on basal/bolus insulin did not apply to them. The only intervention that may decrease the incidence of hypoglycemia in these few patients who were on oral agents or NPH/regular insulin, was the decrease in the corrective insulin doses. Another limitation of this study was related to the use of Glargine insulin only as a basal insulin therapy, due to formulary constraints.
7. Conclusion
Despite the limitations described above, this paper highlights several important messages. Inpatient hypoglycemia is common, and most of the patients experienced dangerous levels of low blood glucose. Documentation of hypoglycemia is very important to promote patient safety in the management of diabetes. Morning administration of basal insulin and the administration of bolus insulin postprandial helps to reduce the inpatient hypoglycemia, particularly for patients who may experience the “unexpected nutritional interruption/ discordance” [9]. The decrease in standard doses of corrective insulin may also have a beneficial effect in reducing the risk of hypoglycemia [2]. Overall, preventing hypoglycemia by addressing the potential predisposing factors could decrease patient harm, improve diabetes control [2] and quality care.
Competing Interests
The authors have no competing interests with the work presented in this manuscript.
Author Contributions
Stefan Bughi, MD, MACM- is the author who initiated the project, and had substantial contribution in the writing of the abstract, presenting the preliminary data as oral presentation, and had a major contribution in the write up the paper. He followed the completion of this project from start to end.
Shanpin Fanchiang, OTRL, PhD - participated in the writing of the paper and helped with statistical analysis and patient education.
Brian Joyo Pharm D.- Chief pharmacist who helped with data review and discussion of hypoglycemic cases, and also helped with the write up of the manuscript.
Richard Wong, MD- Chief Pharmacy and Therapeutic Committeehelped with data review, analysis of results and participated in the write up of paper.
Almara Nazarian, Pharm D- was instrumental in collecting the PSN data, helped with data review, and participated in the write up. Helped by educating the providers to use the new insulin regimens and monitored compliance.
Brian Kekehashi, Pharm D. - helped with data review, documentation of hypoglycemic case and the write up of paper. Helped by educating the providers to use the new insulin regimens and monitored compliance.
Sunshine Shahinian, RN, Diabetes Educator- helped with patient and health care providers education RE new changes in the insulin protocols.
Sheetal Desai ( Research Assistant) and Paul Dillaway, Tatjana Jones - are medical students who helped with data collection, data entry and participated in preparing the poster and paper for publication.
Sylvia Shaw, MD, MACM – is a co- initiator of the project and its implementation, who participated in the write up of abstract, oral presentation of the preliminary data and had a major contribution in write up of the paper.
Acknowledgments
The authors thank the Rancho Diabetes Health and Wellness Center for their continuous support of patients and their family’s education, the Ortho/Diabetes nursing staff for their enthusiastic support and efforts to implement this pilot study and Dr. Stephanie A. Bughi for editorial assistance.