


1. Introduction
25% of all cervical spine injuries affect the axis [1,2], of wich odontoid fracture represent 10–15% [3]. These fractures were classified into three distinct types by Anderson and D’Alonzo [4] in 1974. Type I odontoid fractures are quite uncommon and involve an avulsion of the rostral-most portion of the dens. In contrast, Type II fractures are the most common odontoid fracture, occurring in 65%–74% of the cases [4,5]. The fracture line traverses the base of the odontoid process at the junction of the vertebral body. A lateral bending force has been proposed as the mechanism causing the development of Type II fractures [6]. Finally, Type III fractures actually extend into the body of the axis, frequently involving the superior articular surface. These fractures may be caused by a flexion moment through the occiput [6]. Management for odontoid fractures includes anterior odontoid screw fixation, posterior wiring and bone grafting of C1–2 (Gallie, Brooks-Jenkins), transarticular screw fixation (Magerl) [7], C1 lateral mass screw fixation described by differents authors: Goel and Laheri [8] (associated with a C-2 screw lamina, pars, or pedicle) in 1994, this technique was modified by Harms and Melcher [9] in 2001 to use polyaxial screws and rods instead of a plate. In 2012 Reis and al. [10] proposed a novel technique using opposing laminar hooks to form a claw at C-2 combined with C-1 lateral mass screws ; as well as nonoperative strategies, such as immobilization by a halo vest and cervical collar [11]. A review of the literature shows that the best treatment strategy for Type II odontoid fractures remains controversial [12-14]. In this paper, we present five cases of Type II odontoid fractures (TOF) OBAV treated by Harm's technique [9] and a new C1 lateral mass/C2 laminar hooks procedure in posterior approach that we propose as an alternative procedure for the surgical management of TOF OBAV.
2. Materials and Method
2.1 Patient demographics
Patient Demographics. Five patients underwent Harms's technique and and a novel C1 lateral mass/C2 laminar hooks procedure in posterior approach for TOF OBAV. All patients were male. The average age was 49,2 years (range 16-75 years).The mean follow-up was 10 months. In 80 % of the cases, fractures occurred in a high energy trauma (Intentional Injury, Motor Vehicle Accident, fall from a height) and in 20 % were secondary to low energy trauma (fall). The revealing clinical presentation is described in table 1.

Fractures are classified according to the classification of Anderson and D'Alonzo [4]. The postoperative clinical evolution was studied according to the modified Rankin scale (mRS) (Table 1).
2.2 Surgical technique
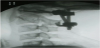
Posterior screw fixation was performed using 3.5 x 24 mm or 4.0 × 30 mm polyaxial screws. Screws were inserted bilaterally into the C-1 lateral masses and C-2 pedicles, as described by Harms and Melcher [9].
Titanium rods (3.5 mm in diameter) were fixed to the connectors on the C1 and C-2 screw heads with locking nuts (Figure 1).

The screw-hook-rod construct consisted of a hook and a screw interconnected on a single rod (Figure 2). The hooks were inserted in contact with the caudal border of the C2 lamina, as laterally as possible from midline, to facilitate the connection of the rods.
3. Results
All patients were surgically treated posteriorly (Table 2). The mean follow-up was 10 months. Clinical outcome was improved in all cases. Bony fusion at lateral-view and openmouth view on Xrays was considered good in 4 patients. We observed a case of an infection of the surgical site resolved under antibiotics.

4. Discussion
Like our series the causes of these injuries are, falls in the elderly or high-velocity accidents in the young and middle-aged. The fracture mechanism is hyperextension or hyperflexion of the cervical spine. The incidence of neurological involvement after odontoid fracture has been reported to be between 0% and 27% [4,15,16]. Neck pain is the main symptom. Plain radiography remains the mainstay for identification of odontoid fractures [17,18]. Both lateral-view and openmouth view radiography may demonstrate the fracture. The magnitude and direction of displacement should be noted because this may be related to failed bone union when nonoperative management is undertaken. In addition, the ligamentous stability of the atlantoaxial joint can be estimated by measuring the atlantodental interval. Fielding and al. [19], have suggested that a greater than 3 mm separation between the anterior C-1 ring and the dens implies possible transverse ligament disruption. In addition, Spence et al. [20], have suggested that when the lateral masses of the atlas overhang the superior articular facets of the axis by more than 7 mm, injury of this ligament may similarly occur.
The use of CT scanning may be quite helpful in demonstrating the plane of the fracture line as well as the degree of comminution [18]. Both sagittal and coronal CT reconstructions often delineate the fractures more precisely than plain radiographs. However, CT scanning occasionally fails to demonstrate a fracture in the transverse plane if the gantry angle is parallel to the fracture line. MRI has a more limited role in evaluating patients who have sustained odontoid fractures without neurological injuries [18]. However, evaluation of the integrity of the transverse ligament can be facilitated using MRI. Multiplanar gradient echo modalities have successfully demonstrated disruption of this ligament, prompting operative treatment rather than applications of external immobilization devices alone.
The optimal treatment of TOF is controversial. Nonsurgical treatment with a cervical collar or halo vest has a nonunion rate of as high as 40% [21]. For this reason, surgical treatment is especially indicated in patients who have a higher risk for nonunion. In this context, surgical treatment with posterior cervical instrumented fusion increases the fusion rate to more than 80% in many patient series [21,22].
The posterior surgical approach represent [8,9] a good technique for the management of TOF OBAV.
Some authors have reported up to 98-100% healing with posterior C1–2 arthrodesis [9,22-25] .
Using C-1 lateral mass screws and C-2 pedicle screws with a polyaxial screw/rod system like 3 cases of our study is favored by some authors [9,24] and has a low complication rate.
Our novel screw-hook-rod construct consisted of a hook and a screw interconnected on a single rod. It is an especially attractive option in osteopenic patients, where screw pullout would be a concern.
The screw-hook-rod technique like the standard Harms technique, making it an acceptable alternative technique when aberrant arterial anatomy precludes the placement of C1–2 transarticular screws.
In a human cadaver study, Fagerström and al. [26] found that 95% of 77 cervical laminar hooks placed, no deformation of the dural sac was observed and there was no evidence of spinal cord compression.
Winter [27] reviewed the risk factors for spinal cord injury during cervical spine surgery and pointed out that direct trauma to the spinal cord caused by hooks was a hazard. Using of hook does require intact posterior elements [28]. Our two procedures can be performed in all cases of TOF OBAV where the lateral mass are normal.
Compared with a posterior laminar hook procedure, the screw/ rod system does not require intact posterior elements, which can be disrupted in conditions such as trauma [29].
The transarticular screw system does not require intact posterior elements; however in the litterature review [23] the incidence of malpositioned screws and vertebral artery injuries was 1.4 and 1.7%, respectively after atlantoaxial transarticular screw fixation.
We found no previous study tested the C1 screw and C2 hook-rod technique in the litterature.
Further others studies will be necessary to evaluate this procedure (C1 screw and C2 hook-rod technique) and compare to others posterior procedures.
5. Conclusion
The screw-hook-rod technique like the standard Harms technique, making it an acceptable alternative surgical procedure for TOF OBAV. Surgeons might consider theses differents approachs techniques before realizing a treatment.
Competing Interests
The authors declare that they have no competing interests.
Author Contributions
All authors contributed to the design, analysis and interpretation of the data, the writing of the article or the critical revision of its intellectual content. All authors have read and approved the final version of the manuscript.
Abbreviations
CSF : Cerebrospinal Fluid; CT: Computerized Tomography; InI: Intentional Injury; MRI: Magnetic Resonance Imaging; mRS: modified Rankin Scale; MVA : Motor Vehicle Accident; OBAV: Fracture line Oblique from posterosuperior to anteroinferior; TOF: Type II Odontoid Fracture