


1. Introduction
Occupational leg symptoms, such as swelling, pain, and feeling of heaviness and tension in the legs frequently occur in healthy individuals who work for hours in the sitting or standing positions [1] . Sitting or standing for hours decreases the blood flow out of the legs and results in increased pressure on the veins; therefore, prolonged sitting and standing are both risk factors for the development of chronic venous disease [2] . Occupational leg symptoms, especially leg swelling is associated with feelings of tiredness and heaviness of the legs, and leg pain [1,3,4]; therefore, reducing leg swelling is an important approach to prevent the development of the chronic venous disease.
Previous studies have reported that compression stocking [1,4,5-18], neuromuscular electrical stimulation device [8] , and leg movement [9,10] are effective in reducing the occupational leg swelling. These methods promote calf muscle pump efficacy, peak venous velocity, and venous return, thereby reducing ambulatory venous pressures, interstitial fluid volume, and leg volume [5,11-13]. However, the above methods have disadvantages and cannot be applied to participants who have movement and sensory disorders, circulatory disturbance, and inflammation of the skin. On the other hand, it is reported that hand massage is effective in reducing chronic edema and lymphedema [14,15], and leg edema during pregnancy and postpartum [16,17]. Hand massage is advantageous in that it can be performed on a participant with the above-mentioned disorders because the intensity and treatment site can be manipulated manually. However, the effect of hand massage on occupational leg swelling has not been clarified. In addition, studies have revealed that hand massage improves emotion and mood [18,19]; however, the underlying neural mechanism has not been sufficiently verified. Hence, this study aimed to investigate the effect of hand massage on occupational leg swelling and resting-state electroencephalographic (EEG) activity.
2. Materials and Methods
2.1 Participants
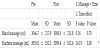
Eighteen healthy women (mean age ± standard deviation: 47.5 ± 16.2 years; mean height: 158.0 ± 4.4 cm; mean bodyweight: 50.9 ± 4.9 kg) who work in a sitting or standing position were included in this study. Only women were recruited because women have a higher incidence rate of leg swelling [1] . Participants with Mini-Mental State Examination (MMSE) scores below 24, cardiovascular or orthopedic diseases that might influence the results were excluded.
The study was conducted according to the principles of the Declaration of Helsinki and was approved by the local Institutional Ethics Committee (Kyoto Tachibana University). All subjects provided written informed consent and were free to withdraw from the study at any time.
2.2 Study protocol
This study was designed as a randomized cross-over study (Figure 1). First, the participants were divided into 2 groups (A and B). Group A received hand massage to their right leg and group B received machine massage to their right leg, for 15 minutes each. After 2 weeks, group A received machine massage to their right leg and group B received hand massage to their right leg, for 15 minutes each.

The participants were seated comfortably in a chair with back and armrests and then received either a hand or machine massage. The massaged right lower limb was held at 30 degrees of knee flexion. Hand massage was performed by a therapist who had worked as an instructor at the Japan Wellness Therapist Association for 5 years. Massage oil (2E32000, Naris Cosmetics Co., LTD, Japan) was used during the hand massage to prevent friction and discomfort. A standard massage technique, without pressure on the points indicated in foot reflexology [21] , was used in this study. First, the therapist stroked the entire lower leg, from the ankle to the knee, using her entire hand (5 minutes). Next, she stroked the entire foot from the toes to the ankle (5 minutes). Further, she stroked the toes one by one from the base of the toes toward the tip (5 minutes). The same therapist massaged all participants and was requested to keep the depth and rate of massage as consistent as possible. Machine massage was performed using the Foot Air Massager (HM-261, Omron Co., Ltd., Japan). This machine massaged, using pressurization, the toe, ankle, and the lower leg. Hand and machine massages were conducted for 15 minutes each. Lower leg volume and resting-state EEG activity were measured before (Pre1 and Pre2) and after (Post1 and Post2) each massage. Moreover, the emotion and mood states were measured after each massage (Post1 and Post2).
2.3 Experimental measurements
Lower leg volume was measured using the water displacement method. The reliability of the water replacement method has been reported in a previous study [22] . For the measurement, a rectangular shaped aquarium, with walls made of an acrylic board (length 300 mm × width 150 mm × height 450 mm, Natsume Seisakusho Co., Ltd., Japan), was used. A drainage outlet was attached to the upper end of the aquarium, and any water overflow was discharged from the drainage outlet. Next, the participants gradually lowered their right lower limb into the full water tank, and the displaced, overflowing water was measured with a measuring cylinder.
The Likert scale [23] was utilized to measure the degree of pleasant, relaxation and refreshing, after each massage, to assess the emotional state and mood after each massage. The Likertscale consisted of a 5-point scale ranging from 1 (strongly disagree) to 5 (strongly agree), and the higher scores indicated positive emotion and mood states.
EEG was obtained using a bio-signal recording system (Livo, Tec GihanCo., Ltd., Japan) and an active dry electrode system (g.SAHARA, g.tec Co., Ltd., Austria). EEG was recorded using 15 channels (Fpz, Fz, Cz, Pz, Oz, F3, F4, C3, C4, P3, P4, F7, F8, T7, T8) based on the international 10-20 system, at a sampling rate of 1000 Hz. Reference electrodes were attached to both the earlobes. The recorded EEG data were processed as follows: down sampling to 512 Hz, band pass filter set to 1-30 Hz, independent component analysis to remove artifacts, and re-referencing to the average reference, using EEGLAB (Version 15) [24] . Next, the exact low-resolution brain electromagnetic tomography (eLORETA) was used to analyze the cortical distribution of current source density [25] . In the eLORETA, the solution space consists of 6239 cortical gray matter voxels at 5 mm spatial resolution, in a realistic head model [26] , using the Montreal Neurological Institute (MNI) 152 template [27] . The eLORETA image was calculated in the alpha frequency band (8–13Hz) because the resting alpha activity reflects the emotion and mood states [28] .
2.4 Statistical analysis
Lower leg volume after each massage was analyzed with a 2 (massage: hand, machine) × 2 (time: pre, post) ANOVA. We assessed whether massage or time showed any significant differences using the post hoc Bonferroni test. The degree of pleasant, relaxation, and refreshing after each massage was analyzed using the Wilcoxon signed-rank test. Statistical analyses were performed with SPSS ver. 24.0 (IBM, Chicago, IL, USA). The comparison of the cortical distribution of current source density, between massages in each frequency band, was assessed by the voxel-by-voxel independent sample F-ratiotests, based on the eLORETA log-transformed current density power. In the resulting statistical three-dimensional images, cortical voxels exhibiting significant differences were identified utilizing a nonparametric approach (statistical nonparametric mapping; SnPM). The level of significance was set at a p < 0.05.
3. Results
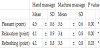
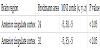
Two-way ANOVA showed that there was a significant time effect, although there was no significant group × time interaction (p < 0.05). Post-hoc Bonferroni comparisons revealed that the lower leg volume was significantly reduced after each massage compared with the lower leg volume before each massage (p < 0.05, Table 1). In addition, the magnitude of change in lower leg volume before and after each massage (pre-value minus post-value) was 38.3 ± 47.6 ml for hand massage; and 45.6 ± 56.3 ml for machine massage. The degree of pleasant, relaxation and refreshing was significantly higher after hand massage than after machine massage (p < 0.05, Table 2). There was no significant difference observed between the resting-state alpha activity for pre-hand and pre-machine massage (p > 0.05). Interestingly, the resting-state alpha activity after hand massage was significantly increased in the left anterior cingulate cortex compared with the resting-state alpha activity after machine massage (p < 0.05) (Figure 2, Table 3).

4. Discussion
This study aimed to investigate the effect of hand massage on occupational leg swelling and resting-state electroencephalographic (EEG) activity. We observed that occupational leg swelling was significantly reduced after hand and machine massages. It has been reported that compression stocking [1,4,5-18], neuromuscular electrical stimulation device [8] and leg movement [9,10] are effective in improving occupational leg swelling. The present study suggests that the hand and machine massages could contribute as an additional tool to improve occupational leg swelling.
Partsch H et al., demonstrated that occupational leg edema was reduced 34.1 ml using compression class A stocking (pressure at ankle level, 11.2 mmHg), 39.6 ml using compression class I stocking (pressure at ankle level, 18.1 mmHg), and 59.1 ml using compression class II stocking (pressure at ankle level, 21.8 mmHg) [5] . In another study, Mosti G et al., also reported that occupational leg edema was reduced by 40 ml by using graduated elastic compression stockings (pressure at ankle level: sitting = 22 mmHg, standing = 25 mmHg; pressure at calf level: sitting = 18 mmHg, standing = 21 mmHg), and by 20 ml using progressive elastic compression stockings (pressure at ankle level: sitting = 18 mmHg, standing = 19 mmHg; pressure at calf level: sitting = 30 mmHg, standing = 32.5 mmHg) [6] . On the other hand, occupational leg volume in this study was reduced by hand massage (38.3 ml), and by machine massage (45.6 ml). Thus, the reduction in occupational leg swelling observed in our study was similar to that observed in other studies.
The resting-state alpha activity, after hand massage, was significantly increased in the left anterior cingulate cortex compared with the resting-state alpha activity after machine massage. A previous study reported that movement performed with a human hand has a higher score of pleasantness and increases activity in the anterior cingulate cortex, when compared to movement with a rubber-gloved hand [29] . In this study, the degree of pleasant was significantly higher after a hand massage than after a machine massage. Therefore, it is suggested that a hand massage is more pleasant than a machine massage, resulting in an increase of resting-state alpha activity in the anterior cingulate cortex. Additionally, since we observed lateralization in the left anterior cingulate cortex, the involvement of emotion and mood processing in the left frontal region may be considered. This is supported by a previous study that revealed an association between positive information / emotional processing and an increase in alpha activity in the left frontal region [30] . The present study revealed that hand massage increased the alpha activity in the left frontal region related to positive information / emotional processing because the degree of pleasant, relaxation and refreshing was significantly higher after a hand massage than after a machine massage. In addition, since the alpha activity in the frontal region reflects the activity of the anterior cingulate cortex [31] , the present study identified the left anterior cingulate cortex as the source for the alpha activity, in the left frontal region and related to positive information / emotional processing, using the eLORETA analysis.
The present study does have a few limitations. First, since the hand massage was carried out with only one therapist, it is not certain whether other therapists will perform similar results. Second, longterm effects of hand massage and its effects on participants with any disease were not verified. Future studies are needed to verify the effect of hand massage taking into consideration the above issues.
5. Conclusions
This study investigated the effects of hand massage on occupational leg swelling and the resting-stage EEG activity. Results revealed that the lower leg volume was significantly reduced after hand and machine massages. Moreover, resting-state alpha activity after hand massage was significantly increased in the left anterior cingulate cortex compared with resting alpha activity after machine massage. This study suggests that hand massage improves occupational leg swelling and increases the resting-state alpha activity in the left anterior cingulate cortex.
Competing Interests
The authors have no competing interests with the work presented in this manuscript.
Author Contributions
HN, TK and SM conceived and designed the experiments. HN, TK, MS, TU, TT, IM and SM performed the experiments. HN, TK, MS, TU and SM analyzed the data. HN, TK and SM wrote the paper.
Acknowledgments
We would like to thank all volunteers who participated in this study.