


The study of gastroesophageal reflux disease uses three main diagnostic methods, as well as some secondary ones.
The main ones are:
- Esophageal gastroduodenoscopy
- 24-hour pH-impedance
- High Resolution Esophagael Manometry (HRM)
Esophageal gastroduodenoscopy evaluates mucosal damage and the possible presence of hiatal hernia. With this procedure a diagnosis is not always made due to the high percentage of reflux disease without esophageal lesions (NERD: Non Erosive Reflux Disease). Thus, it should not be repeated frequently (except in the case of pre-cancerous lesions: BARRET’s Esophagus).
The 24-hour pH-impedance (MII-pH-Multichannel Intraluminal Impedance and pH) is currently considered the most reliable method (gold standard) in detecting gastroesophageal reflux. It recognizes any reflux episode and defines its composition (acid, weakly acid, basic, neutral), duration, location and nature (solid, liquid, gaseous, mixed). This exam is an important evolution in 24-hour Esophageal pH monitoring.
pH monitoring has significant limits:
- Acid esophageal reflux is identified only with each drop in pH below level 4.
Generally, the cut off point for reflux is considered when the pH rises above level 4
- It is unable to determine the height of the refluxate in the esophagus.
Therefore clinically symptomatic patients may have a negative pH monitoring.
DeMeester score
Revision as of 13:53, 8 November 2009 by Mlj (Talk | contribs)
(diff) ← Older revision | Latest revision (diff) | Newer revision → (diff)
Measure of lower oesophageal acidity and therefore a surrogate of severity of gastro-oesophageal reflux. A score of >14.72 shows significant reflux.
Based on 6 parameters (scored in comparison to mean values in normal subjects for each category below):
- Supine reflux
- Upright reflux
- Total reflux
- Number of episodes
- Number of episodes longer than 5 min
- Longest episode
These issues have been overcome by the 24-hour ph-impedance monitoring. The exam involves introducing a catheter of about 1mm in diameter transnasally (procedure usually takes a few minutes). The catheter must be positioned 5cm above the Lower Esophageal Sphincter (LES) and left in place and connected to a portable recorder for 24 hours. During the exam, the patient will carry on with their regular daily activities (even going to work) and will record meal times, any symptoms, position (orthostatism, clinostatism). A catheter with a pH sensor (sometimes 2) and six channels measuring the electrical impedance is transnasally introduced.
1. Impedance
- is the inverse of conductivity
- varies with the chemical and physical nature of the bolus
- displays direction and transit of the bolus (including refluxes and gas)

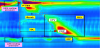
The impedance is measured by the instrument and its value changes with the passage of the bolus and reflux, identifying its “direction”. In having the 6 channel Impedance Catheter, the exam allows the detection of the reflux exposure time and height in the esophagus, critical data from a clinical and therapeutic point of view.
To sum up, the combined pH and impedance measurements have allowed the classification of new reflux categories which are undetectable through just pH-monitoring.
- Acid reflux (pH < 4 as with pH monitoring exams)
- Repeated and proximal acid reflux while the pH is < 4, normally recognized as the only reflux episode in pH monitoring
- Weakly acid reflux with pH > 4 but < 7
- Nonacid reflux with pH > 7
The pathophysiology of the first part of the digestive tract includes the study of the pharyngeal motility, the esophagus and its sphincters (Upper Esophageal Sphincter - UES and Lower Esophageal Sphincter - LES).
The HRM (High Resolution Esophageal Manometry), using state-of-the-art probes, makes it possibile to provide immediate information, all at once, about the entire upper digestive tract. This new technology, under the new “Chicago Classification”, provides precision and ease of diagnosis never achieved before.
The High Resolution Esophageal Manometry exam is performed by the transnasal introduction of a catheter with a number of sensors ranging from 24 to 36, depending on the technology. This allows for a complete study of the swallowing phase while keeping the probe in the same position, with the result of obtaining:
- Complete and coordinated results of all degenerative and peristaltic activity.
- Faster exam performance.
- Greater acceptance of the exam by the patient.






We know that GERD is a disease that essentially stems from a motility disorder. GERD is, therefore, linked to functional alterations of the mechanisms that usually prevent gastroesophageal reflux.
The most frequent functional alterations are
- Reduction of the basal tone of the Lower Esophageal Sphincter (LES)
- Spontaneous transient releases of the LES
- Delayed gastric emptying, resulting in increased intragastric pressure
- Alterations in esophageal peristalsis, which causes reduced ability in the cleaning of refluxed material.
The LES pressure tone is almost always below 10 mmHg.
The amplitude of peristaltic contraction is more or less reduced in patients suffering from gastroesophageal reflux disease. Reflux occurs when the amplitude of the contractile wave is not sufficient enough to trigger the closure of the lumen upstream from the bolus and there is a reduction in pressure in the LES. Furthermore, patients with GERD exhibit a greater proportion of ineffective peristaltic contractions. As the inefficiency of the peristalsis may be frequent, no contraction begins after voluntary swallowing. Even non propagated or simultaneous peristaltic waves are proportionately linked to the severity of the disease.
2. Conclusion
The 3 first-choice diagnostic techniques in GERD are
- Endoscopic exam. It is irreplaceable in ascertaining the existence and the severity of esophagitis and its complications.
- pH-impedance monitoring. It is the most reliable method in detecting GERD as it can recognize any reflux episode and define its composition, duration, localization and pH.
- HRM Esophageal Manometry: It allows the study of the functional motility alterations that are at the base of the prevention of gastroesophageal reflux.
To sum up
- Endoscopic exam: assessment of mucosal damage by GERD.
- pH-impedance monitoring: Evaluation of the entity and type of reflux.
- HRM Esophageal Manometry: Evaluation of motility alterations.
This does not mean that every patient with episodic or sporadic symptoms should be subjected to 24-hour pH-impedance monitoring and HRM Esophageal Manometry.
The elective guidelines (gold standard) of these complementary methods are:
- Study of symptomatic patients, endoscopically controlled, with negative exam (NERD);
- Study of patients endoscopically controlled with therapyresistant symptoms;
- Study of patients with atypical or extra-esophageal symptoms (such as pharyngitis, rhinitis, cough, asthma, retrosternal pain, etc..)
- Study of patients in which surgical treatment for gastroesophageal reflux disease is indicated.
Competing Interests
The author declare that there is no competing interests regarding the publication of this article.