


1. Introduction
Internet use is an integral part of daily life and has radically changed the way people communicate, inclusive of how they seek information about health, wellness and disease [1]. Internet users now have access to information in real time, which creates a new milieu for nursing and other support services [2,3]. This information is often sought in order to self-diagnose or to diagnose the medical condition of someone else [4]. However, this online information should be treated with scepticism if the source is unknown, as health information not based on scientific evidence can pose increased risk, fear and distress [5]. The quality of information on health care websites varies, so it is also difficult for individuals to decide whether or not, to trust the information [6,7].
Individuals in the process of seeking illness information online also gain knowledge about the ways to access health professionals for support, or have found others who share their illness concerns [4]. An Online Support Community (OSC) that focuses on their particular disease or illness is one place where they can tell their story to others in a similar situation, and find information, advice and support [8,9]. There are numerous OSCs, some that focus on a specific condition such as fibromyalgia or diabetes [10] and others that focus on a category of disease such as cancer [11,12].
Individuals with breast cancer have indicated satisfaction with their ability to access the online stories of others, [13] particularly if the other person was in the same stage of the illness, had opted for similar treatment or had told a story of long-term survival [14]. Caregivers or supporters of those with breast cancer have also benefited from reading the narratives of others, as well as writing about their own thoughts and feelings concerning their burden of care giving or the effect(s) of the disease on their family member or friend [15]. Those with breast cancer stated that they felt better able to cope with their illness because their online interactions reduced uncertainty and anxiety, [13], major contributors to their distress [16].
A direct link between a cancer diagnosis and distress has been widely acknowledged in the literature, to the extent that distress has been referred to as the ‘sixth vital sign’ [17,18] that should be assessed by health professionals caring for a person with cancer. Significant psychological distress is suffered by half of all adults with cancer and much of this distress goes unrecognised and untreated [19]. Nurses who work closely with cancer patients are in an excellent position to screen for distress using the Distress Thermometer (DT) tool, and to provide timely intervention or referral to appropriate treatment providers [20].
Distress is described as
“…a multifactorial unpleasant emotional experience of a psychological (cognitive, behavioral, emotional), social, and/or spiritual nature that may interfere with the ability to cope effectively with cancer, its physical symptoms and its treatment. Distress extends along a continuum, ranging from common normal feelings of vulnerability, sadness, and fears to problems that can become disabling, such as depression, anxiety, panics, social isolation, and existential and spiritual crisis [16].”
Distress may result from the person’s struggle to adjust to or cope with the impact of cancer on their physical, emotional, and social well-being [21]. What is known is that support from others, particularly family and friends, helps to decrease the negative effects of cancer’s symptoms and treatments, and that it is important for health professionals to continue to assess for symptom distress and the adequacy of personal support throughout the cancer trajectory [22]. If the offline support of family and friends is not forthcoming, then the person may turn to the Internet and an OSC to find this advice and support. The supporter of someone with breast cancer may also seek information and support online through an online support group or community [23].
2. Methods
2.1 Research question(s)
Can the distress thermometer score of members of a breast cancer focused online support community be influenced by the information, advice or support provided by a Specialist Breast Care Nurse (SBCN) and the written expression of their emotions (SWEE)?
2.2 Study design
Netnography is participant-observational fieldwork in an online community, whereby data collection means observation and collection and analysis of the text-based communication between members of an online culture or community [25]. The researcher was a Clicker and participated in and/or observed the interaction on of the Click.
All Clickers were required to enter a Distress Thermometer (DT) score, per the Click membership process, then again in response to a survey question. The survey was posted six months after the SBCN had joined the Click. Once the individual had joined the Click, they were welcomed and encouraged to complete a 'structured written emotional expression' (SWEE) exercise in their Click blog space.
For the purposes of this paper, only the survey questions and responses related to the DT score, the SBCN support and the SWEE are used.
2.3 Research participants
While the broader Click membership base included the research team and some health professionals, only data related to Clickers with breast cancer, herein referred to as Clicker (BC) and supporters Clicker (S), was collected and analysed in this research study. The Clickers (BC) were in various phases of their breast cancer trajectory, some newly diagnosed and some undergoing active or palliative treatment or maintenance therapy.
2.4 Data collection
Data was obtained through an online survey and from the text/ posts on the Click website.
2.5 Survey
The survey was an online opt-in survey, which was posted to the Click home page six months after the part-time SBCN had been employed. Survey participants were asked to give their Click username so that their Click text could be identified.
2.6 Distress thermometer
The Distress Thermometer (DT) is a very brief screening tool consisting of a self-rating visual analogue scale with 11 points of measurement (0 = no distress and 10 = extreme distress) and a list of problems used by the self-rater to identify possible causes of their distress. The DT is used to measure psychosocial distress and related problems in cancer patients (see Appendix 1). The National Comprehensive Cancer Network (NCCN) developed the DT and it is an important part of the routine cancer care recommended in their good practice guidelines [25,26,21]. Permission was given by the NCCN for the use of the DT tool in this research project.
A DT thermometer score of four or greater than four indicated moderate to severe distress and alerted the SBCN to the fact that the Clicker needed help from other health professionals. This involved suggesting to the Clicker to contact their treating medical practitioner for assistance and referral to an appropriate health care practitioner as necessary. A score of less than four indicated mild distress or ‘expected distress’ that could be investigated and managed by the SBCN or the breast cancer team [21]. The DT score of four was chosen because this score was used in a community-based telephone helpline for cancer patients and their careers, which is similar to online contact in that the assessor and the patient are not meeting face-to-face [26].
2.7 SWEE
The SWEE formed a supportive intervention and avenue for Clickers to vent their feelings and relieve some of their distress. It also provided the SBCN with further information about the causes of the Clickers’ distress and the information, advice and support they required. On joining the Click, members were invited to write a SWEE which, according to the literature, can benefit their psychological and physical health [27-29]. A SWEE requires participants to write for 15- 30 minutes for 3-5 consecutive days, expressing their deepest thoughts and feelings about their or their family member/friend’s breast cancer experiences [30]. Offline this would be written in a journal or diary; online it was in their Click blog space. It could not be determined whether a Clicker had followed this particular process to complete their SWEE, but if the content provided insight into how the Clicker was feeling about their breast cancer experiences, it was considered to be a SWEE.
2.7 Reliability and validity
The DT has been used in psycho-oncology research in many countries, and has been recommended as a clinical tool that routinely detects clinically significant distress in cancer sufferers [31]. A systematic review of research studies to test the validity of the DT showed that the DT “…maintains good psychometric properties across countries and cultures; the values for sensitivity and specificity, and for positive and negative predictive value, are largely in the range typically characterized as representing good overall accuracy” [31]. DT cut-off scores have ranged from 3-5, with the cut-off score of four being the most commonly used scores [31].Reliability of the data was ensured by the triangulation of the data from three different sources: member posts, the survey and member checking.
2.8 Ethics
ECU’s human research ethics committee approved the research project and all procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1974, as revised in 2005 [32].
For Click membership, each person was required to acknowledge that they had read the research information and to give online consent to their participation in the research project. Consent to participate in the online survey was sought within the survey process, whereby the participant had to click “Yes” if they understood the purpose of the survey and agreed to participate. If they did not click “Yes” then they were not able to proceed any further in the survey. The respondent clicked on the submit button at the end of the survey and this showed implicit consent to participate [33]. The privacy and anonymity of the participants was protected by referring to those who have been quoted as Clicker (BC), Clicker (S) and SBCN.
3. Results and Discussion
There were N=385 Clickers at the time the survey was posted and although this is a substantial membership, it must be noted that only a small core of Clickers actively (visibly) participated on a regular basis in the Click activities. It is not unusual for only a small number of OSC members to actively participate in an online community at any one time. A large majority of OSC members can participate by reading what is posted and not posting or entering a chat room and not posting any text, therefore they are largely invisible [34]. Sometimes referred to as ‘lurkers’, research has shown that these people still consider themselves to be members of the OSC [34]. It is also possible that some members join an OSC and never return to participate either visibly or invisibly [35].
Thirty-six Clickers completed the survey, one a health professional whose response was discarded from the results. All 36 participants completed the DT at membership and 30 participants completed the second DT in the survey six months later. This was a response rate of almost 10 per cent, which was reasonable, given that only two per cent of members in some online communities actively participate [34].
Ten participants, including eight females with breast cancer and two supporters (one female and one male), gave their usernames to enable the identification of their membership DT scores and SWEEs. Therefore, only 10 data sets were analysed in the results presented in the table 1.
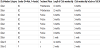
The changes in the distress thermometer scores of the ten participants are presented in the Graph I.

3.1 Decrease in DT score
When the two DT scores were compared, six Clickers, five with breast cancer and one supporter showed a decrease in their DT scores. Of the six, five had been Clickers for six to 14 months and all five indicated that the SBCN’s information, advice and support had been instrumental in decreasing their DT scores.
The Clicker (S) in the above group of five had a DT score of seven on joining the Click, which is the second highest recorded, but after 14 months membership she recorded a DT score of two in the survey. This score reflects research showing that supporters of people with cancer have a higher DT score than the person with the cancer. While in this instance the DT score of the supported person was not known, this Clicker did have a membership score higher than the Clickers’ (BC) in this survey group [26].
To the survey question: What was the advice that helped decrease your Distress Thermometer score? The Clicker (S), (verbatim) response, was:
“What cancer is as when my wife was told i did not know a lot about what may happen i just was thinking of the word Cancer and what i knew it to mean as in Death?”
Notably, this Clicker was also a lurker, who read the online information but had only posted once, thereby confirming the notion that lurkers can learn as effectively as those who visibly and actively participate in an OSC [36]. Lurking online could also have prevented or minimized any distress that can be caused by difficulties in accessing or using the website facilities, referred to later in this paper.
3.2 DT score remained the same
Three Clickers’ DT scores remained the same as their membership DT scores, and none of these were higher than three. One Clicker (BC) scored zero on both DT scores and this could be attributed to having completed her breast cancer treatment some seven years prior to joining the Click. All three indicated they had benefited from the SBCN’s support and advice.
3.3 DT score increased
This experience illuminated the need for a richer understanding of the people and their systems, partnership dynamics and a rethinking of the process of community engagement to promote a shared stakeholder vision and ensure engagement success where engagement is a rich platform for social learning.
One Clicker said their score had increased from 5 to 10. This Clicker had been a member for one week and indicated that she had not actively participated other than completing the survey. Her survey comment was: “I have just had diagnosis, a mastectomy and reconstruction all in 3 weeks …I was much stressed when I tried to get into the chat room but I wasn't really ready for it and it made my distress worse, too busy dealing with the process of operation. I received a message from one of the members [the SBCN] who gave support.” The factors contributing to her distress could not be ameliorated to any great extent because of her brief time on the Click, which was further escalated by the difficulty she had accessing the chat room. However, a prompt supportive response was provided by the SBCN, which could, depending on its content, lead to a decrease in the Clicker’s distress level. If the Clicker is not computer-savvy or has difficulty accessing the website, then this can further escalate distress as shown by one Clicker’s survey comment: “I would like to see the usability improved; especially when it is a place I have turned to while distressed and seeking support/help”. These comments prompted the Click research team to review the useability of the site and post clearer instructions for website and chat room access [37].
The following are verbatim examples of the SBCN personal messages to Clickers. Firstly, a message to a Clicker with a high distress score and secondly, a message to a Clicker who initially recorded a very low distress score and subsequently became extremely distressed.
SBCN: Hi […] I’ve noted you have a very high distress score – please contact your local support services or GP if not already receiving support.
SBCN: Oh […] I'm so sorry to hear it's a big struggle ... yet not surprised! You ARE Wonderwoman, but not beyond all aspects of being human!!! No-one could deal with all you do. Several options: 1) Breast Cancer Clinical Psychology Service (free). Fantastic ladies - qualified Clinical Psychologists specialising in breast cancer and associated aspects. I know them and they are great. However they do get booked up so may not get an appointment for a few weeks (I can contact them/send referral for you and find out). **Also depends if you want the psychological approach ... discussing coping styles /strategies. […] Will do phone consultations. Ph:[…] (message machine - leave your contact details) 2) Breast Cancer Care WA (free) - have several counsellors … Look more into imagery / thought patterns / tools for coping, etc. Ph:[…] - ask to speak to a counsellor. Are flexible with services 3) See GP or contact Cancer Council 131120 - who may be able to recommend a counsellor locally. Likely to be a fee involved, may be eligible for Medicare rebate (not for full amount) under 'mental health care plan for a series of sessions. I will try to ring you tomorrow (is in clinic but will find time somewhere!). Sending hugs & talks soon! xxx
3.4 SWEE
Four Clickers (BC) in the survey stated they completed a SWEE; of these, three showed a decrease in their DT score and one DT score remained the same. The Clickers (BC) who had a decrease in their DT score and who had written a SWEE were stalwarts of the Click community, as was the Clicker whose score remained the same. Each of the four Clickers responded positively when asked if the advice and information that the SBCN provided them with, was instrumental in decreasing their DT score. A typical comment follows:
3.5 Clicker (BC)
“Support regarding my fears of tests and treatments that I was due to
have. It was good to have the SBCN to interpret the medical jargon).”
One Clicker (BC) wrote in capitals, which is referred to as online
‘shouting’ to emphasise her point: “WRITING A BLOG (SWEE) -
THAT REALLY HELPED” but did not give any details.
The following is an example of a SWEE written by one of the four Clickers mentioned above and responded to by the SBCN and other Clickers:
What? It's Monday already? How did that happen & who got the number of the road train that hit me? Every muscle is aching & every noise reverberates through the head like a banshee. [...] I thought I had this covered.. Friday was a good day! Day 1 after 1st treatment & I was feeling really good - great in fact! [...] I did go in to work (and stayed until 7pm) perhaps that was my mistake. But I felt great & didn't want to lose momentum. Progress was made. That's good right? Saturday a bit slower resting on & off. Just tired from the 1st treatment day marathon & the day of work? [...] Sunday..Slower still surely I should be over the tiredness the culmination of the past 7 weeks. Apparently not. Monday & yes - I'm looking for the driver of that road train. I anticipated being able to go in to work this afternoon but that's just not going to happen. A quick chat to S… before the nausea decided to threaten & I learn I have been tricked! Damn you 'roids! Giving a false sense of everything. Right now this minute I feel ok again but I know that's the pain meds. In 30 seconds I'll probably have another hot flash & my head will start aching again. My mouth feels like it's packed with cotton wool & I need water. Should I go to bed? Yes. Do I want to? No. This feeling of not being in control I hate it. Looking forward to tomorrow.
The Clicker who writes a SWEE can make it public or for friends and family only, to read. Selecting friends and family provides the Clicker with a way of letting their supporters know how they are feeling without the stress of talking about their illness face-to-face. In turn, supporters become aware of their loved one’s thoughts and feelings and learn how best to support them [38]. If the SWEE is made public, all Clickers can read the SWEE, identify how that particular Clicker is feeling and provide advice and support. Alternatively, the Clicker who reads the SWEE may recognise someone in the same situation as themselves, and so commences a private online dialogue with them. Either way, there is potential for a decrease in the distress felt by those involved.
Writing a SWEE has been shown to have positive effects on the physical and psychological health of those with an illness and their supporters [39,15] but it was not the aim of this project to determine the extent of these benefits. Rather, the objective was to provide the Clicker with an written avenue for expressing their distress. The examples provided demonstrate the expression of this distress and the support and advice received.
Nurses have played a pivotal role in the conduct of research into the use of the DT in cancer patient care [23] and the DT has been utilised in various stages of a person’s cancer trajectory. The use of the DT by a nurse in her online practice can be seen as an innovative, yet natural, extension of their offline nursing practice.
Although research studies have shown that the DT has primarily been used in face-to-face situations (for example in hospital and outpatient clinics [12,27-29], it has also been administered via the telephone in a community-based cancer helpline service to assess the distress of both patients with cancer and their supporters/carers [26]. Online administration of the DT can be viewed as similar to this because the individuals do not meet face-to-face, however online use could prove to be superior because the user has time to read and understand the information, whereas the telephone method is reliant upon the person understanding what is said to them at the time of the phone call.
4. Limitations
There were relatively few survey respondents, but these were representative of the Click population.
5. Conclusion
The DT can be used online to assess the distress level of members of a breast cancer-focused OSC and that the evidence-based information, advice and support provided by the SBCN can result in a decrease in this distress level. DT scores should be sought more than once, perhaps before and after each phase of treatment, in order to minimise or prevent a high level of distress from occurring.
Although a direct connection between the writing of SWEEs and their effect on the Clicker’s distress score could not be made, research indicates that distress does decrease when people write about their traumatic experiences offline in a journal or diary [40]. It follows that taking this structured writing online should have a similar effect, provided the website is easy to access and use.
It is anticipated that in the future, more nurses will be employed to practice online in an advice, support and referral capacity. The DT could be easily incorporated into this practice.
Competing Interests
The authors have declared that no competing interests exist.
Author Contributions
All the authors substantially contributed to the study conception and design as well as the acquisition and interpretation of the data and drafting the manuscript.
Acknowledgments
Many thanks to the Clickers who participated in this study.