


1. Introduction
Haptic TheraDrive is a low-cost robotic system for post-stroke upper extremity (UE) rehabilitation. The system uses off-the-shelf computer gaming wheels with force feedback to help reduce motor impairment and improve function in the upper extremities of stroke survivors. Preliminary results from studies have shown that the Haptic TheraDrive system is not capable of delivering effective therapy to low-functioning patients; it also lacked a patient specific adaptive controller for personalized therapy [1]. A new low-cost, high-force haptic robot with a single degree of freedom has been developed to address these concerns [2]. The aim of this case is to determine the impact on motor performance and function when this new custom force-feedback device, Haptic TheraDrive (Figure 1), is used to complete games for rehabilitation by a low-to-moderate functioning stroke survivor with hemiplegia.

According to the United States Center for Disease Control and Prevention the prevalence is more than 795,000 people in the United States have a stroke every year [3]. With an incidence of approximately 610,000, an estimated 185,000 Americans have had a previous stroke [4]. However, stroke as a leading cause of serious long-term disability, also presents as a global disease burden. Despite global age-adjusted mortality rates for ischemic and hemorrhagic stroke decreasing between 1990 and 2013, the absolute number of strokes annually, as well as stroke related deaths and disability-adjusted life years (DALYs) lost, increased [4,5]. Globally in 2010, the prevalence of stroke was 33 million [6] with an estimated incidence of 16.9 million events [5]. The mortality world-wide in 2013 was 6.5 million stroke deaths, making stroke the second leading cause of death [7]. Measurement of disability by DALYs in 2010 totaled 102.2 million. The majority of global burden is in low-income and middle-income countries [5,7] suggesting a need for affordable care.
Upper extremity impairments that require intervention for recovery are caused by contralateral brain lesions in individuals with stroke. However, it has long been believed that stroke patients with mild to severe UE paresis should not be expected to have further functional recovery respectively 6 and 11 weeks after stroke onset [8]. Less than 20% of patients with severe UE paresis achieved full UE recovery [8]. Current guidelines for adult stroke rehabilitation and recovery in the United States note that formal rehabilitation, commonly 3-4 months after stroke, should not mean the end of the recovery [9].
Due to the paresis, strength deficits are an important target for clinical intervention. In Brazil, using the International Classification of Function the interrelationship between the UE body structure impairment/function, activity and participation of the arm function in chronic stroke subjects was observed [10]. It was found that grip strength alone could account for variances of 62%, 54% and 36% respectively in the activity measures of Test d' évaluation des membres supérieurs des personned âgées (TEMPA, a test of UE performance of eight tasks representing standardized daily activities), Box and Block Test (BBT) and Nine-hole Peg Test. Shoulder pain accounted for 30% of the participation measure Stroke Specific Quality of Life Scale.
Significant improvements in the BBT, Fugl-Meyer Arm Motor Scale (FMA), Wolf Motor Function Test, Motor Activity Log, shoulder and elbow strength, and reaching speed have been achieved after exoskeleton robotic training [11]. However, moderate-to-low functioning chronic stroke subjects were not included. The twenty subjects that participated had only mild to moderately impairment as indicated by FMA scores of 52 ±8. This training with a robot with multi-joint six degrees of freedom was found not to be superior to training with a single joint, one degree of freedom robot.
Robot-assisted reach training is able to significantly improve the kinematic movement velocity performance and the function of the upper extremity as measured by the Action Research Arm Test, a 19 item measure of UE activity with 4 sub-tests (grasp, grip, pinch and gross arm movement). However, prior studies enrolled high functioning chronic stroke survivors and used an expensive whole arm manipulator robot [12]. Thus, little research exists involving patients with chronic stroke disability and moderate-to-severe upper limb impairment. In the VA ROBOTICS trial, stroke survivors with moderate-to-severe upper limb impairment demonstrated a 8 point difference in the FMA as compared to subjects receiving robotic treatment in the second half of a study and subjects receiving usual care during the first half of a study as provided by Veterans Affairs (VA) therapist in the VA ROBOTICS trial [13,14].
Robot-therapy has 73 out of 100 groups focused on recovery in the chronic stage of stroke [15]. Robotics now afford an intervention for recovery of function that was previously determined not to be expected in chronic strokes. Krebs [13] notes this paradigm shift where robots are moving beyond assistive technology to robots that facilitate recovery. The American Heart Association [9] recommends robotic therapy is reasonable to consider to deliver more intensive practice for individuals with moderate to severe upper limb paresis with robot-assisted therapy for the upper extremity achieving Class IIa, Level A evidence. Although current literature needs to provide information on the physical human-robot interaction mechanism, the HRI features, to allow for comparing therapeutic effects and benefits [15].
Haptic TheraDrive is a robot with a haptic control strategy with a force feedback feature and a single degree of freedom. This case presents a chronic stroke survivor with a low-to-moderately impaired UE and the impact of the custom force-feedback device (Haptic TheraDrive) on motor performance and function.
2. Materials and Method
A single subject repeated measures case study design was used. A battery of tests were assessed at baseline, after 10 sessions of Haptic TheraDrive use, and at one month follow up. Robot therapy does not have a standard application of time. Effects have been seen with a variety of strategies. Ten sessions to 12 sessions at a frequency of 3 times per week was chosen to fit in the outpatient setting paradigm and standard of care for therapy at the urban rehabilitation hospital. The subject was evaluated to determine their level of impairment using the: Montreal Cognitive Assessment (MoCA) [16] , Beck Depression Inventory (BDI) [17], Fugl-Meyer Assessment for the Upper Extremity (FMA-UE) [18,19], grip strength using a Jamar® dynamometer [20,21], BBT [22], and the Modified Ashworth Scale (MAS) [23]. The author (CAW) has over 25 years of experience in neurological physical therapy care and was able to serve as an expert clinical evaluator.
The setting was an urban rehabilitation robotics lab. The subject was a 52-year old male 22 months post stroke. Consent of the participating subject was obtained. He was not receiving therapy and worked a sedentary office job. The subject reported difficulty with activities of daily living (ADLs) of inability to independently use his involved UE to bathe his uninvolved UE and was unable to retrieve his wallet out of his left rear pant pocket. The subject was not cognitively impaired as demonstrated by a MoCA score of 30/30 and did not demonstrate depression on the BDI. He had a low-to-moderate functioning left UE with a FMA-UE of 37/66. His left grip strength with a dynamometer was 16.76 pounds as compared to 72.46 on the right on averaging of 3 trials. A Modified Ashworth Scale 1-1+/4 in his left shoulder adductor, elbow flexor, forearm pronator and wrist flexors, reflected increased but not debilitating spasticity. Initial performance of the BBT resulted in a score of 9 on the left compared with 49 on the right. The subject did not have arm contractures, had never received Botox® injections, and had no complaint of UE pain.
Haptic TheraDrive robot (static and adaptive force modes) for computer gaming of movement timing, velocity and accuracy was used 3 times per week for one month for a total of 10 sessions. Each session was approximately 45-60 minutes. The subject's fatigue was monitored every 15 minutes via questioning to rate fatigue on a verbal analog scale. The level of fatigue ranged from 0 (no fatigue) to 10 (worst fatigue ever). Session duration depended on the level of fatigue of the subject and would be stopped if the subject reached a level 6 on the verbal analog scale.
During each session the subject would be allowed to choose between different games. Due to the nature of the one degree of freedom of the Haptic TheraDrive robot all games had one degree of freedom that involved racing using Mario Kart™ or shooting using Galaga™ game. The intervention sessions were structured to enhance motivation and game performance. An adaptive controller monitored the subject's performance to ensure that the exercises were difficult but able to be completed by the participant. During each game, at the discretion of the author (RR) and the game score of the subject, the level of difficulty could be increased or decreased. Game score is a measure of motor performance, speed of crank arm rotation related to game performance and was therefore used as a subject-centered measure of performance, which was also related to keeping the subject engaged in therapy. The aim was to keep the subject motivated, challenge their performance limits, and ensure the subject did not get frustrated.
3. Results
After completion of the 10 sessions the subject demonstrated a FMA-UE score of 45/66, which was maintained at the one month follow up (48/66) (Figure2). The FMA-UE component of fingertip knee to nose was used to measure coordination and session 10 indicated a performance of 11.44 seconds with a speed at follow up of 10.8 (Figure 3). Left hand dynamometry assessed pounds of grip strength at 19.7 and 23.23 respectively at session 10 and 1 month follow up (Figure 4). Figure 5 demonstrates the number of blocks manipulated as measured with the BBT for 20 blocks at both the tenth session and at follow up.
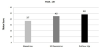
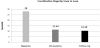


After session 10, the subject demonstrated an 8 point improvement in the FMA-UE and a 59% increase in coordination speed, 18% increase in grip strength and 122% increase in BBT score. Functionally he could use his left UE to shower his right shoulder and reach his left rear pant pocket.
At one-month follow up the subject demonstrated gains in the FMA-UE, coordination speed, and grip strength (Figures 2-4). Since completion of the training long terms gains at one-month included: FMA-UE (3 points), coordination speed (9%) and grip strength (18%). BBT gains were sustained at 122%.
4. Discussion
Haptic TheraDrive provides an adaptive controller using forcefeedback to deliver individualized and effective therapy for a single low-to-moderate functioning stroke survivor with hemiplegia. After ten sessions, this subject demonstrated improvements in FMA-UE, coordination speed, grip strength and BBT score.
The FMA-UE for assessing impairment has a minimal detectable change of 5.2, 8% of the total UE score of 66 [24]. After session 10, the subject demonstrated an 8 point improvement. At his onemonth follow up there was an 11 point increase from baseline with both instances clearly demonstrating a positive change. All primary outcomes (FMA-UE, ADLs, BBT and dynamometry) demonstrated improvement and were sustained and/or gained at one month follow up. He was able to pick up 11 more blocks indicating improved manual dexterity. A study limitation is that ADLs were not formally assessed for activity limitation with such measures as the Action Research Arm Test or Motor Activity Log. However, the subject did provide anecdotal report of having achieved the ability to use his left UE to reach his left rear pant pocket for his wallet. Even more importantly, was the report that he became independent in his bathing and now uses his involved UE to bathe his uninvolved shoulder when showering. These outcomes provide support for the Haptic TheraDrive’s ability to deliver effective therapy to an individual low-to-moderate functioning stroke survivor.
The subject’s MAS at baseline indicated increased left UE tone in a flexor pattern. It was noted that the subject's tone was less at the beginning of the battery of outcome measures as compared to when actually assessed at the end of the test battery. The temporal consideration for the administration of the MAS as well as activity influencing the subject’s tone served as confounding factors making it difficult to draw comparisons before and after the Haptic TheraDrive intervention [25]. Additionally, follow up was not pursued beyond one month therefore it is not known if the subject's gains were sustained over a longer period of time.
The use of the FMA and other outcome measures has good retest reliability. However, as this is a single-subject design, an alternate design would have been useful to establish that no spontaneous improvement was occurring and that the differences between testing sessions were indeed due to treatment change, versus variability such as tone. This particular individual had a good outcome from the intervention but the authors cannot conclude this effectiveness for the population of chronic low-to-moderate functioning stroke survivors without further study.
An additional limitation is that data does not reflect the entire performance of the unaffected arm. Often the aim of rehabilitation is to recreate function by recovery of the affected side and/or by compensation using the non-affected side. The compensation is especially important when the recovery of the affected side cannot be achieved. Therefore, the overall function should be evaluated in the assessment of recovery [8]. Nakayama, et al. in the Copenhagen Stroke Study in 1994 demonstrated that recovery of UE function in more than half of the stroke patients with initial severe UE paresis could only be achieved via compensation by the unaffected limb [26]. Intervention now with robotics indicates other than compensation can be achieved.
Robots could transition from intervention to clinically assessing and validating hemiparetic movement [27]. Future robots could incorporate task-oriented training versus gaming, as this subject did, for motivation and interest [28]. There exists evidence that robotic interventions improve upper limb motor scores and strength but, does not transfer to activity in a chronic stroke population. The work indicates a need for active assisted mode intervention for the whole arm [15]. Finally, for the millions of stroke survivors living with chronic UE paresis there is potential to use home therapy as an opportunity to provide an affordable dose of home physical activity. Individuals with severe arm impairment are limited by an inability to complete exercises at home without assistance. Zondervan, et al, used the Resonating Arm Exerciser (RAE) machine in the home, which demonstrates exercise for this population is feasible without human assistance [29]. Yet to be explored is whether the Haptic TheraDrive, a robot, can improve outcomes and provide the automated assistance in the home for stroke survivors with severe impairments.
5. Conclusion
Research is beginning to recognize that robots have a role in rehabilitation. Robotic rehabilitation and gaming can have an impact on clinical outcomes in a patient with upper extremity hemiplegia and on the functional outcomes in the low-to-moderate chronic stroke survivor. The intervention of the Haptic TheraDrive impacts motor performance, function, grip strength, coordination, finger dexterity and to a lesser extent spasticity. Further study is warranted to assess the effectiveness of Haptic TheraDrive for the population of low to moderate functioning stroke survivors. The long-term goal is to develop an inexpensive high-force haptic rehabilitation robot that can safely be used by patients in low and middle-income countries and in the home.
Competing Interests
The authors declare that they have no competing interests.
The project was funded by the American Heart Association. The robot is
not commercial. The robot developer (MJJ) is interested in the ability
of the system to support recovery in this population.
Author Contributions
CAW: Contribution to selection of outcome measures, administration of physical outcome measures, acquisition and interpretation of case data, drafting and revising of manuscript, and final approval of the version to be published.
RR: Operation and maintenance of Haptic TheraDrive robot; implementation of interventions with Haptic TheraDrive; provider of computer gaming with acquisition of data on movement timing, velocity and accuracy; lab manager; and final approval of the version to be published.
MJJ: A developer of Haptic TheraDrive robot, primary investigator of Haptic TheraDrive usability and motor outcomes in stroke, selection of outcome measures, interpretation of data, lab director, revising of manuscript, and final approval of the version to be published.
Acknowledgments
Jennifer Dekerlegand, MPT for editorial assistance.