


1. Introduction
Cervical dilatation is mandatory before a many gynecological operations as uterine biopsy, operative hysteroscopy, and loop insertion. By far operative hysteroscopy is the most common gynecologic operation requiring cervical dilatation up to 10 mm with multiple insertions and extractions of the operative system. The diameter of the hysteroscope is generally too large to easily pass through the cervix directly, thereby necessitating cervical dilation to be performed prior to its insertion. Cervical dilation can be performed by temporarily stretching the cervix with a series of dilators of increasing diameter [1,2].
Difficulty in cervical dilatation is a complication that is infrequently discussed, despite the fact that almost 50% of hysteroscopic complications are related to difficulty with cervical entry. Potential complications include cervical tears, creation of a false passage, perforation, bleeding, or simply difficulty in entering the internal os with the hysteroscope [3,4].
Many trials were made to facilitate cervical dilatation including preparation of cervix by misoprostol or lamineria tents or balloon catheter given the night prior to procedure. Although these methods were successful in many patients giving little time and effort in cervical dilatation, but these methods were not adequately effective in patients with previous cesarean deliveries and cervical fibrosis or stenosis. Cervical stenosis remains an obstacle for safe hysteroscopic procedures as it requires more time, effort and associated with many complications as cervical lacerations, bleeding or potential cancellation of the procedure [5-8].
Repeated trials of dilatations with vulsellum either single toothed or multiple toothed are associated with cervical trauma, bleeding, surgical team exhaustion and potential cancellation of the procedure.
Vulsellum with relatively large diameter points on the grasping portion frequently cause traumatic bleeding and may require suturing to stop the bleeding. Also, excessive traction on application can pull off cervical tissue causing lacerations and more bleeding. Cervical infections may follow the use of a vulsellum because the vulsellum pierces and compresses the cervix. Moreover considerable cramping and discomfort are often experienced when vulsellum was applied in awake patients [9,10,11].
From these drawbacks we developed a new technique similar to cerclage by applying a nylon or silk suture at the external os to serve as a stable, steady element for traction on the cervix preventing repeated applications and slipping of vulsellum. At the end of procedure the stitch can be removed easily by traction or scissor.
2. Materials and methods
Study design and settings: A prospective randomized controlled study conducted at Tanta University Hospitals in the period from October 1, 2015 to September 30, 2016.
Patients: The enrolled 200 patients were randomly allocated into 2 groups. Group I included 100 patients with application of cervical stitch. Group II included 100 patients with application of traditional vulsellum. Randomization was done by enclosed envelope method with alternate allocation.
Patients were included by the following inclusion criteria: (i) Age between 18 and 49 years, (ii) Patients suffering infertility with uterine lesions as submucous myomas or polyps, and (iii) Patients suffering abnormal uterine bleeding requiring curettage for obtaining biopsy and decreasing blood loss.
Preoperative: 2 tablets of misoprostol equal 400μg were inserted vaginally the night before procedure in all patients.
3. Procedure
In group I: The cervix was grasped by vulsellum and silk suture no. 1 was applied all around the cervix with 4 bites including cervical mucles in a manner similar to McDonald cerclage. The stitch was applied at 1 cm above the level of external os and stretched anteriorly with artery forceps to serve as traction in steed of the vulsellum. Tightening of the stitch could be done easily when leakage of fluid occurred to raise intrauterine pressure improving performance and vision in operative hysteroscopy (Figure 1).

In group II: The cervix was grasped by vulsellum till the end of procedure.
Methods: All demographic data, type of gynecological procedures, time for cervical dilatation and any complications occurred were recorded
4. Outcomes of Study
- Time required to dilate the cervix to 10 mm.
- Intraoperative complications of the procedure including: cervical tears, creation of a false passage, or bleeding.
- The need for additional measures or cancellation of procedures.
Ethical approval: The study was approved by local institutional ethics committee of Tanta University Hospitals.
Statistical methods: All data collected were analyzed by SPSS version 18. The tests used were mean, standard deviation, Chi square and P-value less than 0.05 is considered significant.
5. Results
The enrolled patients were 200 patients allocated in 2 groups with equal number in each group (100 patients). The flow chart was shown in Figure 2.The demographic data of enrolled patients were shown in table 1.

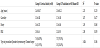
The mean age was 24.5±3.87 years in group I and 25.6±3.21 years in group II with non-significant difference (P value 0.0233). There were no significant difference in gravidity, parity and BMI. The types of procedures were operative hysteroscopy in 144 patients and uterine biopsy for 32 patients (Table 1).
The mean time for cervical dilatation was 10.66±2.70 minutes in group I while it was 18.2±1.45 minutes with significant difference between both groups (P value=0.002). As regard operative complications, there were no cervical lacerations, or bleeding in group I while bleeding occurred in 12 (13.64%) and lacerations of cervix occurred in 68 (77.27%) in group II (Table 2).
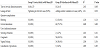
Lacerations and bleeding were managed by additional measures as suturing in 2 cases (2.27%), coagulants were used in 58 cases (65.91%) and vaginal packing was used in 34 cases (38.64%). The cancellation occurredin 3 cases in group II due to cervical stenosis with multiple applications and slipping of the vulsellum and failure to reach 10mm in dilatation resulting in exhaustion of medical staff and occurrence of false tracks (Table 2).
The most interesting data found was that sometimes the cervix was dilated excessively resulting in leakage of fluid from inside the uterus. In this situation the stitch was tightened over the scope in group I [8 cases (9.09%)] preventing leakage and improving performance and vision inside the uterus. In group II, this situation was reported in [6 cases (6.82%)] and was solved by application of another vulsellum with more traumas to the cervix (Table 2).
6. Discussion
Cervical dilatation is the cornerstone in many gynecological procedures requiring introduction of sizable instruments inside the uterus. Many of these operations are done for biopsy in bleeding disorders or for exploring uterine cavity in infertility assessment. By far operative hysteroscopy is the most common gynecological operation requiring wide cervix and associated with multiple insertions and extractions of the scope [1,2].
Many interventions were tried to make dilatation easier as preliminary administration of lamineria tents or misoprostol to soften cervix. Difficulty and/or resistance to dilatations remain an important issue in some cases with stenosed cervix [3-8].
The most common type of cervical injury is a superficial laceration caused by the vulsellum or Allis forceps tearing off during dilation. At the other extreme are the cervico vaginal fistula and the longitudinal laceration ascending to the level of the uterine vessels. Rates of cervical injury range from 0.01 to 1.6 per 100 suction curettage [12,13].
In the current study, a cervical stitch was applied to the cervix in a manner like cerclage but at 1 cm above level of external os aiming to apply traction on the cervix with single application in group I compared to the traditional use of cervical vulsellum in group II.
The demographic data were nearly the same in both groups. Operative time required for cervical dilatation was shortened in group I (10.66±2.70 minutes) compared to (18.2±1.45 minutes) with P value (0.02). No complications occurred in group I while bleeding occurred in group II due to excessive force against the vulsellum with multiple applications and slipping of the vulsellum leading to more lacerations and more bleeding (Table 2).
Additional measures were taken in group II to decrease or stop bleeding as the use of by vicryl-1 suture to ligate bleeders which was indicated in 2 cases (2.27%), coagulants were used in 58 cases (65.91%) and vaginal packing were used in 34 cases (38.64%) (Table 2).
No cancellation of procedures was reported in group I while in group II, 3 cases were cancelled due to tight cervical stenosis with multiple applications and slipping of the vulsellum, failure to reach 10 mm in cervical dilatation, tired exhausted medical staff and occurrence of false tracks Table 2.
Johnson et al. (1991) conducted a study to evaluate safety of vulsellum use. They concluded that routine use of a vulsellum theoretically makes insertion of an intrauterine device safer and the passage of an embryo transfer catheter less traumatic [14].
Turok et al. conducted a study on 25 patients to evaluate Bioceptive cervical retractor instead of traditional vulsellum in IUD insertion. They concluded that the Bioceptive® suction cervical retractor demonstrated a new trend toward lower pain scores than the singletooth vulsellum and is a viable, atraumatic alternative [15].
Another trial done in Utah University, USA to replace the traditional vulsellum by a new spiral cervical retractor apparatus to minimize cervical trauma and decrease pain score in most of gynecological procedures. They concluded that the new device is a good alternative to vulsellum and is considered a potent cervical retractor that causes minimal pain, bleeding and cramping [9].
7. Conclusion
The application of cervical stitch before gynecological procedures requiring wide cervical dilatation was more effective than vulsellum. It provided stable and steady element for traction on the cervix and could be tightened to prevent leakage of fluids from inside the uterus to improve vision and performance in operative hysteroscopy.
Competing Interests
The authors declare that they have no competing interests.
Author Contributions
Dr. Ayman Shehata Dawood: Is the idea developer, operating all cases,
gathering information and revisions were done by him.
Dr. Mohamed Attia Raslan: Is the writer, data analyzer and revisions
were done by him.