


1. Introduction
Orthognathic surgery is required for many cases of class III malocclusion for improving function and establishing a symmetric aesthetic face [1-6]. Accurate diagnosis of facial asymmetry might be essential for both presurgical treatment planning and postsurgical evaluation. Although the radiation dose of computed tomography (CT) is significantly higher than that of a conventional cephalometric radiograph three-dimensional (3D) CT is becoming more popular because 3D CT has no superimposition, dimensional change or distortion of structures which are inherent shortcomings of two dimension imaging [7]. There have been many studies for developing the evaluation methods of facial asymmetry using 3D CT. However the evaluation method of facial asymmetry has not yet been established [8-13].
Facial asymmetry can be evaluated by analyzing some facial lines [10]. An alternative spherical coordinate system was developed from the geographic coordinate system for analyzing facial lines and asymmetry [12-14]. Three-dimensional analysis of facial asymmetry can be effectively achieved by using a spherical coordinate system(v,θ,ϕ) of 3D facial lines, where v is length, θ midsagittal inclination angle, and ϕ coronal inclination angle. The alternative spherical coordinates can be calculated from rectangular coordinates(x,y,z) of landmarks which compose the facial lines. The rectangular coordinates are obtained from three orthogonal planes, midsagittal, coronal and horizontal reference planes.
Over the last few decades, studies about the changes of hard and soft tissues by orthognathic surgery through a 3D CT have been significantly developed [13,15-21]. However, only a few studies were conducted about facial asymmetry remaining after surgery [13,15,18,21].
The purpose of this study is to compare the amount of asymmetry of facial lines before and after orthognathic surgery by analyzing a spherical coordinate system of 3D facial lines on CT.
2. Materials and Methods
2.1 Study subject
Fourteen CT images of seven subjects (3 males, 4 females, average age 24 yrs±3 mns,; ANB -6.0˚±2.86˚) were reviewed for this study. CT scans had been taken before and after orthognathic surgery at Chonnam National University Hospital from 2003 to 2009. Two subjects received two-jaw surgery with genioplasty, two received two-jaw surgery without genioplasty and three had only mandibular surgery with genioplasty.
2.2 CT SCAN
CT scans were obtained by a spiral CT scanner (Light Speed QX/I, GE Medical Systems, Milwaukee, WI, USA). The scanning time was 0.8 sec with 2.5 mm axial image thickness and 3 mm/sec table speed. Digital imaging and communication in medicine images were obtained with 1.0 mm slice thickness. The acquired data were transmitted into a personal computer, and 3D image reconstruction was performed by the combined software of Vworks and Vsurgery (Cybermed, Seoul, Korea).
2.3 Measurement of the deviation of the Me
The menton (Me) was defined as the most inferior point on the mandibular symphysis.The deviation of the Me was measured as distance of menton from midsagittal reference plane on the reconstructed CT scan.The side of the face with the Me was identified as the deviated side, while the contralateral side of the face the opposite side [10].
2.4 Spherical Coordinate system of facial lines and amount of asymmetry
The horizontal ,midsagittal and coronal planes were established to be perpendicular to each other. The horizontal reference plane was first established using the right Po, right Or, and left Or. The midsagittal reference plane was formed using Na and Op. The Op was also used to establish the coronal reference plane. The condylar and gonion landmarks were identified. The most superior point of condyle and the most inferior point of gonion composed the ramal height line (Cdsup-Goinf). The most lateral point of condyle and the most lateral point of gonion composed the ramal lateral line (Cdlat- Golat). The most posterior point of condyle and the most posterior point of gonion composed the ramal posterior line(Cdpost-Gopost). The most posterior point of gonion and the Me composed the mandibular body line(Gopost-Me). The rectangular coordinates (x,y,z) of the landmarks were obtained from the orthogonal reference planes (Figure 1, Table 1) [10,12].


Figure 2 shows the definition of the spherical coordinate system (v,θ,ϕ) of the mandibular body line as an example (Figure 2). The spherical coordinates (length, midsagittal inclination angle, and coronal inclination angle) of the bilateral facial lines were mathematically calculated from the rectangular coordinates (x,y,z) of the landmarks, where xwas set to absolute values to reposition the right side of the face to the left side as a mirror image. The mandibular body line (Gopost-Me) was formed as (xgo-xme, ygo-yme,, zgo- zme), where (xgo,ygo, zgo) is for the Gopost and (xme,yme, zme) for the Me. The mandibular body line was identified as a vector and its length ,v, was calculated. The angle between the midsagittal reference plane and the vector was identified as midsagittal inclination angle, θ. The angle between the coronal reference plane and the vector was identified as coronal inclination angle,ϕ. The spherical coordinate (v,θ,ϕ) of the other facial lines was made in the same way [12]. If x=xg-xme, y=yg-yme, and z= zg-zme, the spherical coordinates (v,θ,ϕ) were obtained from the formulae as below:
Sin θ= x/v,
tanϕ= y/z,
for θ,ϕ in radian measure (θrad = θ °× π/180).
Additionally, amount of asymmetry (dv,dθ,dϕ) of the facial lines before and after surgery was evaluated.
(dv,dθ,dϕ) = (v,θ,ϕ)deviated - (v,θ,ϕ)opposite
Because all the bilateral facial lines have different starting points on the three-dimensional space, it was also necessary to describe the starting point for a definite representation of the vectors. The bilateral difference (dx,dy,dz) of starting points, Goinf, Golat and Gopost , were obtained [12].
(dx,dy,dz) = (x,y,z)deviated - (x,y,z)opposite

2.5 Statistical analysis
The comparison of the menton deviation after surgery with that of before surgery was done by Mann-Whitney U test. Spherical coordinates (v,θ,ϕ) and amount of asymmetry (dv,dθ,dϕ) of the facial lines before and after orthognathic surgery were compared by Wilcoxon’s signed-rank test. IBM SPSS statistics software (IBM Corporatism, United States) was used for statistical analysis.
3. Results
The menton (Me) deviation after surgery was significantly lower than before surgery preoperative 7.67 mm±4.46mm, postoperative 2.17 mm±1.58mm, p<.05). For one subject (14%), the deviated side was changed after orthognathic surgery. The preoperative position of the Me on the right side (0.48mm) was changed to the left side (1.69mm) by surgery. The spherical coordinates of the facial lines were evaluated before and after surgery (Figure 3).
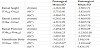
- The spherical coordinates of facial lines of deviated and opposite sides after were compared with those before surgery. The midsagittal inclination angle of mandibular body line on the deviated side wasincreased significantly by surgery (presurgical 25.04°±3.65°, postsurgical 30.67°±4.3°, p<.05). Length of mandibular body line on the opposite side was decreased by surgery (presurgical 103.33mm±8.96mm, postsurgical 94.20mm±8.72mm, p<.05)(Table 2).
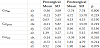
- The amount of asymmetry of length (dv) of ramal height line, ramal lateral line, ramal posterior line and mandibular body line were –1.26 mm±2.08mm, -0.24 mm±2.44mm, -2.49 mm±4.53mm, -3.62 mm±5.11mm before surgery and –1.38 mm±2.72 mm, –5.46 mm±9.80mm, -2.96 mm±6.09mm, 1.64 mm±5.56mm after surgery (Table 3).
- The amount of asymmetry of midsagittal inclination angle (dθ) of ramal height line, ramal lateral line, ramal posterior line and mandibular body line were 5.77°±5.40°, -0.24°±2.44°, –3.80°±6.23°, –7.65°±5.67° before surgery and –3.62°±4.05°, -3.60±5.54°, –5.23°±10.08° –1.19°±4.64° after surgery. The amount of asymmetry of midsagittal inclination angle (dθ) of mandibular body was significantly changed by surgery (presurgical –7.65°±5.67°, postsurgical -1.19°±4.64°, (p<.05)) (Table 3).
- The amount of asymmetry of coronal inclination angle (dϕ) of ramal height line, ramal lateral line, ramal posterior line and mandibular body line were –3.39°±2.51°, -2.59°±3.29°, -1.89°±7.85°, 0.30°±2.48° before surgery and –2.52°±3.72°, –9.20°±7.50°, -2.33°±5.50°, 0.45°±2.91° after surgery(Table 3).
- There was no statistically significant difference inbilateral differences (dx,dy,dz) of starting points, Goinf ,Golat and Gopost after surgery with those before surgery (Table 4).


4. Discussion
Orthognathic surgery is generally performed to correct facial abnormalities related to maxillar and/or mandible [22].In spite of possible complications [23], many patients seek orthognathic surgery for esthetic improvement. Subjects with skeletal malocclusion are often affected by three-dimensional problems and may have clinically noticeable asymmetry [24]. The skeletal asymmetry after surgery has been rarely studied. A case report showed that skeletal asymmetry remained after surgery in a different form from that before surgery [13]. This study aims to analyze the amount of asymmetry of facial lines before and after orthognathic surgery using spherical coordinate system on 3D CT.
In this study, all spherical coordinate of facial lines changed after surgery. In particular, the midsagittal inclination angle of mandibular body line on the opposite side was significantly decreased by surgery (presurgical 103.33mm±8.96mm, postsurgical 94.20mm±8.72mm, p<.05) (Table 2).
Although the amount of asymmetry of the facial lines was changed by surgery in all the subjects, only the amount of asymmetry of midsagittal inclination angle of mandibular body line was significantly changed (presurgical –7.65°±5.67°, postsurgical -1.19°±4.64°, p<.05) (Table 3). The menton deviation was significantly reduced by surgery (preoperative 7.67mm±4.46mm, postoperative 2.17mm±1.58mm, p<.05). It showed that orthognathic surgery may recover facial symmetry by repositioning of the Me which is an index to classify facial asymmetry [13,19,20].
However, none of the amount of asymmetry of the facial lines changed to zero by surgery. This result was consistent with previous reports that some level of asymmetry can remain even after orthognathic surgery [13,15,18,21]. Jung et al. [18] reported that surgical results of facial asymmetry correction seemed to be clinically acceptable. However their research dealt only the landmarks of the midfacial area. This study showed that even when the menton deviation was significantly reduced by surgery, facial lines except mandibular body line remained significantly asymmetric. Through this study, it might be considered that mandibular body line significantly contributes to the improvement of facial asymmetry rather than the other facial lines (Table 3).
5. Limitations of this Study
The limitations of this study were a small number of subjects and lack of analysis in soft tissues. In conclusion, the position of menton was repositioned by orthognathic surgery, and the length and position of the mandibular body line was changed with statistical significance. Facial asymmetry may remain after surgery even with attempts to correct asymmetry by reducing the menton deviation.
Competing Interests
The authors declare that they have no competing interests.
Author Contributions
All the authors substantially contributed to the study conception and design as well as the acquisition and interpretation of the data and drafting the manuscript.