


1. Introduction
Cervical cancer is the 10th most common female cancer in Singapore [1] , with about 190 cases diagnosed every year. Approximately 130 cases of cervical cancer are diagnosed each year in our institution, KK Women’s and Children’s Hospital, of which 10% are Stage IIA. Cervical cancer is staged clinically in our institution, using the International Federation of Gynecology and Obstetrics (FIGO) staging criteria.
In light of studies suggesting that tumor size is a prognostic factor for Stage IIA cervical cancers, FIGO revised the cervical cancer staging criteria [2] , subdividing stage IIA into stages IIA1 and IIA2, based on tumor size (<= 4 cm and >4cm) in 2009.
Subsequently, several studies have attempted to validate the changes in the FIGO staging criteria, but with varying results. This study aims to determine if the new sub-staging has any impact on overall survival, as well as to elucidate any other prognostic factors and treatment patterns in this category of patients at our institution.
2. Materials and Methods
This was a retrospective cohort study conducted in KK Women’s and Children’s Hospital, a large tertiary institution in Singapore. The sample consisted of all women who were diagnosed with FIGO Stage IIA cervical cancer from 1st January 2001 to 31st December 2005. The medical information required was retrieved from the KK Gynecological Cancer Centre Database as well as patient records.
The inclusion criteria included 1) tumor histology of squamous, adenocarcinoma or adenosquamous, 2) documented clinical tumor size, and 3) patients who received primary treatment in KK Hospital. Primary treatment included either radical hysterectomy (RH) or radiotherapy (RT), with or without, concurrent chemotherapy.
At our centre, Stage IIA cervical cancer patients who have undergone primary RH are considered for adjuvant therapy depending on surgical pathological information. In the presence of positive lymph nodes, parametrial involvement and positive surgical margins, postoperative radiation with concurrent chemotherapy is given to reduce the risk of both local and distant failure [3] .
In the group of patients considered to be of “intermediate” risk, as identified by Delgado et al. from Gynaecology Oncology Group (GOG), i.e. without the above the above adverse factors but with bulky disease, deep stromal invasion and lymphovascular space invasion, it is thought that adjuvant radiotherapy may be beneficial. The GOG score is calculated by multiplying the relative risks assigned for factors such as tumor size, capillary or lymphatic space involvement and depth of invasion [4] . Based on the score obtained, patients would be recommended either observation, small field radiotherapy or standard field radiotherapy [5] .
The patients were retrospectively assigned using the 2009 FIGO staging criteria to IIA1 and IIA2. The clinico-pathological factors analyzed include patient demographics, histology types, grade of tumor, tumor size, lymphovascular space invasion, lymph node status, type of primary treatment modality and adjuvant treatment. Characteristics between stage IIA1 and stage IIA2 were compared with the Pearson x2 test.
Overall survival and disease free interval were calculated using the Kaplan-Meier method. Cox regression hazard model was used to determine the prognostic factors. The statistical analysis was performed using SPSS version 19.
3. Results
A total of 66 patients were diagnosed with Stage IIA cervical cancer between 2001 and 2005. Of the 50 patients who met the inclusion criteria, 35 (70%) had Stage IIA1 and 15 (30%) had Stage IIA2 cervical cancer. See Table 1 for patient demographics. None of the patients were lost to follow-up.

The mean age at diagnosis was 55.8 years and the patients who had Stage IIA2 were younger than those with Stage IIA1 though this was not statistically significant (p=0.12). The majority of the patients were Chinese (90%) and the most common tumor histology was squamous cell carcinoma (80%).
A total of 23 patients (46%) underwent primary RH, of which 16 were Stage IIA1 and 7 were Stage IIA2. A total of 27 patients (54%) underwent primary RT, of which 19 are Stage IIA1 and 8 are Stage IIA2. There was no significant difference between the two groups in terms of primary treatment modality (45.7% Stage IIA1 vs 46.7% Stage IIA2 underwent primary RH, p=0.50).
Among the patients who underwent primary RH, the lymph node metastases were found in 52% (12/23) of patients. However there was no statistically significant difference in lymph node metastases between Stage IIA1 and Stage IIA2 (50 % vs 57%, p=1.0). Almost all the patients (95.7%) who had primary RH received adjuvant radiotherapy. This was not significantly different between Stage IIA1 and Stage IIA2 (93.8% vs 100%, p=1.0).
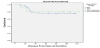
The 5-year overall survival (OS) was not significantly different between Stage IIA1 and IIA2 (79.6% vs 73.3%, p=0.9) (Figure 1). Likewise, the progression-free survival was not significantly different between Stage IIA1 and IIA2 (76% vs 80%, p=0.86) (Figure 2).

However, patients who underwent primary RH performed better compared to those treated by primary RT or concurrent chemoradiotherapy (87% vs 69.6%, p=0.043).
Cox regression analysis showed that age, tumor grade, histology types, tumor size and lymph node status were not independent predictors of survival.
4. Discussion
In 2007, Horn et al. [6] showed that tumor size, defining bulky disease as tumors larger than 4 cm, is of prognostic impact in FIGO stage II cervical carcinomas. This study showed that patients with tumors >4cm showed an increase of recurrent disease compared to tumors < or = 4cm (40.2% vs. 28.0%; p=0.045). The 5-year OS rate was also significantly lower (67.7% vs. 49.5%; p=0.0015) in patients with tumors >4cm. In multivariate analysis, tumor stage, pelvic lymph node involvement and maximal tumor size were independent prognostic factors. All 245 patients with Stage IIA or IIB in this study underwent upfront surgery, but this is not routinely performed in many centres around the world where radiotherapy is the standard treatment for most cases of Stage II cancers. Nevertheless, the FIGO classification of Stage IIA was revised to Stage IIA1 and IIA2 in 2009.
Our study did not find any difference in progression-free or 5-year OS based on the 2009 FIGO sub-staging of IIA1 and IIA2. Similarly, in a study of 560 patients with Stage IIA cervical cancer (data extracted from SEER database from 1988 to 2005; 271 with Stage IIA1 and 289 with Stage IIA2 disease) by Garg et al7, no significant difference in survival was found. The 5-year OS was 65.8% in Stage IIA1 vs 59.5% in Stage IIA2 (p=0.2). Likewise, in a study by Lai et al8, which included 51 patients with Stage IIA cervical cancer (36 with Stage IIA1 and 15 with Stage IIA2 disease), there was no significant difference in survival between the two groups (86.3% vs 51.9%, p=0.218). In these studies, primary treatment included either RH or RT.
In another recent study, Hongladaromp et al. [9] looked into 133 patients with Stage IIA cervical cancer, 101 (75.9%) Stage IIA1, and 32 (24.1%) Stage IIA2. All of these patients were treated with RH and pelvic lymphadenectomy. There were comparable rates of 5-year disease-free survival (84.6% vs 88.7%, p=0.67) and 5-year OS (83.4% vs 90.0%, P=0.49). The authors hence concluded that the revised 2009 FIGO staging system did not demonstrate significant survival differences between Stage IIA1 and Stage IIA2 cervical cancer.
On the other hand, Wagner et al. [10] demonstrated in a larger study of 857 patients with Stage IIA cervical cancer (data extracted from SEER database from 1988 to 2008), that patients with Stage IIA1 disease had improved cause-specific survival (CSS) compared to patients with Stage IIA2, with 5-year CSS's of 84% and 69% respectively (p<0.0001). Mean survival times were 146 months for Stage IIA1 compared to 73 months for Stage IIA2 (p<0.0001). This supports the changes made to cervical cancer staging 2009. It is likely that Wagner et al’s results differed from the other studies due to several reasons, such as the larger number of patients included, as well as the use of CSS, instead of OS, as the primary endpoint of analysis, hence reducing the risk of other confounding variables.
Garg et al. concluded that age, tumor size and lymph node status were independent predictors of survival and Wagner et al concurred that age was significantly and independently prognostic. On the other hand, this was not shown by Lai et al, nor in our study. This is likely due to the smaller numbers in the latter studies. Moreover, at our centre, clinical staging is routinely performed via examination under anesthesia. Tumor size is measured clinically and not dependent on radiology, which is more reflective of what is recommended in the FIGO clinical staging criteria.
In terms of treatment modalities, Stage IIA cervical cancer is treated with either primary RH or RT with or without concurrent chemotherapy. Primary surgical treatment allows preservation of sexual function and ovarian conservation, avoids the late side effects of radiotherapy, and is hence preferred in younger patients. The decision on primary treatment is dependent on the policy of the institution, gynecological oncologist, radiation oncologist, age and general health of the patient. Our study shows that only age at diagnosis was found to be a significant predictor of primary surgical treatment (p=0.009) and RHs were more commonly performed in younger patients below the age of 60.
Patients who underwent primary RH in our study were found to perform significantly better compared to those treated by primary RT (5-year OS 87% vs 69.6%, p=0.043). This was likely due to the fact that 95.7% of patients who underwent primary RH in our study received adjuvant treatment with RT or concurrent chemo-radiotherapy (p<0.05), based on the postoperative GOG score. It is important to be mindful that patients who undergo primary RH, followed by adjuvant RT with or without chemotherapy, are subjected to complications of both treatment modalities hence increased morbidity11. Further studies are needed to aid in streamlining the selection of patients for each treatment arm, so as to decrease morbidity and improve quality of life after treatment.
On the other hand, the study by Garg et al showed that there was no significant difference in survival between patients treated by surgery and radiotherapy (p>0.05), with 67.3% of patients being administered adjuvant radiotherapy. However, the incidence of the use of concurrent chemo-radiation as adjuvant therapy was not reported. Similarly, Lai et al. did not show statistical significance in the survival between the different treatment modalities. This may be due to the limited number of patients with Stage IIA2 disease in this study (36 Stage IIA1 vs 15 Stage IIA2), a higher proportion of 71% of patients undergoing primary RH, and also the lack of information on types of RH and details of chemotherapy. The study by Wagner et al was unable to evaluate the benefit of different treatment modalities, as complete details on surgery, radiation and chemotherapy were not available.
5. Conclusions
In conclusion, our study did not find any difference in overall survival based on the new FIGO sub-staging of IIA1 and IIA2 in our local population. However, it is important to bear in mind that this study is small and retrospective, hence it may not have sufficient power to show any difference. Larger prospective studies are needed to confirm our findings.
Competing Interests
The authors declare that they have no competing interests.