


1. Introduction
Pneumonia is the third leading cause of death among all age groups in Japan, but yearly deaths from pneumonia are increasing particularly among the elderly. In 2016, 97.3% of pneumonia deaths were of people 65 and older; among those in long-term care pneumonia is the leading cause of death at 30%. In fact, it is said that most elderly deaths in nursing care facilities are a result of pneumonia. Many elderly pneumonia cases are caused by pulmonary aspiration, and the rate of cases of pulmonary aspiration increases with age [1]. In a nationwide study conducted by Yamasaki [2], 80% of pneumonia in patients 70 and older was found to be aspiration pneumonia.
Aspiration occurs when, owing to a decline in oral function, chewed food does not move smoothly from the pharynx to the stomach. From some previous studies [3], it is clear that declining oral function among the elderly is a primary factor leading to severe conditions such as pneumonia, and it is closely related to health prognosis.
Oral function is a key body function, so its efficacy decreases with age. In recent years, efforts to maintain or improve oral function among elderly people are spreading in Japan. Oral exercises are used as a general approach with dependent elderly people. The oral cavity consists of many muscles which can be trained by oral exercise, so theoretically the muscles around the oral cavity can be strengthened as well. Thus, it is thought that oral exercises can maintain and improve oral function. Currently, they are widely used as preventive nursing care in Japan. However, current evidence for the effect of oral exercise is insufficient. Therefore, in this study, we aim to clarify the impact of oral exercise on the oral function of dependent elderly people.
2. Methods
Dependent elderly individuals were guided through oral exercises, and we investigated oral function before and after their implementation.
For our oral exercise methods, we consulted some previous studies which reported that effects could be expected [4]. Furthermore, we used exercises that elderly individuals could continue no matter their mental and physical condition, care personnel, caregivers’ burden, or other factors. Medical welfare professionals such as nurses, physiotherapists, caregivers, etc. conducted group exercise guidance for elderly subjects for about 15 minutes per day, once a day, at least 3 days a week (Figure 1). The exercises included neck, shoulder, and upper limb region movement forward and back and up and down, tongue area motion exercise, lip opening and closing motions, cheek inflation and deflation, vocal exercises, deep breaths, and the like. Oral function was evaluated before oral exercise, 3 months after exercise, and 6 months after exercise.

2.1 Research subjects
The subjects of the survey were Japanese dependent elderly persons over 65 living in nursing facilities who, after reaching mutual understanding, consented to the study. Additionally, they were able to continue with the oral exercise regimen. Furthermore, the nursing facility that conducted this survey is positioned as an intermediate facility for medical care and welfare, and the average number of days for elderly people is about 100 days. After leaving the facility, the elderly patients move to one’s home or permanent residential welfare facility.
2.2 Survey items and evaluation methods
2.2.1 Basic status
We received information about subjects’ age, gender, and nursing care level from the host institution’s staff. In Japan nursing care is categorized into five levels. Level 1 indicates the lightest need for nursing care, and level 5 indicates the most serious need for care.
2.3 Oral functions
The following two items were examined: tongue pressure and oral diadochokinesis.
2.3.1 Tongue pressure
TPM-01, a tongue pressure measuring instrument (manufactured by JMS Co., Ltd., Hiroshima, Japan, Figure 2), was used to measure tongue pressure. This tongue pressure measuring instrument comprises a digital tongue pressure meter, connecting tube, and tongue pressure probe. The balloon section of the tongue pressure probe, which was automatically pressurized as predetermined by the measurement device, was inserted onto the oral part of the tongue while the participant was seated; the participant was instructed to elevate the tip of the tongue to the palate at a maximum force for 5 to 7 seconds, during which the intensity of the force that crushed the balloon was measured. The tongue pressure measurement was performed twice consecutively in accordance with the method described in previous studies [5], and the mean of the measured values was recorded as the tongue pressure level (kPa). Elderly adults aged 70 years or older are considered to require a tongue pressure level of 20 kPa or greater [5].

2.3.2 Oral diadochokinesis
Oral Diadochokinesis (OD) was used. OD is regarded by Japan’s Preventive Care Project’s oral function improvement program as an indicator of articulation function. Participants are asked to alternately repeat “pa/ta/ka” syllables as quickly as possible, and the frequency of utterances is assessed. For measurement, an automatically counting OD-measuring instrument called Kenkou-kun (manufactured by Takei Scientific Instruments) was used [6]. Five second intervals of vocalization were performed in a quiet room, and from that five second interval a one-second average utterance rate was calculated.
2.4 Data analysis
Before oral exercise was implemented, after 3 months, and after 6 months, associations with the oral functions were analyzed using a paired one-way analysis of variance. The significance level was set to less than 0.05. The statistical software IBM SPSS Ver. 25.0 was used for the statistical analyses.
2.5 Ethical considerations
This study was conducted after obtaining consent from the participants as well as from individuals affiliated with the surveyed facilities; the following were fully explained to the participants and affiliated individuals: the study purpose, procedure, optional nature of study participation, protection of personal information, and results publication.
In addition, the survey in this study was conducted after obtaining approval from the Research Ethics Review Committee of the School of Nursing at the Himeji University (2016-N005).
3. Results
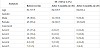
3.1 Basic attributes (Table 1)
There were 62 subjects (19 males and 43 females) before starting oral exercises, average age 82.7 ± 7.9 years old. Among them, 29 (46.8%) required nursing care of level 1 to 2, and 33 (53.2%) required care level 3 to 5. After 3 months, the number of subjects was 36 (12 males, 24 females), average age 84.5 ± 5.9 years old. Among them, 14 (38.9%) required nursing care level 1 to 2, and 22 (61.1 %) required care level 3 to 5. After 6 months, the number of subjects was 25 (9 males, 16 females), average age 84.0± 6.4 years old. Among them, 11 (44.0%) required nursing care level 1 to 2, and 14 (56.0 %) required care level 3 to 5.
3.2 Oral functions
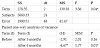
Tongue pressure values before oral exercise, after 3 months, and after 6 months are shown (Table 2).

3.3 Tongue pressure
Average tongue pressure before exercises was 22.52±9.44kPa, and 20 participants (32.3%) did not achieve a force of 20kPa, which is considered a standard value for those aged 70 years or older.
The average after three months was 24.80±10.90kPa, and 11 participants (30.6%) did not achieve a force of 20kPa. The average after six months was 26.85±10.56kPa, and 8 participants (32%) did not achieve a force of 20kPa.
3.4 Oral diadochokinesis
The average /pa/ value prior to exercise was 4.0±1.1 times per second; after three months the average was 4.2±1.2 times per second; after six months the average was 5.3±3.6 times per second.
The average /ta/ value prior to exercise was 4.1±1.2 times per second; after three months the average was 4.1±1.2 times per second; after six months the average was 5.4±3.6 times per second.
The average /ka/ value prior to exercise was 3.6±1.2 times per second; after three months the average was 3.8±1.0 times per second; after six months the average was 4.7±3.3 times per second.
3.5 Analysis of oral function before and after oral exercise
Oral function evaluation values before oral exercises, after 3 months, and after 6 months were analyzed using a one-way analysis of variance corresponding to each tongue pressure value and each OD value. There was a significant difference between tongue pressure values before and after oral exercise (p less than 0.05, Table 3), but no significant difference was found in any OD value.
4. Discussion
4.1 Current oral functions among dependent elderly persons living in nursing facilities
In this study, the present condition of oral function of elderly patients needing primary nursing care admitted to nursing rehabilitation facilities was clarified by assessing tongue pressure and articulation function.
Although tongue pressure is the force required to send chewed food to the pharynx at the time of swallowing, it is reported that the decrease in the tongue pressure of the elderly also affects chewing function [7] and meal form [8].
Among these subjects, about 30% did not reach 20kPa [5], which is a measure of tongue pressure over the age of 70 years, and there is concern about potential adverse effects on aspiration.
As for OD, compared with a study of 218 people receiving home nursing care (/pa/ 4.9±1.5 times per second, /ta/ 4.8±1.4 times per second, /ka/ 4.5±1.3 times per second) [9], the value before oral exercise as well as three months after starting were low.
From these results, it is clear that there are considerable numbers of elderly persons who suffer oral function deterioration entering nursing facilities. The oral function of dependent elderly people is not only a physical health issue but is also related to Quality of Life [10], so we believe it is necessary to actively take some approach to maintain or improve oral function.
4.2 Association between oral functions and oral exercise
Based on previous studies, oral exercises in this study were made into methods that can be implemented at facilities. After 3-month and 6-month intervals of oral exercise, we assessed oral function using tongue pressure and OD. The tongue is a power source that moves the food taken into the oral cavity onto the teeth and mixes the crushed and milled food with saliva to form a bolus [11], accomplishing an important role in the feeding process. It is thought that the amount and strength of the tongue muscles decreases in the elderly [12,13], and the tongue pressure value also decreases accordingly. In this study, we observed a significant increase in tongue pressure after oral exercise.
Therefore, our study suggests that oral exercise is effective in improving tongue pressure. While no significant difference was observed in the tongue pressure value after 3 months, nevertheless a significant difference was confirmed after 6 months. For that reason, in order to prevent deterioration in tongue pressure due to aging, we believe that a continuous long-term effort of about 6 months is necessary.
Regarding OD, there was no significant difference observed after oral exercises. Accordingly, improvement on articulation function among dependent elderly patients from a 3-month period of oral exercise is considered weak. However, when comparing the average value of each OD before and after oral gymnastics, an increase in the value is observable, so upon reassessing the methods and so forth, we think we can expect such results.
Previous studies have revealed that the presence or absence of exercise for tongue movement and lip movement among oral exercise is related to OD [9]. Therefore, we think that there is a possibility that the articulation function improves by strengthening the tongue movement and lip movement.
Competing Interests
The author declare that there is no competing interests regarding the publication of this article.
Acknowledgments
The authors would like to express their heartfelt gratitude to all personnel involved with the nursing facility that collaborated in this study, as well as the dependent elderly persons who participated in the surveys.