


1. Background
For years depression was considered to be an adult disease but it's now recognized that most major mental illnesses begin in adolescence and early onset is highly related to recurrence in adulthood [1]. Accordingly, adolescent mental health has been designated by Healthy People 2020 as an important topic area with the specific objective to reduce the proportion of adolescents aged 12 to 17 years who experience major depressive episodes [2]. An example of data supporting the need for this HP2020 objective is found in the 2013 Youth Risk Behavior Survey (YRBS), which was conducted among students in grades 9-12 in the United States. Findings indicated that during the12 months before the survey, 29.9% of students nationwide had felt so sad or hopeless almost everyday for two or more weeks in a row that they stopped doing some usual activities, 17% had seriously considered attempting suicide, 13.6% of students had made a plan about how they would attempt suicide, 8% had attempted suicide once or twice 12 months before the survey and 2.7% had made a suicide attempt that resulted in an injury, poisoning, or overdose that had to be treated by a doctor or nurse [3]. Depression is a known risk factor for suicide [1,4] and more completed suicides have been found to occur in rural areas than urban [5]. Rural adolescents who live with depression face mental health care access issues not experienced by their urban peers. Also, rural areas are more likely to be designated as mental health care provider shortage areas [5]. The Federal Collaborative for Health Disparities Research selected mental health disparities in rural areas as warranting national research attention because rural residents experience unique mental health disparities that are influenced by multiple determinants at the individual, community, program, system, and policy levels [6]. There is evidence that protective factors at these levels can protect adolescents from the onset of depression [7]. Therefore, it is important to consider the socio-ecological context in which adolescents live and be aware of the risks and assets of environment to their health [8].
Photovoice is a research method that compliments CBPR and is unique because it uses photography to promote elicitation and identification of significant phenomena. Photovoice provides visual information that is not available in traditional qualitative approaches such as interviews and focus groups [9]. The use of Photovoice as a method in CBPR studies is becoming more prevalent and there is increasing evidence that Photovoice can be used as a participatory tool for engaging communities in the CBPR process successfully [10,11]. The intent of Photovoice as a CBPR method is to address individual- level change and community and policy-level change [12]. The three main goals of Photovoice are to enable people to document their community’s assets and concerns, promote critical dialogue about important community issues, and reach policymakers [13]. Photovoice studies have been implemented around the world with vulnerable populations of all ages [11] and has also been used to address social justice and public health concerns with underserved communities across the globe [14]. Photovoice has been found to be especially appealing to adolescent populations and has resulted in outcomes that are important to adolescent empowerment and health promotion [11,12,15]. Researchers can increase the chances that their study findings will be applicable to children and adolescents if they partner with youth to identify content area, research questions, data collection methods, and dissemination efforts [16]. Photovoice encourages verbalization through discussion of photographs, which can be an effective means of addressing and securing participation for some adolescents who do not usually volunteer for research [17].
2. Method
This article describes a participatory study that used a unique and creative research approach to partner with rural adolescents to identify perceived risk and protective factors for depression. A sub-aim of this study was to carry out a preliminary evaluation of the relationship between participation in Photovoice and youth empowerment. Empowerment has been reported as the result of raised critical consciousness and social action in previous Photovoice studies with adolescents [12,15, 17-26]. By participating in research that has been tailored to address the unique needs of adolescents, they may gain empowerment, a sense of importance, and knowledge concerning the importance of policy and social change [12]. Also, growth in the areas of leadership, character, self-esteem, sense of responsibility, and civic engagement may be seen as a result of engaging in participatory and empowering methodologies [27].
This study adapted the application of Photovoice as a Community- Based Participatory Research (CBPR) method to identify perceptions of rural adolescent youth about risk and protective factors for depression. Allowing adolescents to share their perceptions about important issues through Photovoice builds upon earlier adolescent research that obtained data from interviews with parents, teachers, and physicians [28]. Past Photovoice studies have been used with youth to empower and engage them in community and policy change [29].
2.1 Overview of the Photovoice Methodology
To mobilize community action when working with adolescents as partners in the research process, Wang, an original conceptualist of Photovoice, recommends following a nine step strategy when working with youth [29]. These nine steps are:"1) select and recruit a target audience of policy makers or community leaders, 2) recruit a group of Photovoice participants, 3) introduce the Photovoice method to participants, and facilitate a group discussion about cameras, power, and ethics, 4) obtain informed consent, 5) pose initial themes for taking pictures, 6) distribute cameras to participants and review how to use the camera, 7) provide time for participants to take pictures, 8) meet to discuss photographs and identify themes, and 9)plan with participants a format to share photographs and stories with policy makers or community leaders" [29, p. 149].
2.2 Study Timeline and Procedural Steps
The following timeline was developed for this study with the recommended time span and nine step strategy for youth Photovoice studies in mind. Institutional Review Board approval was received prior to initiation of the following Timeline as was a Certificate of Confidentiality.
Community Advisory Board recruitment. Proposal review by board-Month 1
Recruitment of Participants-----------------------------------------------Month 2
Participant Photovoice Training-------------------------------------------Month 3
Data Collection (Photo Assignments/Interviews)-----------------------Month 4
Data Analysis/PI Coding----------------------------------------------------Month 5
Data Analysis/Interactive group discussion------------------------------Month 6
Dissemination Activities----------------------------------------------------Month 7
Step 1. Selection and recruitment of target audience of policymakers or community leaders
A voluntary Community Advisory Board (CAB) comprised of local policymakers and community leaders was formed through Primary Investigator (PI) recruitment efforts. The primary role of a CAB in a Photovoice study is to serve as a group with the political will to put participants’ ideas into action [29]. CAB recruitment efforts by the PI resulted in voluntary participation of one public school board member, two university psychiatry and nursing department faculty, one Board of Health member, and two psychologists. According to CAB members, curiosity related to the Photovoice method compelled them to volunteer for membership. Community Advisory Board members reviewed and provided feedback for the study proposal and consent form. They also attended dissemination activities.
Step 2. Recruitment of a group of Photovoice participants and Step 4. Obtaining informed consent
Sample: Participants were adolescents between the ages of 11 and 17 who had a current or prior clinical diagnosis of a depression made by a licensed mental health or primary care provider. Adolescents were not allowed to participate in the study if they had been recently hospitalized for depression or suicide attempt, deemed high-risk for suicide, or self-reported suicidality. The sampling strategy was purposive. To meet inclusion criteria, the participant must have
- been between the ages of 11 and 17;
- resided in one of the three study counties;
- had a current or previous diagnosis of a depressive disorder from a licensed mental health or primary care provider;
- maintained regular mental health care provider visits as prescribed by their provider;
- been willing to participate in research that included taking photographs and exploring perceptions of adolescents who live with depression,
- been willing to attend meetings with other participants, parents/ guardians, and community advisory board members; and
- been willing to share photographs with a small group for discussion.
Local psychologists, psychiatrists, mental health counselors and primary care physicians agreed to assist in recruitment by distributing informational flyers to potential participants who met inclusion criteria. The recruitment of participants from diverse school districts and communities in participating counties was sought to limit recognition and minimize confidentiality issues and stigma for participants. After one month of recruitment efforts, using the phone number on the informational flyer, eight adolescents voluntarily contacted the PI by phone and expressed interest in the study. Wang states that 7 to 10 participants is an ideal group size when working with youth [29]. After attrition, the study was conducted with seven participants.
Consent: Verbal permission from the participant and parents/ guardians to visit their home to obtain written consent/assent was obtained during the adolescent’s initial phone call. The consent form was assessed for readability by the Fogg Test (5.2 grade level) and the Flesch-Kincaid Test (9.2 grade level).Written permission from the participant’s mental health care provider was obtained by the PI. A signed release of information by the parent/guardian was also required and kept at the mental health provider’s office. Parents/ guardians were instructed in the consent form that information disclosed by their child during individual and group interviews would not be shared with them, but that they could request a copy of study findings and attend photograph exhibits where the child could identify his or her own photos. Participants consented to the use of their photographs for educational and publication purposes, which included internet usage. Involvement of parents/guardians was encouraged and important for provision of support and development of pride in participant’s work [12].
Step 3. Introduction of the Photovoice method to participants, and facilitation of group discussion about cameras, power, and ethics and Step 6. Distribute cameras to participants and review how to use the camera.
Method and camera: Group training sessions were held at a local community arts hall because it was safe, accessible, and convenient geographically to participant, parents, advisory board, and researcher. The first group training session was led by the PI, lasted two hours, and was attended by participants, parents, and CAB members. Importance of confidentiality of individual identities and of information disseminated during group sessions was emphasized. This first session provided information about the purpose and aims of the study and the Photovoice method. Another purpose of the first training session was to establish rapport and trust among participants and between study participants and the PI. Participants and parents/ guardians were given the opportunity to discuss meeting content and have all of their questions answered. Instruction emphasized that the Photovoice method is more than just taking photographs. The history, development, and strengths of Photovoice as a participatory method was shared through a Powerpoint® slide presentation. Examples of prior Photovoice studies with youth was also shared. Communication style by the PI was delivered as appropriate to the cognitive level of the adolescent. Each participant was given a digital camera that they were allowed to keep after the study ended. A local professional photographer provided instruction in camera and photography basics for a nominal honorarium.
Ethics and Power: There were ethical and safety issues to consider. Researchers must remain cognizant of individual variation when dealing with young people’s ability to comprehend the purpose of research, the risks involved and their rights [30]. Young people may not understand that they can actually choose not to participate, or even cease participating part-way through [30]. Specific instructions for participating and/or ending participation in this research project were included in the consent/assent form. The PI used appropriate age-level terminology when conducting, informing, and obtaining consent. Participants were informed that if they disclosed information to the PI that could be considered important for parents or provider to know during individual and group interviews, the PI would need to share this information with the health care provider and parent/guardian. If participants disclosed information that indicated dangerousness (defined as threat to life) to self or others, the adolescent was told they would be immediately referred to the health care provider and parent/ guardian. Participants were informed of this potential action in the first training session and in the consent form.
Step 5. Pose initial themes for taking pictures
The PI guided participants to take photos of risk and protective factors for their depression. Risk factors were defined for participants as things that influence or have influenced them to be depressed or more depressed. Protective factors were defined as things that protect them from being depressed or have influenced them to not be depressed or less depressed. To minimize the potential for bullying and stigmatization, participants were asked not to take pictures within their school environments or when they were with other adolescents. If participants wished to photograph risk or protective factors that were associated with other adolescents or within their school environment, they were instructed to take pictures of things that were representative of those issues without being physically present with other adolescents or on school grounds. Participants were instructed not to take identifiable photographs of other individuals. Examples of how this could be accomplished were shared during the first training session. Contact information for the PI and reminders of the photo assignment topic were given to participants and parents/guardians by phone call. If a participant had shared digital images or information that suggested bullying, the parent/guardian and health care provider would have been notified. If the bullying had occurred at school, a conference would have been scheduled with the student, parent/ guardian and school official.
Step 7. Provide time for participants to take pictures
Participants took photographs over a two-week time period after the first training session. The first week’s photo assignment was to take pictures of things that represented risk factors for adolescent depression. For the second week’s photo assignment, participants took pictures of things that represented protective factors for adolescent depression.
Step 8. Meet to discuss photographs and identify themes.
Individual interviews: Individual semi-structured interviews were held between the investigator and each participant to discuss their photographs. Interviews took place at the participant’s home or other preferred site, and were digitally recorded for professional transcription. Participant photographs were downloaded onto the investigator's laptop computer. Photograph and interview data storage was encrypted. Participants were asked to choose five to ten photographs that were most significant to them out of their collection for discussion during the interview. The mnemonic “SHOWed” guided the interviews and participant discussion about photographs by asking: What do you See here? What's really Happening here? How does this relate to Our lives? Why does this situation, concern, or strength exist? And, What can we Do about it? [31,29]. These are “root-cause” questions that help identify and discuss the issue at hand and develop strategies for change [32].
Participants were also asked the following questions:
1) How does this photo relate to your life as an adolescent who has
experienced depression?
2) What has your community done or not done about the risk and
protective factors that you identified?
3) What would you like your community to do about the risk and
protective factors that you identified? and
4) What can we do to educate other people in your community about
the issues you identified?
The individual interviews were concluded by the investigator summarizing and asking for validation of summaries.
Group Interviews: As a form of member checking, a group interview was planned to be held after all individual interviews and data analysis were completed to allow for participant discussion and validation of PI findings. According to IRB proposal requirements, mental health provider presence was required during group interviews in case of participant distress. However, mental health providers informed the PI they would not attend because they felt their presence would affect participant responses. Therefore, the group interview had to be cancelled.
Step 9. Plan with participants a format to share photographs and stories with policy makers or community leaders
To disseminate findings to policymakers, community leaders and the general public, participants were asked how they would like their photographs to be shared with their community. For this study, participant suggestions included photo exhibits and website development.
2.3 Parental involvement
Parents’ support and questions were encouraged throughout the project. Involving parents/guardians in youth Photovoice projects is important to provide support and develop pride in participants' work [12]. Parents/guardians were invited and attended the initial participant training session and dissemination activities. Parents/ guardians were informed that they could contact the PI, the University Institutional Review Board (IRB) Office or their child’s mental health care provider at any time if they had questions or suggestions. Contact information for the PI and the IRB were included in the consent form.
2.4 Empowerment
Evidence of empowerment as a result of participation in this study was evaluated through a pre- and post-test scale called The Brief Perceived Opportunity for Empowerment Scale (BPOES). The BPOES was originally developed for middle school youth [33]. It is a five-item Likert scale consisting of the following items: 1) my neighborhood involves youth in important decisions, 2) I am given lots of chances to make my neighborhood better, 3) I am given chances to work with other young people and adults in my neighborhood to make it better, 4) young people my age are able to make a difference in my neighborhood, and 5) if I feel strongly about an issue, I would talk to people in power (such as mayor, school board, city council, etc.) about my opinion [33]. Each item is scored on a five-item Likert-type response scale (a. strongly agree, b. agree, c. not sure, d. disagree, e. strongly disagree). In their study of perceived youth empowerment, Paxton et al. purposed to determine the factor structure, validity, and reliability of the BPOES [33]. After examining descriptive statistics, internal consistency and confirmatory factor analysis, the authors found that the BPOES appeared to have adequate face and factorial validity. Paxton et al. noted that the ability to measure an increase in perceived youth empowerment that is the result of wellplanned, implemented and evaluated interventions is beneficial to future practice and research in health promotion and positive youth development [33]. The PI received verbal and written permission from the author to use the BPOES for this study.
3. Results
3.1 Sample
The final sample consisted of seven adolescent participants. Results of a Demographic survey are included in Table 1 which describes participant characteristics. There were two male participants and five female participants. Ages of participants ranges from 11 to 17. Initially, the desired age group for participants was 12 to 14 years of age because the literature suggested that age range tended to be when depression first occurs. Due to a lack of participants, the age parameters were increased to 11 to 18 years of age.

3.2 Data analysis
Thematic content analysis of individual interview data: Coding of interview data was the first step in data analysis. Digital audio recordings, text interview transcripts, and photographs were imported into NVivo 9 for data management, coding, and analysis. Transcripts of participant interviews were analyzed iteratively for thematic content and categorized by levels of the Social-Ecological Model (see Supplementary 1). Photovoice is not a method that analyzes visual data intensively [34] and therefore coding focused on text transcripts. Content analysis through focused coding was performed by the PI by reviewing all interview text transcripts three times to refine key reoccurring content elements. Text was separated into short paragraphlength units to code and linked with corresponding images and audio recordings simultaneously in NVivo 9. Re-occuring elements were coded by node (ie. dogs, cats and other animals were re-occuring elements that were coded under the node “Pets”). Nodes were then categorized as either risk or protective factors. Risk and protective factors were then categorized by ecological level and theme. Some themes and protective or risk factors were categorized in more than one ecological level. There was a total of ten thematic categories that were identified: activity, sensitivity, creativity, spirituality, comicality, cruelty, security, responsibility, facility, and morbidity and mortality. Collectively, protective factors (N=45) at all ecological levels represented coping strategies that provided ways of escape and risk factors represented things that hindered escape. There were a smaller number of identified perceived risk factors (N=23) for depression compared to protective factors.
Risk and Protective factors were categorized by social ecological level (Table 2). Factors categorized at each of the levels were analyzed and grouped by theme. Themes were identified by the primary investigator. Study rigor is addressed in Supplementary 2.

3.3 Social-ecological levels
3.3.1 Intrapersonal ecological level
The first level of the Social Ecological Model is the Intrapersonal Ecological Level. The Intrapersonal level refers to characteristics of an individual that influence their health behaviors such as selfconcept, attitudes, skills, intentions, and developmental history [35]. Thirty protective factors and nine risk factors were identified by focused coding and categorized by the PI at this level. These factors were then categorized by the PI into one or more of the following themes: activity, sensitivity, creativity, spirituality or comicality. The PI interpreted the identified protective factors to beindividual ways that participants perceived they could escape or cope with depressive symptoms. The PI interpreted identified risk factors to be things that an individual could do that would worsen depression.
For example, creativity through writing, drawing, and painting was perceived as a way to process through depressive episodes. As one fourteen year-old female explained, “It’s easier for me to process with something to help me than without it”. Creativity through writing and drawing was perceived as a more acceptable way to deal with depression instead of “drugs, alcohol, cutting or suicide”. A sense of humor was perceived as protective. The sensation of happiness, relief, comfort, love and expressing feelings were identified as protective factors categorized under the theme of Sensitivity. Feeling alone, sad, confined and afraid were intrapersonal risk factors categorized under the theme of Sensitivity. Feeling close to God, praying, being in the light, reading the Bible, seeking spiritual guidance, having faith, and having purpose were identified intrapersonal protective factors categorized under the theme of Spirituality. Not seeking a higher power was a risk factor that was categorized by the theme of Spirituality.
3.3.2 Interpersonal ecological level
The Interpersonal level of the Social-Ecological model is described by McLeroy et al. as the social relationships with family, friends, neighbors, work contacts and acquaintances that influence healthrelated behaviors [35]. Participants identified eleven protective factors at this ecological level that were categorized by the themes of security, sensitivity, and responsibility. Nine risk factors identified at this ecological level were categorized by the themes of activity, cruelty, sensitivity, and morbidity and mortality. Animals, stuffed and alive, were the most commonly referenced protective factor. Sheep, roosters, chicks, chickens, pigeons, cats, dogs, cows, rabbits, ducks, geese, penguins, and bears were photographed. Animals were seen as dependent, giving people a sense of purpose and responsibility, comforting, humorous, joyful and protective. House pets offered relief. For example, “My dog will lick my face. It usually will make me laugh or smile or something, so it’s kind of a relief from the sadness or depression that I feel at that moment and it takes my mind away from it for a while”. One fifteen year-old female suggested that “giving people a sense of responsibility over someone might help them feel better and might focus them on someone else instead of always focusing on how bad they feel”.
The protective factor of getting attention stemmed from analysis of text related to the importance of giving attention to or getting attention from someone or something. Acceptance was perceived as a protective factor supported by statements alluding to allowing adolescents to “be themselves”. Having friends was perceived as an indispensable protective factor at the interpersonal social ecological level.
3.3.3 Institutional/organizational ecological level
The Institutional or Organizational level of the Social Ecological Model directs attention to organizational or institutional factors that may affect adolescent depression positively or negatively. Examples of organizations include schools, work settings, neighborhood and professional associations, and agencies and corporations. Analysis of interview data identified two protective factors that were categorized by the theme of facility. Facilitation of preventive education and access to technology were perceived as protective factors against depression. A fourteen year-old female suggested her community offer selfdefense classes to increase citizen awareness of violence and offer ways to protect themselves. Television, phone and internet services provided through corporate communication providers were also perceived as protective factors.
Two risk factors were identified at the institutional/organizational level and were categorized by the theme of activity. These two factors included living in a small town and attending a school where the principal and teachers were unreasonable. Stressors related to school requirements and grades were perceived as risk factors for depression as were poor relationships with teachers. Participants were asked not to take photographs on their school grounds to reduce the possibility for bullying. Therefore, no photographs were identified for this level.
3.3.4 Community ecological level
The Community ecological level refers to mediating structures such as family, informal social networks, churches, voluntary associations, neighborhoods and the relationships between them [35]. Two protective factors categorized by the theme of activity were identified at the community ecological level. These two factors were community recognition of adolescent depression and living in a neighborhood. One fifteen year-old male suggested the protective factor of “humor” could be addressed at the community level by the development of “a community comedy club”. An eleven year-old male shared that the love of God experienced through church activities would be supportive.
Three risk factors were categorized at the community ecological level and identified thematically as activity. These three factors included living in a small town, living near danger, and living in a small town where there aren’t enough churches. Small town characteristics of low socio-economic level, lack of church and recreational facilities, and lack of shopping alternatives were perceived as risk factors for depression. One participant talked about the murder of a homeless person near the railroad tracks in her neighborhood; the episode made her acutely aware of potential danger in her community.
Community-related questions at the end of the SHOWed interview addressed ways the community could respond to the mental health needs of local teens. Participants were asked the following questions:
1) How does this photo relate to your life as an adolescent who has
experienced depression?
2) What has your community done or not done about the risk and
protective factors that you identified?
3) What would you like your community to do about the risk and
protective factors that you identified?
4) What can we do to educate other people in your community about
the issues you identified?
A fifteen year-old male who saw responsibility as a protective factor responded that communities should make it easier for people to acquire animals in order to learn responsibility. He stated, “Responsibility is one of the things people need in this town.” A female participant suggested her community be more willing to help people, allow them to be who they are, and be less critical of their beliefs. Another female who liked to walk with her friends thought that her community did a good job of providing parks and areas for walking, but she felt her community should provide more education about bullying. Providing transportation to church was suggested as a community need by an eleven year-old boy. He also wanted his community to stop bullying and put up surveillance cameras and microphones in restrooms at school so bullying would be caught. He also suggested the community “make it a law where your family actually does love you.” Education related to substance abuse was needed according to a fourteen yearold female; she also felt more opportunities for writing and drawing were needed in order to use them as coping strategies. One female who was particularly adept at the arts suggested keeping chorus, band, and art as outlets at school and that the community should be more aware of the signs and symptoms of depression, such as cutting.
3.3.5 Public policy ecological level
The Public Policy level addresses factors related to local, state and national laws and policies. There were no risks or protective factors or themes identified at this level.
3.3.6 Perceived risk and protective factors by ecological level
Overall, a greater number of protective factors (N=45) than risk factors (N=23) were identified. The majority of these factors occurred at the intrapersonal and interpersonal ecological level areas. At the intrapersonal ecological level, 30 protective factors and 9 risk factors were identified. At the interpersonal ecological level, eleven protective factors and 9 risk factors were identified. An equal number of protective factors (2) were identified at the institutional and community ecological levels. Two risk factors were identified at the institutional ecological level and three were identified at the community level. As stated above, there were no protective or risk factors identified at the public policy ecological level.
Examples of participant photographs that triggered dialogue about protective and risk factors at each level can be viewed in Supplementary 3.
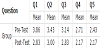
3.4 Brief perceived opportunity for empowerment scale (BPOES)
The Brief Perceived Opportunity for Empowerment Scale (BPOES) was administered prior to the first training session and after the individual interview. All seven participants completed the pre-test and six participants completed the post-test. The Pearsons’s Chi Square Test of Association results were not statistically significant. Although there was no statistical significance between the pre- and post-test scale by the Chi Square analysis, the general trend of changes in pre- and post-test means by group and question was interpreted as demonstrating a trend toward an increase in empowerment (Table 3). Lower post- test means were interpreted as participants tended to agree more with the BPOES question after participation in the study. The assigned point format was as follows: 1) strongly agree, 2) agree, 3) not sure, 4) disagree, and 5) strongly disagree.
3.5 Dissemination of findings
An Open House for the first photograph exhibit was held at a community arts center in the youth art gallery. The show was publicized on the center’s website. Formal invitations were sent to local politicians, mental health care providers, and board members. The Opening night drew over 50 attendees. Attendees included a mayor and his wife, mental health care providers, university faculty, general public and participants’ families (Figure 1). Supplementary 4 contains examples of comments written in the guest book by attendees about the photograph exhibits.

4. Discussion
4.1 Method
While there is a substantial body of literature that has used Photovoice with youth around the globe [15,23,26, 36-44], there is a lack of studies that specifically use a social ecological model with the method. In addition, there is a lack of Photovoice studies that address mental health issues with rural youth, in particular those who are diagnosed with depression. This study contributes to this gap in the literature through its use of the unique method of Photovoice while looking through the lens of a social ecological context with a vulnerable population of depressed youth.
Findings from this study indicated a positive response to participation in Photovoice by the adolescents. They seemed to accept and embrace an opportunity such as this to share their perspectives related to their lived experiences. Photovoice as a method was adaptable to their cognitive and developmental levels and to their context and environment, which enhanced its acceptability by the youth. Photovoice was also found to be a viable Community Based Participatory Research (CBPR) method with rural depressed adolescents. Consistent with the principles of CBPR, adolescents and their parents were engaged as partners as much as possible in this study throughout the research process. Through public exhibit of photographs, participants built upon existing community knowledge of the lived experience of rural adolescents who live with a diagnosis of depression.
4.2 Risk and protective factors
Study findings revealed a greater number of protective than risk factors and most of the protective factors occurred at the intrapersonal and interpersonal ecological levels of the Social Ecological Model. One must acknowledge that numbers do not necessarily indicate relative strength of a protective or risk factor. However, it is encouraging that participants identified a greater number of protective than risk factors for depression. As one participant stated, “A good thing about being in this study was that it showed me I had a lot more protective factors than triggers for my depression”.
In general, perceived protective factors by participants in this study were identified as tangible active coping strategies that offered ways to escape from depression... ie. taking a walk, exercising, being with friends, listening to music, drawing, and writing. Perceived risk factors were less tangible and more inescapable…ie. the weather, a small town, death, living in this world, school, authority, and danger. Adolescents are at a transitional stage in which they are still shifting cognitively from concrete to abstract thinking. This may explain why tangible concrete coping strategies of doing something or being involved in some type of activity were perceived as more protective. Differences in abstract and critical thinking skills and photography abilities were apparent among participants whose ages ranged from 11 to 17 years. For example, protective factors shared by an 11 yearold male included church, family, and pets. He reported risk factors of bullying and loss of pets. He took a total of seven photographs. In contrast, protective factors shared by a 17 year-old female who took over 200 photos included reading, painting, and exercising. The older participants shared protective and risk factors that encompassed a greater number of ecological levels. This emphasizes the importance of considering the cognitive developmental stage of participants when partnering with adolescents and planning interventions.
Intrapersonal factors such as the developmental history of the individual can influence health behaviors [35]. Adolescents are in the process of transitioning out of an egocentric self and are still dependent upon adults. Consequently, their perceptions are more likely to align with intrapersonal and interpersonal levels. It would behoove those who design interventions for this particular population to consider the identified risk and protective factors that were identified so that those interventions will be more acceptable to the adolescents. Interpersonal interventions should address social relationships and influences that foster unhealthy behavior [35]. Parents/guardians can provide opportunities for these youth that aim at addressing identified risk factors and enhancing protective factors at intrapersonal and interpersonal ecological levels. Decreasing a depressed adolescent’s exposure to unhealthy groups and social influences will decrease opportunity for risk factors to cultivate [35]. Parents/guardians interventions are needed to deter identified risk factors at all levels and promote protective coping activities attesting to the importance of parent/guardian participation and support. At the intrapersonal ecological level, spirituality was identified as an important protective factor for depression. Yet at the community ecological level, a lack of churches was noted as a risk factor. Perhaps support of mental health promotion activities for youth may be a promising option for the rural church community.
Protective and risk factors identified at the institutional organizational, community and public policy levels were minimal. Adolescents do not vote on public policy and are generally not yet active in their community at organizational or political levels. Photovoice projects may be able to instill early recognition of the importance of public policy, citizenship and social action in the participant. Policymakers must participate in the Photovoice process if social change is desired. If policymakers are to make a persuasive argument for change, they need clearly documented data to make things happen [10]. Policymaker involvement in the entire Photovoice/ CBPR process will expose them to study findings and dissemination activities. Policy change takes time, which may make it difficult to demonstrate outcomes and impact of a Photovoice project within a projected timetable [33] but this can be a goal of future studies.
4.3 Empowerment
Use of the Brief Perceived Opportunity Empowerment Scale (BPOES) in previous studies to evaluate empowerment as a result of participation in Photovoice studies was not found in the literature. Increased individual empowerment was identified as an outcome by Catalani et al. in their review of 37 Photovoice articles [11]. In this study, results of the Brief Perceived Opportunity for Empowerment Scale (BPOES) revealed a trend toward a positive change in empowerment. Measuring increased empowerment resulting from well-planned interventions is useful for future practice and research in promoting youth health and development [33]. Participating in a Photovoice project that empowers may strengthen adolescents as they learn to accept and meet the demands of a mental health diagnosis.
4.4 Risks
There are risks when using Photovoice as a method in a CBPR capacity [45]. Photovoice has the potential to create the negative outcome of raising hopes but then failing to inform policy or rally public concern, which could cause feelings of hopelessness and lack of empowerment [12]. In this study, participants were informed of the potential for lack of community action at the initial training session and in the consent process. When working with participants with a diagnosis of depression, sensitivity to the psychological repercussions of identifying and discussing issues that makes depression worse is warranted [12].
Another issue may be participant attrition. Youths need encouragement to complete project activities [12]. Life challenges such as competing school activities, health issues, and other demands may interfere with participation. Listening to adolescents share their concerns may help deter attrition [29]. The researcher should also be aware that provision of guidance needed by adolescent participants for a CBPR project is time consuming. Adolescent groups may not have the capacity to conduct CBPR without external help, and they may not be willing to allot the extra time needed toward building trust with the researcher [46,29].
4.5 Benefits
There can be potential positive outcomes that outweigh the risks for adolescents who participate in a Photovoice project. The experience offers a way for adolescents to take on the role of a competent citizen and active participant to enhance their community's well-being [29]. Empowerment experienced through a participatory method such as Photovoice may assist the adolescent to incorporate the diagnosis of depression into their identity in a healthy way [47]. Youths may realize that their thoughts and opinions really do matter [12]. Psychological empowerment may occur through building self-esteem and self-competence as the youths acquire photography skills [12]. Engagement of youths as researchers inspires a sense of responsibility and purpose in society which contributes to social competency [12]. Also, participation in a youth Photovoice project facilitates youth-adult partnerships and adults benefit from recognizing the contributions that youth can make to creating policies and programs that are relevant and appropriate [29].
4.6 Unexpected results
An unexpected result of the study was development and demonstration of camaraderie among parents and participants that spanned throughout the project. Parents became friends, supported the project together, and referred adolescents for participation who lived in their communities. Participants who did not know each other discovered they attended the same schools and became friends. Another unexpected result was local mental health providers requesting training so that they could initiate future Photovoice projects with their clients.
4.7 Recommendations
Continuing research efforts can lead to interventions that will decrease risks and strengthen protective factors prior to the onset of mental health disorders [48]. As a result of developmental and epidemiological research that identifies modifiable risk and protective factors, prevention approaches can be developed to change those factors to prevent the development of mental problems [48]. Prevention of mental disorders is possible when protective contexts are fortified and risk factors are decreased [48].
Replication of youth Photovoice studies is recommended to inform evidence-based data collection and analysis, as well as to establish the reliability and validity of findings. This in turn will provide support for the use of Photovoice as a beneficial participatory method to improve the health and well-being of adolescents. This Photovoice study served as a starting point for future CBPR efforts with depressed rural adolescents by initiating a relationship between the PI and community. Replication of the study and long-term evaluation of outcomes is needed. Findings of this Photovoice study imply that participants may have experienced empowerment. Evaluation of empowerment as an outcome is warranted. Evaluation of evidence of long-term community outcomes such as social and policy change is also needed. Continuing efforts to increase awareness of community agencies, stakeholders and policymakers are needed to influence decision-making related to creation and delivery of policies and interventions that address adolescent depression. In order to more effectively design and deliver interventions it would benefit mental health care providers, researchers, community stakeholders and policy makers to examine the identified perceived risk and protective factors resulting from this study. It is important to understand an adolescent’s perceptions of the ecological factors that influence their health because it guides development of evidence-based prevention and early intervention strategies to reduce mental health problems [49,18]. Particular attention should be paid to the social ecological levels at which the factors occur so that interventions can be directed accurately at the protective and risk factors that occur at those levels.
5. Conclusion
Using Photovoice as a Community-Based Participatory Research(CBPR) method with depressed rural adolescents to identify risk and protective factors for their depression is an innovative and unique way for qualitative researchers to gain access to an adolescent’s lived experience. The Photovoice method demonstrates consistency with the CBPR process in that the research plan, data collection, project implementation, data analysis and interpretation, and dissemination of findings are inherent in the Photovoice process. CBPR allows the researcher to approach the topic of interest with a comprehensive viewpoint to address multiple social ecological factors that influence health outcomes. Using a social ecological framework fosters consideration and organization of factors in an adolescent’s environment that influence their depression from multiple perspectives. The importance of new approaches that apply Social-Ecological Theory to mental health care is emphasized by our present healthcare system that focuses efforts on the individual or family unit but does not address other environmental influences [50]. Health disparities will remain until social structures such as community, organization, and political systems are viewed as the primary site of intervention by nursing research and practice and our mental healthcare system [50]. To have the most positive impact on adolescent health, multiple systems such as government agencies, community organizations, schools, and community members must work together in a comprehensive approach [51]. Researchers and communities need to recognize that adolescents can contribute to community assessment, activism and empowerment endeavors through participation in Photovoice [20] and Community-based research. The results of Photovoice projects with adolescents with mental health disorders can be used to raise community awareness of the nature of their problems and guide the selection of programs most relevant to community needs [52]. Mental health practitioners as well as parents can use this information to design and implement relevant preventive actions before problems occur [52]. Community leaders can assess community risk and protective factors associated with depression in adolescents to best target preventive services [52]. Educators can address risks associated with onset of depression early before the child or adolescent reaches the point of greatest risk on their developmental trajectory [52]. Constructing interventions that are fitting to social ecological level and address risk and protective factors identified by adolescents who have experienced depression will hopefully improve their future mental health outcomes and chances for a successful adulthood.
Competing Interests
The author declares that she has no competing interests.
Author Contributions
Julia Dempsey
1. Conception and design, team training, analysis, interpretation of
data and funding acquisition
2. Involvement in drafting the manuscript and revising it critically
for important intellectual content
3. Final approval of the version
Acknowledgments
With special recognition of the contributions of the seven adolescents who participated in this study.