



1. Introduction
The use of lower limb orthosis in hemiplegic patients with stroke promotes active rehabilitation and facilitates quick recovery by improving activities of daily living (ADLs) [1]. The benefits of lower limb orthosis are (1) stability in the stance period, (2) easy toe clearance, (3) almost normal walking pattern, and (4) prevention of deformation [2]. The orthosis allows patients to gain stability in the paralyzed foot and walk with good dynamic balance [3]. The Japanese Guideline for Stroke 2015 [4] recommends the use of orthosis for improving ambulation in hemiplegic patients with equinovarus foot.
In the Kaifukuki Rehabilitation Ward (KRW) a, stroke patients undergo intensive rehabilitation in the early stages after stroke to help decrease impairments in their ADLs, expecting that the rehabilitation will help them recover early [5]
Nevertheless, few reports have provided information on stroke patients who received prescription of orthosis and walked independently. The purpose of the finding is to clarify how much training using orthosis should be carried out for a stroke patient at a rehabilitation hospital. The purpose of the second finding is to investigate how severe the patient is using an orthosis, is to describe the ability to walk at discharge.
2. Patients and Methods
2.1 Patients
A total of 1317 patients with stroke were admitted to our rehabilitation hospital between January 2013 and December 2015 (Figure 1). Patients who had a history of stroke, those who had psychiatric disease, and those who needed any help before stroke were excluded. A total of 1040 patients were finally considered for inclusion. This research was conducted after obtaining approval from the ethics committee of our university, and informed consent was obtained from the patients.

2.2 Methods
Age, sex, etiology, duration from onset to hospitalization, and clinical symptoms were assessed as described below. The severity of paralysis was evaluated using the Brunnstrom recovery stage (BRS) [6]. Language and visuospatial function were assessed using recognition and were further evaluated using the stroke impairment assessment set [7]. In the language function, acceptance and expression aspects of aphasia are evaluated. Dysarthria is not included in this item. In the visuospatial function, the patient is asked to touch the midportion of a tape held horizontally in front at a distance of about 50 cm. Two trials were performed, the larger error is used for scoring, and deviation of 3 cm or more is judged to be abnormal. The mini-mental state examination (MMSE) was used to assess neurological severity and cognitive function[8]. ADLs were assessed on admission and at the time of discharge using the functional independence measure (FIM)[9],which is an 18-item ordinal measure of disability with 13 motor items and 5 cognitive items. With FIM, patients were assessed on each item using a 7-point scale (from complete independence [value = 7] to complete dependence [value = 1]). The walking ability at discharge was assessed using functional ambulation categories (FACs)[10]. This 6-point scale assesses ambulation status by determining the extent of human support the patient requires when walking, regardless of whether or not they use a personal assistive device. The patients were classified as walking independently if the FAC score was 4 (walks independently on level ground but requires assistance with stairs, slopes, etc.) or more.
2.3 Rehabilitation program
KRWa is the main system providing inpatient rehabilitation facilities covered by Japan’s medical insurance system. Stroke patients undergo intensive rehabilitation in the early stages after stroke to help decrease impairments in their ADLs, expecting that the rehabilitation will help them recover early [5]. Physical therapy, occupational therapy, and speech therapy (if needed) were conducted each day as per requirement for 3 units each (1 unit is 20 min; total of 6–9 units). In cases where the patient’s general condition was stable, physical therapy was started in the training room (gym), which included standing exercises, mat exercises, transfer exercises, wheelchair movement exercises, walking exercises, and stair climbing exercises. If the patient’s general condition was unstable, range of motion exercises, positioning, sitting exercises, and standing exercises at the bedside were conducted. Occupational therapy included ADL training, such as using the bathroom, grooming, dressing, and bathing, and arm exercises, such as changing hand dominance. Speech therapy included exercises for dysphagia and exercises for aphasia.
2.4 Orthotic therapy
Immediately after admission, rehabilitation patients are encouraged to ambulate and start adopting a standing position instantly [11-13]. Physical therapy was performed using orthosis for standing or walking (orthosis therapy). An ankle-foot orthosis (AFO) is prescribed to provide additional support to the lower limb for standing and walking, to correct an abnormal position due to spasticity and contracture, and to prevent deformity and contracture [14,15] .
AFOs are categorized as follows: those having metal uprights on both sides (M-AFO), adjustable posterior strut AFOs (APS-AFO), plastic AFOs (p-AFO), and ready-made AFOs (made with silicone or soft plastic). An M-AFO is used in patients with severe paralysis and strong spasticity. Additionally, it is used in cases that require high fixation. An APS-AFO allows adjustment of the fixation by changing the rear props to aluminum or carbon. Moreover, the attached tool can be used to adjust the angle of the ankle so that AFO can be used by a wide range of patients (from server to mild paralysis). A p-AFO is lighter and cheaper that the other AFOs; however, fixation is low. Therefore, it is used in patients with relatively low paralysis and spasticity. A ready-made AFO is used in patients with drop foot and mild equinovarus foot, as well as mild spasticity (Figure 2). Clinical indication between APS-KAFO and M-KAFO is the same; however, if weight of the patient exceeds 80 kg, APS will be out of the indication. There are some M-KAFOs for practice in gym. Patients use M-KAFO for standing up and walking exercises, except for the patients who had APS-KAFO from a previous hospital.
A knee-ankle-foot orthosis (KAFO) is prescribed when (1) the patient’s general condition has stabilized and the patient is able to undergo standing or walking training, but the knee and ankle joints are unstable due to severe paralysis; (2) the patient exhibits spasticity patterns predominantly in the flexor muscles and cannot hold the knee in the extended position; and (3) the patient displays abnormal knee joint movements, such as flexion contractures of the knee joint [16,17] . Walking training is conducted for patients who show improvement in standing balance when wearing KAFO, even if the side of the affected limb is severe and the balance is bad. A traditional KAFO (M-KAFO) is equipped with bilateral metal struts, ring lock knee joints, and double Klenzak ankle joints. It can be used as an AFO by removing the portions for the knee joint and thigh [18]. An APSKAFO consists of a foot section, a shank, hinge joints, a posterior strut, and a leg cuff, while the thigh portion consists of inner and outer struts, ring locks, an added knee joint, and a thigh cuff (Figure 2).

The knee and ankle joints of the orthosis are adjusted as needed, and if support with the affected lower limb can be achieved and walking is possible without fixing the knee joints, the orthosis is modified (cut down) to an AFO by removing the thigh cuff.
An M-KAFO, M-AFO, APS-AFO, and p-AFO are available for orthotic therapy in the gymnasium, and physiotherapy using an orthosis is performed until the completion of patient’s own orthosis. In all the subjects, the effect of the prescribed orthosis was verified and confirmed by a responsible physician.
Patients were divided into the following 3 groups according to orthosis used in physical therapy immediately after hospitalization: the KAFO group, AFO group, and no orthosis group. We investigated the differences in orthotic therapy, background factors of the patients, neurological symptoms, and cognitive function.
The prescribed orthosis, number of days from admission to the completion of orthotic therapy, and type of orthosis at discharge were investigated. In addition, we examined the relationship between orthotic therapy and walking ability at discharge.
The chi-square independence test was used to assess the independence of two factors. The Kruskal–Wallis testwas used to determine associations between the group sample data, and the Steel– Dwass test was performed for comparison between the individual groups. Statistical analyses were performed using JMP 12.2.0 (SAS Institute Inc., Cary, NC, USA), and significance was set at a P-value <0.05.
3. Results
This study included 1040 patients (539 with cerebral infarction, 402 with cerebral hemorrhage, and 99 with subarachnoid hemorrhage; 649 male and 391 female patients), and the patients were aged between 12 and 94 years (mean age, 66.5 ± 13.4 years). The mean period from the onset of symptoms to hospitalization was 34.1 ± 17.8 days, and the hospitalization duration was 63.7 ± 35.6 days. Among the 1040 stroke patients who were admitted to our rehabilitation hospital, 414 received orthotic therapy, and of these, 220 were included in the KAFO group and 194 were included in the AFO group. Among the patients who received orthotic therapy, 10 had orthoses from previous hospitals (9 were KAFOs [all M-KAFO] and 1 was an AFO [APS-AFO]).
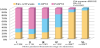
On comparing the KAFO, AFO, and no orthosis groups, no differences were seen in sex and the duration of onset; however, there were differences in age, etiology, neurological symptoms, cognitive function, duration of hospitalization, the FIM score, the walk independence at discharge, and proportion of patients who were discharged among the groups (Table 1). Age of the patients was lower in the AFO group than in the no orthosis group, while neurological symptoms and cognitive function were more severe in the KAFO group than in the other groups. Patients with aphasia and/or neglect who received orthotic therapy were more common than patients without these conditions. On assessing the relationship between motor paralysis and orthotic therapy on admission, we found that 80% of severe hemiplegic patients with below BRS III underwent orthotic therapy (Figure 3). The KAFO group included majority of patients with BRS Iand II, while the AFO group included many patients with BRS III. Majority of patients with BRS IV received orthotic therapy, and most of them were in the AFO group.

Among the 220 patients in the KAFO group, their own KAFO was prescribed in 155 patients (M-KAFO, 128; APS-KAFO, 27) and their own AFO was prescribed in 62 patients (APS-AFO, 41; M-AFO, 6; P-AFO, 15). Among the 194 patients in the AFO group, their ownAFO was prescribed in 186 patients (APS-AFO, 53; M-AFO, 98; p-AFO, 37). In the no orthosis group, seven patients were prescribed their own AFO (all p-AFO). The mean period from hospitalization to completion of orthosis was 11.7 ± 5.3 days in the KAFO and 33.9 ± 20.9 days in the AFO.
At the time of discharge, 95 of 156 patients who were prescribed KAFOs were able to switch to AFOs and 14 did not require orthoses. Additionally, 38 of 260 patients who were prescribed AFOs did not require orthoses at discharge. A total of 47 KAFOs (all M-KAFO) and 328 AFOs (M-AFO, 98; APS-AFO, 152; and p-AFO, 78) were necessary for patients during discharge from the hospital.
There were significant differences in age, sex, etiology, the duration from onset, neurological symptoms, cognitive function, duration of hospitalization, the FIM score, walk independence at discharge, and proportion of patients who were discharged among the orthosis at discharge (Table 2). At the time of discharge, 660 patients (63.5%) could walk independently. Of them, 197 patients were necessary for AFOs during discharge from the hospital. These patients included 43.2% (95/220) of patients from the KAFO group and 66.5% (129/194) of patients from the AFO group.

4. Discussion
In this study, most patients transferred to our rehabilitation hospital were undergoing rehabilitation at acute hospitals; however, only 10 of 1040 patients (1%) were prescribed orthoses. The reasons were (1) no rehabilitation physician was available in the previous hospital, (2) rehabilitation was not the main treatment approach in the acute hospital, (3) the orthosis could not be prepared on time, (4) preparation of the orthosis depended on the rehabilitation hospital, etc. Very few reports have clarified the ratio of orthosis prescription to stroke patients. Masuda et al. [19] reported that orthoses were prescribed in 63 of 573 stroke patients (11.0%) (KAFO, 36; M-AFO, 2; p-AFO, 36) in acute phase hospitals. A lower limb orthosis is often used because the reason for admission to a rehabilitation hospital among most hemiplegic patients is gait exercise. Akebi et al. [20] prescribed a lower limb orthosis in 132 of 386 stroke patients (34.2%) who needed rehabilitation (36 KAFOs and 96 AFOs).
In this study, orthoses were prescribed in 40% of patients, and this appeared to have a great influence on the days from stroke onset, the medical condition, and the neurological severity of the patient. In particular, many of the patients transferred to a rehabilitation hospital need orthotics due to severe hemiplegia.
Tyson et al. [3] showed that AFO improves walking ability, gait speed, and balance after stroke. Momosaki et al. [21] suggested that stroke survivors had better functional recovery if they were prescribed an AFO than if they were not prescribed an AFO. Nikamp et al.[22] also described positive effects of providing AFO in subacute stroke patients who had not used these orthosis before from a randomized control trial.
Furthermore, walking training is possible with KAFOs for patients with severe paralysis.KAFOs for hemiplegia in stroke patients have been used since the prewar time in our country [23], but orthotic therapy for gait training has only been performed in the recent 30 years [17]. A KAFO is a knee joint and femoral cuff attached to an AFO. Even if hemiplegia is severe, KAFO provides good support, and therapists and family members can easily assist the patient during walking [11-13]. As our hospital has many lower limb orthoses for training and evaluation, they can be used for standing and walking training from the beginning of hospitalization. Among the patients who started training using KAFO, many patients were indicated for an AFO when prescribing an orthosis. Indeed, at the beginning of the training, 220 were trained using KAFO and 194 were trained using AFO, while 155 had been prescribed KAFO and 248 had been prescribed AFO. In particular, although orthotic therapy was started with KAFOs, about 60 patients had been prescribed AFOs, as recovery of physical function and ability improvement were quite significant. Thus, walking training was performed using orthoses for evaluation in the gymnasium, and the days from hospitalization to completion of orthosis was longer for KAFO than for AFO.
In addition, when it is not possible to decide whether an AFO is necessary for walking, the preparation of the orthosis can be delayed, and it appears that this could prolong the period until the completion of orthosis with AFO. During hospitalization, the femoral cuff of KAFO can be removed and KAFO can be converted into an AFO in many cases. About fifty patients who were discharged from the hospital while using KAFO had difficulty in walking. However, it is useful not to use the KAFO for the purpose of only walking training, but also to use for standing training. Indeed, more than 40% of patients who used KAFO during commencement of orthotic therapy could walk independently. Alternatively, more than 60% patients who used AFOs during commencement of orthotic therapy could walk independently.
In our study, many patients who needed orthotic therapy had severe neurological deficits, including aphasia and neglect. The walking ability of a patient with hemiplegia might be related to aphasia and neglect; therefore, it will be necessary to verify this in future studies. From these observations, we believe that it was clear that orthosis therapy is indispensable for rehabilitation of stroke patients.
5. Conclusion
In conclusion, we clarified the use of orthotic therapy and the ability to walk at the time of discharge from hospital among stroke patients.
aKaifukuki Rehabilitation Ward (KRW): In Japan, rehabilitation is conducted at the convalescent stage based on the medical insurance system. Inpatient treatment is carried out for a maximum of 6 months in rehabilitation hospitals for strokes, starting within 2 months of onset. During this time, remuneration for medical treatment can be calculated for up to a total of nine 20-min units (3 h) per day of physical, occupational, and speech therapy.
Competing Interests
The authors declare that they have no competing interests.
Author Contributions
Shinichiro Maeshima analysed clinical data and drafted the manuscript. Sayaka Okamoto, Hideto Okazaki and Shigeru Sonoda participated in the study design and helped to draft the manuscript. Reisuke Funahashi, Kei Yagihashi, Hirokazu Hori, Shigenori Hiraoka, Shinichiro Tanaka, Ikuko Fuse and Naoki Asano participated in the medical examination. All authors read and approved the final manuscript.