



1. Introduction
The incidence of fall-related accidents is rising annually due to the increase in the aging population. Falls cause significant mental and physical problems that require a lengthy recovery period. Preventing falls can lead to the improvement of the quality-of-life (QOL) of older adults and reduce medical costs.
Previous studies have reported that lateral balance is important for preventing falls [1-3]. It is also related to falls in older adults [4]. Robinovitch reported that a lateral impact on the greater trochanter can lead to hip fractures in elderly patients [5]. The center of gravity (COG) is needed to maintain a stable standing posture and for returning to the central position of the limit of stability (LOS) when the COG is about to move out of the LOS. If the patient properly shifts his or her weight or finds a new base of support by taking a step, COG is maintained inside the LOS. However, the most frequent reason for falls during daily activities is incorrect weight shifting[6]. Therefore, a self-generated perturbation, such as a volitional side step in the lateral direction, should be investigated to determine whether it can prevent falls.
Proper crossing motion is needed to avoid stumbling on obstacles or stairs. However, it is difficult for elderly people to do crossing motions owing to their deteriorating sensory ability, spatial perception, and coordination. If they cannot raise their leg or foot as intended, they can trip and fall over. Important factors for achieving intended motion are motor and sensory functions. The constant feedback from the sensory system and a strong musculoskeletal system contributes to this motion. Crossing motion (volitional step) requires not only peripheral function (i.e. sensory and musculoskeletal system), but also a complex central neural system including the anticipatory postural control [7]. Sparto et al. reported that postural responses in older adults are variable, compared with young adults [8]. Caetano et al. reported that older adults were less accurate when performing stepping motions [9]. Therefore, it is necessary to clarify the characteristics of variable and inaccurate motion in older adults from a kinematical stand point. Consistent foot motion is needed to achieve clearance from an obstacle during the crossing motion.
The purpose of this study was to analyze foot motion during the volitional step of older adults. Moreover, we investigated the relationship between step motion and sensory function.
2. Methods
2.1 Subjects
The subjects were 18 healthy older adults (9 men and 9 women; age: 70.8 ± 3.2 years; height: 160.1 ± 7.3 cm; weight: 56.5 ± 10.2 kg) and 22 young adults (15 men and 7 women; age: 20.2 ± 0.3 years; height: 166.5 ± 5.4 cm; weight 58.4 ± 9.1 kg). The subjects had no neurological disorders or orthopedic history with respect to their lower limbs. Subjects were provided a carefully written explanation of the experimental purpose, method, and privacy protection in advance of the experiment. They submitted their written informed consent to participate in this study. This study was approved by the Ethical Committee of Mejiro University.
2.2 Procedure
The subjects were asked to cross over a lateral obstacle with unrestricted motion velocity and landing position. They crossed their arms in front of their chest and looked at a target on the wall. They were asked to try not to look at their feet. They tried to repeat this motion 10 times and were asked to keep each motion as consistent as possible with the last. They practiced several times and decided on the landing position of the foot. The height of the obstacle was 20% of the subjects’ heights. The obstacle consisted of a wood and iron pipe.
We conducted a sensory test to examine the position sense of the right knee. Subjects lay on their stomach, while the examiner held their right lower leg and stabilized the knee joint up to target angle. Subjects flexed their left knee, similar to right knee flexion, while the examiner held up the right knee. The differences between the angles of the right and left knee were recorded. The target angles were 20°, 40°, 60°, and 80°. The position sense test was conducted 3 times for each target angle.
2.3 Experimental set up
Crossing motion was recorded using a three-dimensional analysis system (DKH Co. Ltd., Japan). Reflective markers 14-mm in diameter were placed on the right side of the anterior superior iliac spine, the greater trochanter, knee joint center, the lateral malleolus, the heel, and the head of the fifth metatarsal. Two video cameras were used for motion analysis. The sampling rate of the cameras was 100 Hz.
An electrical goniometer was used to examine the knee angle. The proximal part of the goniometer was attached to the lateral thigh along the axis (great trochanter knee center). Similarly, the distal part was attached to the lateral part of the lower leg (fibula). A measurement of zero degrees was defined as fully extended. All the equipment was synchronized and operated simultaneously.
2.4 Data analysis
Frame-Dias (DKH Co. Ltd., Japan) was used to analyze knee motion and heel trajectory. The angle changes of the knee and heel motion were calculated using a time-series analysis.
The average of trajectory curves of heel and angle change of knee motion were calculated by analyzing the degree of coincidence between the ten trials using the following methods by MATLAB (Math works, Inc. USA). First, the start and end points of the curve were defined as the moment that the heel was off the ground and made contact, respectively, and normalized from 0 to 1. To calculate the average trajectory of the curves, the curves were approximated using cubic spline function, and the data were resampled at regular intervals. Figure 1 shows the method of calculation or the sum of error distance of the heels. The sum of the error angles of the knee angle were analyzed using the same method.

The peak time was defined as the time between the taking off of the motion leg to the top of the trajectory, and it indicated the percentage.
Errors from the target angle were recorded in each angle (20°, 40°, 60°, and 80°) of the sensory test. The average of errors among the three trials was used.
2.5 Statistical analysis
The differences in each parameter of sum of error distance, peak time, and sensory test between two groups were compared using the t-test. A p value of < 0.05 was considered statistically significant. All statistical analyses were conducted using SPSS 20.0 software (SPSS, Tokyo, Japan).
3. Results
Table 1 shows that the peak times of the motion of older adults were statistically shorter than that of young adults (p <0.05). Table 2 shows the sum of error distance in older adults and was statistically larger than that of young adults (p <0.05). Table 3 shows that the error of angle had no statistical significance. Table 4 shows the error of sensory test of each target angle and had no statistically significant difference.
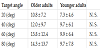
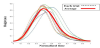
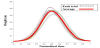
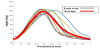
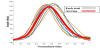
Figure 2-6 show the trajectory of heel markers of a typical older and younger adult, respectively. Each figure shows all 10 trial trajectories.

4. Discussion
The sum of error distance results showed that the foot motions during the steps of older adults are inconsistent. We believe that as sum of error distance increases, the consistency of the motion decreases. Therefore, the crossing motion in older adults may vary widely and lack accuracy. In addition, we believe that motion may change due to aging.
Well-controlled concentric and eccentric contraction, especially of knee joint, should be used for this type of consistent motion. Sensory and motor function and the coordination of many muscles are needed to achieve this motion. One of the most important parts of the sensory system may be proprioception of the knee joint during consistent crossing motion. In a previous study, researchers found that proprioceptive signals encode joint angles [10]. However, these functions generally deteriorate in older adults. We did not observe a decline of proprioception of the knee joint and inconsistency of knee angle during motion, respectively, according to the results of the sensory test and sum of error angles. A slight decline of proprioception could not be detected through the clinical sensory examination of knee joint of older adults. In terms of motor function, eccentric motions are more complex and difficult to control compared to concentric contractions, especially for older adults [11]. However, the force of eccentric contraction is maintained in older adults [12]. Therefore, we believe that older adults are less able to adjust their intended contraction force. This decline may be related to the inconsistencies we observed in their motion and may cause falls. Therefore, exercises that improve accuracy and coordination are needed to prevent falls in older adults.
Furthermore, we found that the ascending period became short, while the descending period became extended in older adults. Therefore, they would pay more attention to landing than young adults in the descending period. A previous study showed that older adults often step before they need to, and therefore, it is likely that cognitive factors also influence the stepping response as seen in the extended descending phase of our study [13]. They may change their motion as they recognized their deteriorating ability for eccentric contraction. This may be an automatically compensated motion during aging. We believe that the change in motion is difficult in older adults and indicates a compensatory mechanism that is part of aging.
5. Conclusion
We collected the three-dimensional kinematic data of heel trajectory for crossing motion. Older adults performed inaccurate and inconsistent motion compared with young adults. Moreover, their actual physical motion differed from that of young adults. These results indicate that older adults cannot smoothly adjust their motion during eccentric contraction and cannot compensate for their decline in function by changing their motion. It is important to identify changes of motion in elderly patients in the clinic. Rehabilitation to improve coordination is needed in older adults to acquire accurate and stable motion.
Competing Interests
The authors declare that they have no competing interests.