


1. Introduction
Axillary temperature measurement is the preferred method in Japan, primarily because this method is noninvasive and convenient. However, there are some instabilities before the temperature display accurate core body temperature, which can lead to inaccurate data collection [1]. This method involves measuring the temperature of the axillary cavity close to the deep part of the body. It is therefore necessary that the upper arm touches the thorax to form a complete axillary cavity and the tip of the thermometer is placed at the deepest part of the cavity and this posture is maintained to obtain accurate data [1-3].
Use of the predictive measurement electronic thermometer is gaining popularity in Japan since it allows for quick and easy measurement of body temperature. In fact, a survey conducted in Japan reported that 44.0% of research subjects used predictive measurement thermometers at home [4]. The predictive measurement thermometer is able to predict the equilibrium body temperature within a short period by using an arithmetic expression that is obtained from processed data. This results in the ability to measure temperature in a period as short as 30 or 90 seconds [5,6]. While this method is simple and easy, it has been pointed out that there is a possibility that the actual value is inaccurate by more than one degree in the case of a predictive expression less than 35.0 degrees Celsius [7]. If the tip of the thermometer is placed in the deepest part of the axillary cavity and measured, this type of error can be improved [8]. To ensure the proper placement, a thermometer angle between 30 to 45 degrees to the upper body is recommended. However, it has been reported that there is a low implementation rate of the correct method [9], therefore, education regarding the correct axillary temperature measurement method is of the utmost importance to increase awareness on how to obtain an accurate measurement.
Body temperature measurements are a part of health maintenance in daily life, and the environment greatly influences the acquisition of the correct method [10]. Many healthcare behaviors are transmitted from parents to children and are learned as vital components of a healthy lifestyle. Several studies have indicated that health behaviors, including children’s prosocial and problematic behaviors, are influenced by relationships with caregivers; the associations between antismoking actions [11], treating caries [12,13], eating behaviors to avoid childhood obesity [14], and family relationships are said to be protective factors against unwanted teenage pregnancies [15,16]. Some children’s behaviors are directly related to parental behaviors. In addition, several studies have suggested that maternal education and practices are possibly effective in enhancing children’s health status [17,18]. In order to ensure the healthy development of children, it is necessary to highlight the importance of caregiver influence. Among the numerous and varied relationships that individuals experience, there is little doubt that the mother-child relationship is the most influential [19]. If the acquisition of healthcare behaviors is influenced by the relationship between an individual and the primary caregiver, then maintaining a good relationship between these two individuals is crucial, not only to help preserve a persistent family relationship but also to help in obtaining good health practices.
The current study considered the axillary temperature measurement method as a fundamental health behavior and sought to examine whether a good mother-child relationship was associated with the agreement regarding axillary temperature measurement methods between mothers and their children. In addition, it aimed to explore if there are other effective means to spread the correct measurement methodology. These analyses could provide information about the mother’s role in children’s health maintenance and could help to identify ways to disseminate more information about appropriate measurement techniques.
2. Methods
2.1 Study design
This study used a noninvasive intervention. The study procedure is shown in Figure 1. After obtaining informed consent, the participants were given a self-administered questionnaire in their classrooms at the conclusion of a regularly scheduled lecture. This allowed individuals who did not wish to participate in the opportunity to leave prior to the start of the survey. The participants measured their axillary temperatures with their own thermometers every morning for one week and recorded the results. Following this, they watched an educational video [9], measured their axillary temperature for an additional week, and completed the self-administered questionnaire once again.

2.2 Setting, data collection, and participants
This study was conducted with students in a nursing course at a university in Fukuoka, Japan. Data collection began in April 2014 and concluded in December 2014. A total of 435 students were invited to participate in the study. In total, 236 enrolled, 102 participants completed both questionnaires, and 84 also completed the two axillary temperature measurements.
2.3 Questionnaires
The first questionnaire included basic demographic characteristics, body temperature measurement methods, the Maternal Consciousness Scale [20], and the current mother-child relationship as well as during childhood. The second questionnaire included items regarding the participants’ mothers’ axillary temperature measurement method, what behaviors were overlooked or performed incorrectly when measuring body temperature (multiple answers up to 3) and should be emphasized items to enhance correct measurement (multiple answers up to 3).
The Maternal Consciousness Scale measured principles considered “motherly,” and consisted of attributes present or absent in traditional Japanese mothers. The reliability and validity of this scale were previously reported [20]. The questionnaire concerning the motherchild relationship during childhood was introduced in a preceding study [21]. It consisted of three components (secure, avoidant, and ambivalent) with 16 items. The current mother-child relationship questionnaire consisted of 26 items and was also introduced in a previous study [22]. All three questionnaires were scored on a 5-point Likert scale.
2.4 Educational video
The first half of a video program titled “TAION WO HAKATTEMIYOU”, presented by Terumo Corporation [9], was used in the study. The program stresses three points: (1) the thermometer tip must be in the center of the axillary cavity; (2) the thermometer angle should be adjusted to about 30 degrees with respect to the upper body; and (3) this posture should be maintained for 20 to 30 seconds. A different source has suggested that the correct thermometer angle is 45 degrees [23]. Because of the importance of thermometer placement on the diagonal and upward angle, the angle established in the current study was between 30 to 45 degrees. This information was further conveyed to participants after they watched the video.
2.5 Data analysis
IBM SPSS Statistics 22.0 was used for data entry and data analyses. The characteristics (mean, standard deviation, frequencies, and percentages) of the participants were calculated. A Student’s t-test was used to compare averages of the axillary temperature measurement data before and after the intervention among the group that completed the questionnaires and measurement sets. In order to confirm whether past results are applicable to the subject of this study, the composition of questionnaires on current and past mother-child relationships was confirmed using factor analysis. In addition, the agreement of the measurement method between the participants and their mothers was dichotomized, and a logistic analysis was used to evaluate whether the agreement of the measurement method was associated with the basic demographic characteristics of the participants and/or the mother-child relationship. A p-value of less than 0.05 was considered statistically significant. Furthermore, a simple tabulation was used to gather information on the two questionnaire items that identified possible factors associated with disseminating the correct method.
2.6 Ethical considerations
The survey was designed to allow for fully voluntary participation. Participants who refused to answer questionnaires and/or measure their axillary body temperature were excluded from analyses. All of the participants signed written consent forms prior to their participation in this study. The study protocol was approved by the Ethical Committees of the study site and a separate research organization to which the author belongs.
3. Results
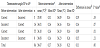
The characteristics of participants are shown in Table 1. Subjects ranged in age from 18 to 23 years, with 99.1% identifying as electronic thermometer users. The agreement of the correct thermometer angle for body temperature measurement between the participants and their mothers before watching the educational video (intervention component) was 50.0%. Table 2 shows the mean observed axillary temperatures before and after the intervention. The mean temperatures before and after the intervention were 36.07ºC and 36.18ºC, respectively, which was significantly different (p<0.001). The changes in the thermometer angle before and after the intervention that were assessed by the questionnaires were divided into four groups, and the overall mean for all groups increased after the intervention.

The agreement rate of the correct thermometer angle adjustment between the participants and their mothers was 70.6% (Table 1). The participants who completed the measurements of their axillary temperatures were divided into two groups based upon whether the axillary thermometer angle between the participants and their mothers were the same. In the second analysis, the correlation between the agreement of the method and the mother-child relationships of participants were examined.
There were no significant relationships between the agreement rate and basic demographic characteristics. At the beginning of the second analysis, the factor structure of questionnaire items regarding participants’ mother-child relationship, at present or during childhood, was confirmed. The past mother-child relationship questionnaire items determined three components: stable, negative, and ambivalent types of relationship, in the same manner, as previously reported [21]. Concerning the current mother-child relationship questionnaire, previous research concluded that this metric was composed of two categories [22]. The confirmatory factor analysis of the current study’s population found three components: autonomy, trust, and dependence (Table 3). This analysis explained 48.05% of the cumulative contribution rate and indicated the highest level of validity. The Cronbach’s alpha indices were acceptable for all factors and were found to be 0.875 (autonomy), 0.813 (trust), and 0.721 (dependence). Taking this information into account, these components were used in the subsequent analysis.

The results of the logistic regression analysis are shown in Table 4. Significant associations were found between the agreement of the axillary temperature measurement method and the total score of the current mother-child relationship in Model 1. When the three components of the past and present mother-child relationship were introduced, instead of the total scores, the correct classification rate of the regression model increased from 65.7% to 70.6%. As shown in Model 2, trust and dependence, which are components of the present mother-child relationship score, were significantly associated with the agreement of the method used. The adjusted odds ratio (AOR) of the correct thermometer angle before and after the intervention was 2.52 in Model 2, but the p-value failed to reach statistical significance (p=0.084).
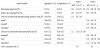
Figure 2 and figure 3 show the results of a simple tabulation of the identified problems in measuring body temperature measurement and the items that should be emphasized to encourage correct measurement methods. In these multiple-response items, 75 participants reported that the problem in measuring body temperature was that the palm could not be kept facing upwards and 43 responded that keeping the palm facing upwards should be emphasized in proper education on temperature measurement method.


4. Discussion
First, the results showed that “trust” and “dependence” components of the present mother-child relationship were independently and significantly associated with the agreement of the body temperature measurement method utilized. Establishment of a sense of trust is one of the essential goals for a healthy relationship between parents and children, as well as an important component of future relationships. Trust plays a role in relationships with parents and peers across childhood and adolescence, and it is also crucial for psychosocial functioning [24]. A basic sense of “trust” means, “When I need you, you will be there.” A child who is experiencing a satisfactory attachment in the relationship with his/her caregiver may be more likely to explore the surrounding environment guided by a sense of trust that his/her caregiver will be there. Through this exploration of the environment, the child gains greater competence and independence in future experiences [19]. This theory suggests that a high mean score of the “trust” component, shown in Table 4, should be indicative of the respondent’s awareness of a secure motherchild attachment. This result may reflect suitable transmission from mother to child of body temperature measurement methods, based on a consistent mother-child relationship.
A significant relationship between the “dependence” component and the level of agreement shown in Table 4 is a contradictory result. Several studies have pointed out that adolescence is a time of selfdiscovery when attachment is important for coping and confronting negative situations [25], and that dependency in later developmental periods results from a lack of confidence in oneself and others [19]. However, especially in industrialized societies, many adolescents have yet to enter the enduring responsibilities of adult life. Currently, a new concept of “emerging adulthood,” which is a period from the late teens to the twenties, has been proposed [26]. According to this theory, individuals in this stage tend to remain happy with their living situations (i.e., living with parents), and they continue to rely on their parents as a source of several types of support, including financial support [27]. The participants in the current study ranged in age from 18 years to 23 years, all of them were students, and most were living with their family (as shown in Table 1). As such, it is likely that many of the participants are in the “emerging adulthood” period. Considering these results, an environment where delayed independence is permitted and expected may not be unpleasant for participants in the current study, and thus the “dependence” component may reflect positive parent-child relationships. Similar to the “trust” component, the higher mean score on the “dependence” component might reflect suitable transmission of methods to measure body temperature, based on a comfortable mother-child relationship. In addition, a statistically significant difference was not observed in the “autonomy” component of the current mother-child relationship metric through the logistic regression analysis. Similar to what is found in other industrialized countries, many young Japanese people obtain higher education and their development frequently changes based on life circumstances and opportunities. Emerging adulthood can be explained as a period that offers many opportunities for identity exploration [26]. If the participants are in the emerging adulthood stage of their development, the lack of statistical significance of the “autonomy” component might be influenced by these circumstances. Likewise, the discrepancy between the present mother-child relationship components of past research and this study might be explained by these situations.
Second, results of this study identified items that could be considered effective for guiding the correct axillary temperature measurement method. While it was initially believed that maintaining the right thermometer angle was critical, this study found that stressing palm direction is also important. Specifically, when the palm faces upwards, the knee joint flexes, the forearm rotates outward, and the upper arm naturally closes to the thorax. Accordingly, stressing that the “palm faces upwards” when teaching about measurement could be helpful for increasing the rate of accurate body temperature measurement.
Third, watching an instructional video about temperature measurement is thought to be an effective educational tool. Previous surveys have indicated that the normal axillary temperature beforenoon, measured with a computerized electronic thermometer, is between 35.66°C and 37.16°C, with a mean of 36.40°C [28]. Therefore, the mean axillary temperature data in this study was thought to be within the normal range. Prior to this study, it was predicted that the axillary temperature measurement value would increase after a change in the correct measurement method. However, the result may suggest that participants used more care in measuring their temperature after watching the video. The information in the educational video program might be effective for expanding health education and the utilization of correct methods; however, more research is needed to fully address this possibility.
The rate of indicating the correct thermometer angle prior to the intervention in the current study was higher than the result reported previously (32.8%) [4]. Because the participants were university students in the nursing department, this result was somewhat expected; however, the value was not ideal, as we would expect an advanced skill set in this population. The reason for this percentage may be due to the use of separate conceptualizations of body temperature measurement methods for themselves and for their patients.
5. Limitations
This study has several limitations. First, some results did not reach statistical significance, as described above. Second, the sample size of this study was small. Among the 435 students, 23.4% completed the two questionnaires, and 19.3% completed both axillary temperature measurements. This was likely due to the attempt to maintain the independence of voluntary participation. In addition, a high proportion of participants in the study were female. This may limit the generalizability of the findings to a wider population. Further, this study ignores several kinds of discrepancies among family members in terms of how they affect participants’ behaviors. Discordance between the parent and adolescent is an important phenomenon of healthy adolescent development [29]. Parent-adolescent conflicts, as well as mother-father discrepancies regarding their children might negatively impact children’s behaviors [30,31]. Further research should include various additional aspects of the study population. Despite these limitations, the results of the current study pointed out multiple aspects for expanding correct health behaviors.
6. Conclusions
The results of this study indicate that the level of agreement between the participants and their mothers on the method of obtaining axillary temperature measurements is significantly associated with presently secure mother-child relationships. This finding implies that a mother’s health practices may influence the acquisition of her children’s health behaviors, in association with a good mother-child relationship. A good mother-child relationship should be developed for the effective transmission of health behaviors and current mothers and those planning to care for children in the future should be targeted for fundamental health education for expanding good health behaviors across generations. In addition, stressing that the palm should face upwards and introducing educational videos should be useful for education regarding accurate body temperature measurement.
Competing Interests
The authors declare that they have no competing interests.
Author Contributions
KK was responsible for the study design, data collection, analysis of data, and manuscript preparation. YS contributed to the study design and the ethics in research.
Acknowledgments
I would like to express my sincere gratitude to my colleagues and the university students who participated in this study.