


1. Introduction
1.1 Significance and Justification
Congestive heart failure (CHF) or heart failure (HF) is a chronic, complex disease that places a significant global burden on health care. Heart failure is a syndrome comprised of symptoms such as dyspnea, edema, and effort intolerance, and clinical signs such as elevated jugular venous pressure, pulmonary crackles and apical displacement, secondary to an abnormality in cardiac structure or function [1]. Patients with heart failure are challenged by threats to their quality of life and face significant morbidity and mortality.
In Canada, heart failure affects approximately 500,000 Canadians with 50,000 new patients diagnosed each year [2]. The impact of heart failure on health care economics is staggering. In developed countries, heart failure accounts for approximately two percent of expenditures and in the United States the costs associated with heart failure hospitalizations reached an estimated $20.1 billion dollars in 2009 [3]. It is projected that in the United States, by the year 2030, the total cost of heart failure to the health care system will reach $70 billion dollars [4].
Patients with HF challenge the health care system with their frequent admissions, often resulting in increased length of stay (LOS) and conservable days due to their complex management needs, and frequent readmissions. Costs associated with the management of CHF are an ongoing challenge. Strategies must be utilized that balance quality, patient care with fiscal accountability and responsiveness from an organization perspective.
At a two site hospital corporation in Ontario, Canada, CHF is one of the top admission diagnoses and one of the leading outliers in terms of LOS and conservable days. Conservable days has been defined by the Institute for Clinical Evaluation Sciences (ICES) as "the number of days that might be conserved if a hospital decreased the adjusted average length of stay from existing levels to the benchmark levels" [5].
The hospital corporation is part of a Local Health Integration Network (LHIN) in Ontario, Canada. Local integrated health networks (LHINS) are not-for-profit organizations that are responsible for planning, integrating and funding health services in 14 different geographic areas of the province. The Ministry of Health and Long Term Care has granted legislative power and authority to the LHINS. The hospitals in this study are part of a LHIN that is geographically diverse and serves the population of urban cities, rural farming communities, and remote settlements. Regardless of the hospital size in this LHIN, heart failure, along with chronic obstructive lung disease (COPD), and pneumonia have been designated as the diagnoses that consistently do not meet the targeted LOS and therefore contribute to a significant increase in conservable days and subsequent cost escalation in Ontario hospitals. Under direction of the LHIN, all hospitals within it have been mandated to implement clinical pathways for these three diagnoses in an attempt to standardize and coordinate care, and decrease hospital LOS.
Clinical pathways are an evidence based strategy to coordinate, standardize, and improve quality of care and health care efficiencies. Like pathways, standardized order sets are evidence based, provide similar benefits and decrease provider variability in care management for patients with selected diagnoses. Depending on the format of the clinical pathway and standardized order set, distinctions between the two may not always be clear as pathways may be viewed as a series of order sets [6]. The hospital sites in this study have a standardized order set with an order to initiate the CHF pathway embedded in it. As the literature suggests, there was confusion at the sites amongst the staff, and even some physicians, as to what the difference was.
The existing CHF pathway and order sets at the hospital sites were out dated and poorly utilized but still an expectation of heart failure care. For the fiscal year (April 1, 2012 to March 31, 2013) quarterly audits have demonstrated poor compliance in the use of CHF pathway and standardized CHF order sets. Utilization of the CHF pathway at one of the hospitals (Site 1) in the corporation ranges from 3% - 13%, with the range of standardized order sets usage at 24%-37%. Utilization of CHF pathway use at the second hospital site (Site 2) ranges from 27%-44% and the use of the CHF order set ranges from 23%-38%. These low utilization rates suggest that the majority of patients admitted with CHF may not have benefited from evidence based, standardized approach to care. Despite the fact that CHF is one of the leading admission diagnoses for the hospital corporation, of all the existing standardized order sets in the organization, the utilization of the CHF order set (which triggers the pathway) is not within the top five.
This mixed method study/ quality initiative was undertaken to review the utilization of CHF pathways and the standardized CHF order set in which it is contained, to determine a strategy to improve compliance with the goal of optimizing patient outcomes, improving quality of care, decreasing LOS and ultimately leveraging organization efficiencies for adult patients hospitalized with CHF.
1.2 Review of Literature
1.2.1 Search Strategy
A PICOT (Population or disease, Intervention or Interest, Comparison intervention, Outcome and Time) approach to formulate the study aim and a structured approach to the article appraisals as described by Melnyk & Fineout-Overholt (2011) was utilized [7]. Two search strategies were undertaken to find articles on clinical pathways in CHF. The first began with PubMed looking for relevant abstracts and citations. The next step involved a search of Ovid (Medline based). The customize search option was utilized and map term to subject heading option was chosen. A search made with the MeSH term critical pathways yielded 4137 results. A follow up search with the MeSH term heart failure yielded 77,863 results. The results of both searches were combined with a result of 102 articles (N = 102). Additional parameters added to the searches included English, adults, meta-analysis, randomized control trials, control trials, and systematic reviews, yielding nine articles (n = 9).
The second search strategy accessed the following computerized data bases from the years 2006-2012: EMBASE, CINAHL, PROQUEST, SCIENCE DIRECT, GOOGLE SCHOLAR, and ACADEMIC SEARCH COMPLETE. Search terms utilized were congestive heart failure, heart failure, adult, clinical pathways, critical pathways, and length of stay. Scholarly articles were requested. No editorials or book reviews were included. Although clinical pathway, CHF or heart failure individually yielded significant numbers, there was a paucity of articles that dealt with a clinical pathway in heart failure (HF). There was no additional yield resulting from this search. Of note, there were findings of pathways in heart failure from 1995- 2002 but these were excluded due to the predetermined criteria to search within a six year time frame to find the most current literature. Perhaps this earlier time frame is when literature, studies and trials resulting from the introduction and progression of clinical pathways were coming to fruition. This finding is supported by Kul et al, [8]. In their systematic review of in-hospital heart failure care pathways, they found no eligible study until 1999 and it is hypothesized that the benefits of clinical pathways, specifically to heart failure, is unclear or perhaps not fully investigated.
After excluding articles that did not include heart failure specific pathways, were based on end of life heart failure strategies, or did not meet the aforementioned parameters, only seven articles were found. The search was expanded to ten years (2002-2012) and included digital dissertations to facilitate a more comprehensive data base. Only one additional article that met the criteria was found. Although this review’s focus is hospital based LOS, an article on an outpatient heart failure pathway was included as patients were referred, in part, from a hospital setting and the pathway was heart failure specific. After evaluating the results of the search strategies and determining the articles suitability for inclusion, eight articles (n = 8) were accepted for review [8-15].
Although the included studies span an almost ten year time frame, the outcome variables remained consistent. This suggested that there is some consensus as to what HF pathways need to achieve to support the efficacy of health care, positive patient outcomes and decreased LOS. Length of stay was the most consistently reported variable. Of the studies reporting this outcome, none reported increased LOS but two reported no significant difference between treatment and control groups [9,10]. The remaining studies determined that clinical pathway use correlated with reduced LOS [11-13].
1.3 Theoretical Framework
Mishel’s Theory of Uncertainty in Illness was the framework chosen for this project.
Mishel’s theory consists of an original theory and a reconceptualized theory. In the original theory, patients in the diagnosis or treatment stage of an acute illness, had the desired outcome of returning to the previous state of health. For patients with chronic illness, the original theory did not produce consistent findings. As a result, the reconceptualized theory evolved to address the challenges of living with uncertainty in chronic disease states or in illness with the possibility of recurrence. The chaos theory was used to revise the original theory with the proposal that prolonged uncertainty can be the catalyst for a change in perspective on life and illness. In contrast to the desired outcome of a return to previous health in the original theory, the desired outcome in the reconceptualized theory is personal growth that results in the evolution of a new value system [16]. For patients with CHF, Mishel’s reconceptualized theory is particularly relevant. The treatment of CHF involves medication, dietary, and exercise regimes that may be vastly different from the pre-diagnosis state. Lifestyle changes with the goal of symptom management and stabilization often require the reprioritization of personal habits and activities. What was valued in the past may require revision if compliance with the treatment plan is to be obtained. The significant morbidity and mortality of CHF supports the need for vigilance and change if quality of life is to be achieved and maintained.
2. Materials and Methods
2.1 Statement of purpose
This mixed method study/quality initiative was undertaken to review CHF pathway use and determine if heart failure pathways decrease LOS, conservable days and leverage organization efficiencies for adult patients hospitalized with CHF.
2.2 Human rights protection
The study utilized both primary data collection and secondary data analysis. Full approval was received from the D’Youville College (DYC) Institutional Review Board (IRB) to conduct the research. Subsequent to this, approval was sought and received from the participating hospital corporation. This study does not involve patient contact and there are no patient identifiers on the data presented in this project. Staff participating in the survey did so on a voluntary basis and understood that the survey results would remain confidential.
2.3 Study Objectives
- To review current literature regarding the effectiveness of congestive heart failure (CHF) pathways and standardized order sets.
- To determine physician, nurse practitioner, and nursing staff barriers to the use of existing CHF pathways and order sets and correlate relationship between awareness of existing CHF pathways and utilization by site.
- To conduct a secondary data analysis of patients with CHF admitted to a two site hospital corporation in Ontario, Canada for fiscal year 2012-2013. Data analysis will consist of: a) site specific chart audits of CHF admissions to assess the percentage of compliance with utilization of CHF pathway and standardized order sets b) report descriptive statistics of site specific CHF admission variables including: Age, LOS-as acute and alternative level of care (ALC), expected length of stay (ELOS), and conservable days attached to each admission.
- To determine correlation between CHF pathway and standardized order set usage and average conservable days for each site.
- To revise existing CHF pathway and order sets based on current evidence for standardization of care.
- To promote and support the consistent use of the CHF pathway and standardized order set in an effort to improve quality of care, decrease LOS and improve organization efficiencies.
2.4 Definition of Terms
The following terms were either conceptually or operationally
defined here:
Conservable days: Conservable days has been defined by the Institute
for Clinical Evaluation Sciences (ICES) as "the number of days that
might be conserved if a hospital decreased the adjusted average length
of stay from existing levels to the benchmark levels" [2].
Cost per weighted case: It is an indicator that measures the cost associated with caring for a standard, acute hospital patient. A weighted case is one that is assigned a resource intensity weight.
Expected Length of Stay (ELOS): It is the expected length of stay for a patient with a specific diagnosis. It accounts for the variables of age and co-morbidities in the calculation.
Resource Intensity Weight (RIW): It is the average cost for patients staying the average length of stay (LOS) that is measured against the national benchmark. A typical case of any acute inpatient admission in Canada is assigned an RIW of 1. Therefore an RIW of 1.22 means this patient had 22% more expense to their LOS than the average typical inpatient in Canada. The RIW is consistent until the patient stays past the expected length of stay (ELOS). At this point the RIW is increased. Dividing the average RIW by the average LOS gives the cost per day. This equates to the cost of a conservable day. Comorbidity adds 25% to the total cost.
Trim point: The trim point is the LOS that identifies a long stay outlier. Approximately 4% of patients in Canada are outliers. Once a patient is an outlier, than the RIW changes for each additional day of stay. In essence, the Canadian Institute of Health Information (CIHI) calculates the cost per day for conservable days once they go beyond the trim point. This is meant to be cost neutral to allow the hospital to continue to care for the patient.
Definitions provided are those utilized by performance evaluation specialists at the study sites
2.5 Setting
A two site hospital organization in Ontario, Canada, was chosen to examine CHF patient outcomes. This organization was chosen, in part, because CHF (along with Chronic Obstructive Pulmonary Disease) accounts for approximately 20% of all hospital admissions. Further, CHF patients are identified as a cohort of adult hospitalized patients that frequently exceed the ELOS thus resulting in the accumulation of conservable days and subsequent increased care costs.
2.6 Population and Sample
The population is all hospitals treating all health conditions. The sample of interest is a two hospital site in Ontario, Canada and CHF patients admitted via the two Emergency Departments (ED). Three separate data sets from each hospital are utilized in this project. The first two data sets were provided by the manager of quality improvement and the director of performance evaluation specialists. Specifically, the first data set detailed systematic quarterly chart audits, conducted over the fiscal year April 1, 2012 to March 31, 2013, documenting use of the CHF pathway and standardized CHF order sets. The second data set, covering the same fiscal year, detailed specific CHF admission variables for patients admitted with this diagnosis. The last data set was a survey of clinicians at the two hospitals assessing knowledge and use of the CHF pathway. Given the use of primary and secondary data, this study is a quality initiative utilizing a mixed methods research design investigating the association between CHF pathways and LOS.
2.7 Data collection methods
The data set supplied by the manager of quality improvement consisted of regularly scheduled quarterly audits on CHF pathway/ order set use that is utilized by the organization to assess compliance with practice standards and expectations, identify areas for improvement, and support decision making. The data set provided by the director of performance evaluation specialists was admission and discharge information for the fiscal year in question and contained patient demographics (i.e. age, sex), as well as LOS, ELOS, RIW and conservable days. The data was delivered electronically in Excel.
The survey utilized was developed by the researcher. Prior to implementation, a small pilot survey was administered to five emergency department staff to assess readability, comprehension, and ability to complete. All five participants reported no issues with comprehension, intent, or challenges with completion. These five staff hold nursing and support positions and were not involved in the administration of the final survey.
Information regarding the study was provided via an e-mail communication prior to the surveys being distributed. In addition, an information sheet regarding the intent of the study was attached to each survey for review prior to completion, to facilitate the decision to participate.
Fifty surveys were distributed, via convenience sampling, to Site 1 and Site 2. Specific clinical staff primarily affiliated with the treatment of CHF patients in the EDs were recruited including physicians (ED and internal medicine), nurse practitioners (NPs), registered nurses (RNs), and registered practical nurses (RPNs).
2.8 Tool
The survey assessing knowledge and use of the CHF pathway comprised five primary questions and six follow up questions depending on the response to question number five. Specifically, respondents who provided a No response to “Use the pathway regularly”, were prompted to report the reasons for not utilizing the pathway. Question one asked the participant’s occupation. Question two asked for the respondents primary practice area. Question three asked if the respondent was aware of the CHF pathway to be used for CHF admissions. If the answer was No, the survey was to be returned. Question four was have you ever used the CHF pathway? Question 5 was a Yes/No question- Do you use the pathway regularly to treat CHF patients? If the answer was No, the follow up was to check all that applied from the following: a) I am not familiar with how the pathway works, b) I don’t know where to find the pathway, c) Pathway use is too time consuming, d) Lack of clerical support to provide computer entry of pathway requirements, e) I don’t think pathway/standardized order sets impact patient outcomes, and f) MD/NP only- I prefer to write my own orders.
2.9 Treatment of data
The two data sets supplied by the quality management and performance evaluation departments were utilized in the following manner. Frequency of CHF pathway and order set use was calculated from the data set detailing chart audits; all calculations were performed directly in the originating Excel data set (Microsoft, 2010). The CHF patient data set was imported into SPSS, Version 22 (IMB Corp) and all calculations were performed within SPSS. The primary survey data was initially entered into Microsoft Excel and, following entry, imported into SPSS, Version 22 (IMB Corp), where all calculations were performed. The study design was strengthened through the mixed methods design that included the utilization of two secondary data sources and collection of primary data. The results are presented in both descriptive and inferential statistics.
3. Results
3.1 CHF admission/discharge data
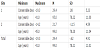
The number of CHF admissions for the two sites reviewed in this study totaled 500 patients. Site 1 produced 216 of these admissions, in comparison to 284 admissions at Site 2. The average age at Site 1 (M = 78.22, SD = 11.00) was nearly identical with the average age at Site 2 (M =78.20, SD = 11.04). Site 1 had a slightly smaller male to female ratio of admissions (1:1.08 respectively), than Site 2 which demonstrated a larger female to male ratio (1:1.31 respectively).
Site 2, despite having more admissions, accumulated less conservable days (M = - 1.15, SD = 4.9) than Site 1 (M = 0.08, SD = 5.23). The negative value is an indication that the patients actual LOS was less than the ELOS assigned to the admission. The observed discrepancy was, in part, attributable to the increased LOS at Site 1 (M = 10.05 days, SD = 9.32 days) compared with Site 2 (M = 7.73 days, SD = 11.03). In order to contain costs and avoid financial penalty, the goal is to limit the number of conservable days.
At both sites, CHF patients within the age group of 60-79 years accumulated the most conservable days (Site 1, 222 conservable days, Site 2, 183.6 conservable days). Table 1 displays summary statistics for age and conservable days.
3.2 Chart audits
The results of the quarterly audits on admitted patients with a CHF diagnosis were significantly different between sites. These audits are undertaken to assess compliance with the use of diagnosis specific order sets and pathways. In the absence of the utilization of the standardized CHF admission order set, the general medicine admission order set, or a free text sheet may be utilized. Site 2 outperformed Site 1 in both CHF pathway and standardized order set use. Site 1 utilization of the CHF pathway varied from 3% - 13% across the four quarters for fiscal year April 2, 2012, to March 31, 2013 while utilization of the CHF order set varied from 20% - 37% in the same time period. In contrast, Site 2 utilized the CHF pathway on 27% -44% of the audited charts and utilized the CHF order set on 23%- 38% of cases. Table 2 displays the site specific audit result for CHF admissions for the fiscal year.
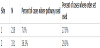
Overall, Site 1 only utilized the CHF pathway in 7% of audited cases, while Site 2 utilized the pathway in 36.3% of audited cases (see Table 3). Of note is that the order to implement the CHF pathway is embedded within the standardized order set, and although the CHF pathway can be implemented independently, the CHF standardized order set utilization, should be relatively equivalent to the CHF pathway use.
3.3 Survey
A total of 50 surveys were distributed to each site. The response rate for Site 1 was 82 % and 100% for Site 2. Nine of the 50 surveys for Site 1 were not completed and two further surveys were excluded from analysis due to errors in completion. Five surveys from Site 2 were excluded from analysis due to errors in data completion. Therefore, all subsequent analyses were conducted on 39 surveys for Site 1 and 45 surveys for Site 2.
Site 2 respondents reported a greater awareness (86 %, n = 37) of the CHF pathway than Site 1 respondents (77.8%, n = 28). Although a larger percentage of Site 1 respondent reported having ever used the pathway (85.7%, n = 24) compared with Site 2 (67.6%, n = 25), Site 2 respondents reported a higher frequency of using the pathway regularly (54.1%, n = 20) compared with Site 1 (21.4%, n = 6).
3.4 Analysis
All analyses were conducted with SPSS, Version 22 (IBM Corp).
Pearson’s chi-square was performed to test whether survey questions 3, 4, and 5 were significantly different between Site 1 and Site 2. A significant chi-square value, denoted by p < .05, indicates the responses to the survey question were significantly different between the two sites. Whereas a non-significant chi-square value, p > .05, indicates the responses were not significantly different.
Responses to survey question 3 (aware of CHF pathway) were not significantly different between the two sites, χ2 (1) = .92, p = .338. Responses to whether the clinician had ever used the CHF pathway (question 4) were not significantly different between the two sites, χ2 (1) = 2.83, p = .093. The difference in responses to survey question 5 (use CHF pathway regularly) were statistically significantly between the two sites, χ2 (1) = 7.07, p = .008, with 54.1% of Site 2 respondents indicating yes compared with 21.4% of Site 1 respondents.
The difference in site variation to the response to question 5 (use CHF pathway regularly), resulted in the performance of additional analyses. Separate tests of analysis of variance (ANOVA) were calculated for age, ELOS, and LOS to determine significant differences between the two sites. Age, along with co-morbidities, is factored into the calculation of the ELOS for any admission. In addition, a chisquare test was performed on the composition of sexes between the sites.
The first ANOVA revealed no significant differences in age between the two sites, F (1, 498) = .000, p = .986. The ELOS was not significantly different between the two sites, F (1, 498) = 2.77, p = .096. The actual LOS was significantly different between the two sites, F (1, 498) = 6.20, p = .013, with the average LOS at Site 1 ( M = 10.05 days, SD = 9.32 days) greater than Site 2 ( M = 7.73 days, SD = 11.03
The chi-square test for differences in total number of men and women approached the conventional level of significance for differences between Site 1 and Site 2, χ2(1) = 3.59, p = .058. Site 1contained a greater percentage of men (51.9%) than Site 2 (43.3%); although, Site 2 reported a greater percentage of women (56.7%) than Site 1 (48.1%).
Given the significant differences between actual LOS between sites, an additional test for significant differences in conservable days between Site 1 and Site 2 was performed. Conservable days represent the difference between the actual lengths of stay in comparison to the benchmark (i.e. ELOS).
Specifically, an ANOVA was performed with site as the independent variable and conservable days as the dependent variable. The ANOVA revealed a significant difference between sites, F (1, 498) = 7.78, p = .006, with Site 2 reporting a statistically significant decreased mean number of conservable days ( M = -1.15, SD = 4.59) compared with Site 1 ( M = .08, SD = 5.23).
3.5 Cost of conservable days
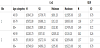
Although Site 2 had less conservable days than Site 1, the number of conservable days for both is significant and therefore costly to the organization. The mean cost per conservable day varied across the three age groups. The cost per conservable day is calculated by taking the cost per weighted case multiplied by the average resource intensity weight (RIW). For patients within the age range 18 to 59 year old, the average cost per conservable day was estimated at $1114.00. For patients 60 to 79 years old, the cost of a conservable day was estimated at $1044.00. This group accounts for the greatest number of conservable days at both sites. Patients 80 years and older had an estimated conservable day cost of $1028.00. The overall average cost for Site 1 ( M = $4676.99, SD = $5034.29) exceeded the overall average cost for Site 2 ( M = $4214.10, SD = $4614.13). Based on the actual reported conservable days, the cost for the total conservable days for Site 1 is estimated at $420, 953, while the cost for Site 2 conservable days is estimated at $249,770, for a total corporate cost of $770,724. Table 3 details the overall conservable day cost and RIW by site for each of the three age groups.
4. Discussion
The study objectives were either met or partially met. A literature review showed some evidence (although limited) that the use of CHF pathways can decrease LOS but a decrease in CHF costs with pathway use was not supported.
Barriers to the use of CHF pathway and order sets were identified. At both sites, the most common responses for not using the pathway regularly was the belief that pathway use is too time consuming (Site 1 - 47.2%, n = 17, Site 2 – 16.3%, n = 7). Site 1 had a greater number of respondents who did not believe that CHF pathway use impacts outcomes (27.8%, n = 10) compared to Site 2 (2.3%, n = 1). The regular use of CHF pathway use at Site 2 correlated with a decreased number of conservable days, despite a greater number of CHF admissions.
Secondary data analysis found that Site 1 had more male patients than female while the reverse was true at Site 2. There was an association (not correlation) between CHF pathway and standardized order set use and conservable days. As correlation is a measure of association between two variables, the choice of the word “correlation” in objective four, was in retrospect, incorrect. Site 2, which scored higher on chart audits for usage of the pathway and order set, also had a decreased number of total conservable days.
Several outcomes of support are presented here to provide evidence of the association between CHF pathway use and LOS. Chart audits from both sites indicate that Site 2 used the CHF pathway over 29 percent (29.3%) more than Site 1 utilized the pathway. Specifically, Site 1 used the pathway, on average, 7% of the time whereas Site 2 used the pathway, on average, 36.3% of the time. The outcomes of the chart audits were corroborated by the survey responses where Site 2 reported using the pathway over twice as regularly (54.1%) as Site 1 (21.4%). The average LOS at Site 1 was 2.32 days longer than the average LOS at Site 2. The association between CHF pathway use and decreased LOS was further bolstered by the overall non-significant differences in patient demographics and ELOS at the two sites.
The CHF pathway and standardized order set have been revised and implemented.
5. Implications for Practice
The organization’s success and viability is dependent on the ability to provide evidence based quality care that promotes positive patient outcomes and achieves the targeted LOS without accumulating conservable days. If a patient is discharged prior to the ELOS, the organization receives the full financial benefit as if the patient stayed for the entire LOS, and has a bed available for the next patient, resulting in the compensation associated with the care of an additional weighted case.
An inability to do so results in negative patient flow, a decrease in quality outcomes, and cost escalation. An increase in LOS puts the patient at risk for potential adverse outcomes. These include, but are not limited to an increased risk for: 1) hospital acquired infections such as MRSA, VRE, 2) urinary tract infection if an indwelling catheter is utilized, 3) potential for medication error, 4) falls, 5) deconditioning, 6) delirium in seniors, and 7) development of pressure sores. All of these potential complications are harmful to the patient and are associated with increased care costs. The results of this study indicated that the number of conservable days incurred by CHF patients at both sites carries a financial burden. Any additional costs incurred by an unnecessary extended LOS cannot be supported. It is critical that practice standards and resources be directed to the strategies that are focused on positive patient outcomes, harm reduction and organization efficiencies.
Education must address the concerns from the survey that pathway use is too time consuming and does not impact patient care. Staff must be aware of the cost of conservable days to the organization and the potential impact that a funding deficit may have on jobs and services.
Achieving the expected LOS for heart failure (or any diagnosis) cannot be at the patient’s expense. As CHF is generally not a disease of the young, co-morbidities, functional status, cognition and a lack of personal and community supports can negatively impact pathway adherence and the ability to achieve targets. If achieving the LOS drives the discharge date, without consideration of the aforementioned variables, then patients may decompensate quickly, require readmission and ultimately increase care costs. A decrease in LOS is only a positive outcome if the patient’s overall status is considered, and the discharge is safe and appropriate.
6. Limitations
The accuracy of the data obtained was reliant on the accuracy of the chart audits, the inputting of admission/discharge information by the health records department, and reports formulated by the divisions of quality improvement and performance evaluation. Human and technological error, although not expected, must always be considered. Data obtained from staff surveys is dependent on individual practice and perception. Although the association between CHF pathway use and LOS, as discussed under objective four, consistently favors Site 2, the limitation of utilizing secondary data (i.e., chart audits and patient outcomes) and survey responses limits the ability to determine causation.
7. Conclusion
The prevalence, chronicity and significant mortality associated with CHF warrants its identification as a health care priority. The current and projected costs of CHF treatment on the health care system and the potential for CHF pathways to decrease LOS and conservable days is an important finding and warrants further investigation. Studies should aim for maximized homogeneity, clearly defined variables, and ensure that the sample, setting and pathway elements are relevant to the clinical question. Due to the confusion between clinical pathways and standardized order sets, consideration should be given to embedding the pathway components clearly within the order set without requiring a separate pathway document. This may improve compliance for use. Future research, specific to this organization, should assign, a priori, the CHF pathway to one site and utilize a matched control site in order to determine if the CHF pathway causes the promising outcomes, as observed in this study.
Competing Interests
The author have declared that no conflict of interest exists.