


1. Background
It has been a long time since the Enhanced Recovery After Surgery Protocol [1] and the fast-track surgery protocol [2] were proposed, and postoperative early ambulation has been shown to be useful in preventing postoperative complications. However, in many cases, bed rest is prioritized over ambulation in patients immediately after surgery because of unstable respiration and hemodynamics. Currently, it is standard practice to start ambulation on the first day after gastrointestinal surgery in a rehabilitation program, where the criteria for ambulation are to start sitting or walking[3,4]. Bed rest is necessary immediately after surgery, but continued bed rest causes decreased peripheral perfusion, venous blood flow stasis in the lower extremities, decreased intestinal peristalsis, and decreased muscle mass. These can lead to serious complications such as deep vein thrombosis and intestinal obstruction.
In our previous study, early postoperative intermittent mild exercise on the bed improved peripheral perfusion [5]. Although the incidence of postoperative complications was not evaluated, the relationship between peripheral perfusion and the incidence of postoperative complications has been clarified in previous studies [6], and exercising immediately after surgery has been suggested to prevent postoperative complications. In addition, active movement of the lower limbs after surgery is useful in preventing deep vein thrombosis[7,8], and lower limb trunk movement prevents postoperative intestinal obstruction[9] has been reported. Furthermore, early postoperative exercise is recommended to prevent the onset of sarcopenia [10,11] and it is expected that combining these exercises into a single program may prevent postoperative complications.
To the best of our knowledge, no study has focused on exercise therapy performed immediately after surgery. Thus, we aimed to develop exercises to prevent postoperative complications that can be performed immediately after surgery while lying in bed. This study is a pilot study to evaluate whether the exercise program we devised can be implemented in surgical patients and evaluate its validity and usefulness in the healthy elderly.
2. Methods
2.1 Study design
This prospective, comparative study from November 2021 to March 2022 included healthy elderly individuals and was approved by the author's university ethics review board (21-A061: Ethical Committee of the Graduate School of Nursing Sciences, St. Luke's International University, Tokyo, Japan).
2.2 Participants
Most patients undergoing surgery were elderly, with a decreased reserve capacity due to age; therefore, we judged that they were suitable for this study and were considered in the inclusion criteria.
The inclusion criteria were age over 65 years, body mass index between 18.5 and 25 kg/m2, and proficient linguistic communication. Exclusion criteria included participants with exercise restrictions imposed by a doctor, participants with paralysis or disability in the limbs, and participants who received peripheral blood vessel treatment.
G-POWER version 3.1 software was used to determine the sample size. To calculate the appropriate sample size in this study, with reference to previous studies, the effect size was calculated using the perfusion index as the primary endpoint and the selection parameters [F tests, ANOVA repeated measures, effect size = 0.5, α err prob = 0.05, power = 0.95, number of groups 1, number of measurements 14], and it was estimated to be nine participants. Therefore, considering dropouts, we determined the optimal sample size for this study to be 10 participants in advance.
2.3 Interventions
The participants were in a supine position on the bed, exercised for approximately 10 min based on the devised program, and the perfusion index and vital signs such as blood pressure and pulse rate were observed for 5 min every hour after the exercises.
Based on a literature review, factors such as exercise site, type, intensity, duration, and frequency were determined, and a program was created based on the opinions of specialists. These specialists include anesthesiologists who specialize in perioperative general condition management, surgeons who perform surgery and postoperative management, physiotherapists who specialize in perioperative rehabilitation, and nurses who have practical experience in perioperative nursing. Since it is performed immediately after surgery, postoperative rest and movement restriction, infusion vein line and drain placement, and degree of pain and discomfort were taken into consideration. Figure 1 shows the framework of the complication-prevention exercise program immediately after surgery.

The program consisted of grip movement of the fingers, active movement of the lower limbs, and lower limb trunk exercises.
2.4 Grip movement of fingers
A study measuring blood flow velocity in the brachial artery showed a significant promotion of blood flow after 20 grasping exercises each of which were performed at a pace of once per second[12]. Therefore, in this study, we decided to perform the grasping exercise once per second for 30 seconds with the left and right hands simultaneously.
2.5 Active movement of the lower limbs
It has been reported that performing dorsiflexion-plantar flexion exercises of the ankle joint once every 4 s for 5 min resulted in a superior improvement in blood flow over the intermittent air compression method [13]. Therefore, we decided to perform dorsiflexion-plantar flexion of the ankle joint once every 4 s for 5 min at the same time for the left and right feet.
2.6 Lower limb trunk movement
Intestinal peristaltic movement sounds have been associated with lower limb trunk movements [14]. Therefore, it was decided to perform flexion and extension exercises of the hip and knee joints once every 10 s for 2 min, and to rotate the trunk to the left and right in the supine position once every 5 s for 2 min.
These exercises were less than 4 METs [15], which is the standard for patients undergoing surgery under general anesthesia, and it was considered that they could be performed without any problems in terms of exercise tolerance. The exercise program was a combination of these exercises for approximately 10 min and was carried out continuously.
2.7 Measurements
The perfusion index and vital signs were recorded on a laptop computer at 5-min intervals throughout the measurement period. Measurements using each method were continued for 1 h in order to characterize and analyze the changes in the measured values over time.
The perfusion index, SpO2, and pulse rate were measured using Radical-7™ (Masimo rainbow SET Pulse CO-Oximeter, MASIMO, USA) and recorded on a laptop computer at 5-min intervals throughout the study period. The index finger was used to measure the perfusion index in both the upper and lower limbs. Blood pressure was measured with an automatic sphygmomanometer (Elemano2, TERUMO, JAPAN) and recorded every 5 min. Intestinal peristaltic sounds were measured for 1 min using a stethoscope (Littman®, 3M, USA) and recorded every 5 minutes.
Dyspnea and feeling tired were evaluated before, immediately after, and 10 min after the exercises using unmarked new 100 visual analog scale (VAS) sheets. For dyspnea, 0 and 100 indicated "Not at all breathless" and "Extremely breathless", respectively. For feeling tired, 0 and 100 indicated "Not tired at all" and "Extremely tired," respectively.
2.8 Data analysis
All statistical analyses were performed using SPSS® Statistics software (v27.0; IBM Corp., Armonk, NY, USA). Continuous, normally distributed variables were analyzed using repeated-measures analysis ANOVA. Differences between points were compared using Bonferroni's method. All values are expressed as mean ± SD and p < 0.05 was considered to be significant.
2.9 Ethical considerations
Based on the inclusion and exclusion criteria of this study and the operation schedule, the chief investigator approached the candidates and disclosed the purpose of the study, the research methods, and other precautions prior to their participation. The participants' rights and privacy were protected throughout the study. Each participant completed a written informed consent form and had the right to withdraw from the study at any given time for any reason. Information pertaining to participants' privacy was kept confidential, and the research findings were maintained to uphold each participant's rights.
3. Results
The perfusion index and vital sign data were obtained from all 10 participants. The mean duration of exercise, including intervals, was 629 ± 28.1 sec. The participants included 5 men and 5 women, with a mean age of 70.3 ± 5.9 years and a mean BMI of 23.5 ± 1.7 kg/m2 (Table 1).

Figure 2 shows the transition of the perfusion index of the upper and lower limbs from before exercise to 1 h after exercise. The pre-exercise upper limb perfusion index was 1.8 ± 2.7. The perfusion index immediately after exercise, after 5 min of exercise and after 10 min of exercise was 2.7 ± 1.1, 2.4 ± 1.2, and 2.1 ± 1.1, respectively, which were significantly different from the values before exercise (P <0.01, P <0.01, P = 0.03, respectively). The pre-exercise lower-limb perfusion index was 0.9 ± 0.2. The perfusion immediately after exercise was 1.2 ± 0.2, and the perfusion index after was 1.0 ± 0.2, which was significantly different from the pre-exercise values (P <0.01, P = 0.03). Figure 3 shows the transition of indicators showing the load on respiratory and circulatory dynamics from before exercise to 1 h after exercise.
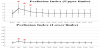

The pre-exercise pulse rate was 63.5 ± 3.2 times/min. The pulse rate immediately after exercise was 71.4 ± 2.3 times/min, and the pulse rate after 5 min of exercise was 69.4 ± 2.8 times/min, which were significantly different from the values of pre-exercise (P <0.01, P <0.01, respectively).
The pre-exercise systolic blood pressure was 132.5 ± 12.4 mmHg, which was not significantly different from other points. The pre-exercise SpO2 was 99.2 ± 1.1, which was not significantly different from the other points.
Figure 4 shows the transition of intestinal peristalsis from before exercise to 1 h after exercise. The pre-exercise value of the number of intestinal peristaltic sounds was 3.7 ± 1.6 times/min, which was not significantly different from other points.
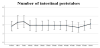
Figure 5 shows VAS scores for feeling tired and dyspnea. The VAS score of feeling tired was significantly higher immediately after exercising than before exercising and no difference was observed in the score between before exercising and 10 minutes after exercising (6.5±3.2, 11.3±5.4, 6.9± 0.2, respectively). The VAS scores for dyspnea did not differ between three points (7.1±3.6, 8.1±4.3, and 7.1±3.4, respectively).

4. Discussion
The purpose of this study is to develop an exercise program that improves peripheral perfusion and prevents postoperative complications that can be applied to patients immediately after surgery. As a preliminary test, the usefulness was verified in healthy elderly individuals. It was clarified that the exercise program devisedin this study improved peripheral perfusion, and that it lasted for approximately 5 to 10 minutes. In addition, although the pulse rate temporarily increased due to exercise, blood pressure and SpO2 were stable, and the load on respiration and circulation was not high; therefore, it is safe to further develop these exercises for surgical patients.
Postoperative pulmonary complications are among the most common pathological conditions encountered in postoperative patients [18,19]. Cardiovascular complications also cause a variety of symptoms, such as arrhythmia angina, and perioperative blood pressure control is of particular importance [20]. As this study aimed to develop an exercise program for patients immediately after surgery, it is necessary to reduce the burden on respiration and circulation as much as possible. SpO2 did not differ at any point throughout the measurement period compared with before exercise. The pulse rate increased predominantly from immediately after exercise to 5 min after exercise, but the circulation was maintained by increasing the pulse rate, and the contractile blood pressure after exercise was not different from that baseline. In the subjective evaluation of the participants, although they felt more tired immediately after the exercise than before, they returned to the same level as before the exercise 10 min later. It should also be noted that the VAS score immediately after exercise was 11.3 ± 5.4, which is not high because it is judged that there is a symptom of 20 or more in general. In addition, there was no difference in dyspnea immediately after exercise compared with that before exercise. When evaluated comprehensively, it can be said that the load on participants was not high.
Zhang et al. reported that a care bundle that includes physical exercise immediately after surgery promotes gastrointestinal function recovery and seems to improve intestinal peristalsis [21]. Moderate abdominal pressure by exercise improves intestinal peristalsis, and prevention of intestinal obstruction is expected to prevent postoperative complications. Although no significant difference in intestinal peristalsis was confirmed in this study, it should be determined in future studies.
5. Limitations of the study
This study had several limitations. First, the study population was limited to healthy elderly individuals with limited age and BMI ranges, and these factors have significant effects on perfusion index and vital sign changes. Thus, further research is required with a larger variety in the population of surgical patients. Second, the protocols for participant movement restriction on the bed were not strictly controlled, which might have affected the results. In particular, the different methods of spending time in bed would have had different effects on the measurements.
6. Conclusion
To prevent complications that can be tackled during the period from immediately after surgery to getting out of bed, we examined the prevention of complications that can be started immediately after surgery even under the condition of bed rest.
It was confirmed that the exercise program devised in this study was expected to improve peripheral perfusion, and the load on the subjects was light in this study, targeting healthy elderly individuals. This verification provided valuable data and proved that it could be developed into an intervention study for patients undergoing surgery. In the future, it will be necessary to develop clinical research with postoperative complications as the main endpoint after examining exercise load through research targeting surgical patients.
Competing Interests
The authors declare that they have no competing interests.
Acknowledgements
The author would like to thank all participants who cooperated in this study and the nursing faculty members who consulted during the data analysis.