


1. Introduction
Urinary tract infections (UTIs) are among the most common bacterial infections occurring in both community and health care setting, with a substantial financial burden on the public health system [1]. Symptomatic UTIs result in about 7 million visits to outpatient clinics, 1 million visits to Emergency Departments and 100˙000 hospitalizations annually in USA [2,3]. UTIs have become also the most common hospital-acquired infection, accounting for as many as 40% of nosocomial infections (primarily catheter-related infections), and represent the second most frequent cause of secondary bacteremia in hospitalized patients [4]. Apart from accounting for extra hospital costs, these infections may be an important reservoir for selection and transmission of multidrug–resistant bacteria [5].
UTIs are diagnosed by urine culture. The laboratory examination of urine specimens accounts for most of the workload in many hospitalbased microbiology laboratories, accounting for as many as 40% of the submitted specimens [2].
In suspected UTIs, empirical antibiotic treatment is usually started before the laboratory results of urine culture and antibiogram are available because of the long time required for these analysis [6]. This can result in therapeutic failure in case of resistant strains, and ultimately lead to the spread of antibiotic resistance among pathogens responsible for both community and nosocomial acquired infections [7; 8]. The availability of a rapid, user-friendly, accurate and inexpensive test, that could quickly detect a clinically significant bacterial load in urine, would allow physicians to properly decide which patients really need antibiotic treatment, thereby improving therapeutic success and reducing the emergence of antibiotic resistance.
A point-of-care test (POCT) is defined as a diagnostic test performed promptly and conveniently at or near the site of patient care avoiding the often lengthy procedure of sending samples to be processed in a central laboratory [9]. Up to date, there are no microbiological POCTs developed for the diagnosis of UTIs. Rapid biochemical dipstick tests are available and currently used as predictors of bacterial UTI, but must often be correlated with other testing and clinical information. In many clinical settings, in fact, it has been proved that the dipstick urinalysis leads to many false positive and negative results when compared with the gold standard culture method, demonstrating the low sensitivity and positive predictive value [10]. The Micro Biological Survey method (MBS) is an alternative method for bacterial counting developed and patented by Roma Tre University [11,12]. It is based on a colorimetric survey performed in mono-use disposable reaction vials in which samples can be inoculated without any preliminary treatment. The analysis can be carried out using a thermostatic optical reader that automatically detects the color change. The ease of use of the MBS method has been evaluated in a previous study on food samples demonstrating the possibility to use it anywhere and without the need of an equipped laboratory and specialized personnel [13]. In previous studies carried out on artificially contaminated urine samples, this method has already been proven to be suitable for the evaluation of the bacterial load and the assessment of the susceptibility to a panel of antibiotics [14,15]. The present study has been undertaken to clinically evaluate the performance and operational characteristics of the MBS POCT for the diagnosis and the antibiotic treatment of UTIs. The MBS method was also compared with another biochemical rapid test for UTI diagnosis, namely the urine dipstick assay [16].
2. Materials and Methods
2.1 Study design
A prospective diagnostic accuracy evaluation study was performed in collaboration with the Department of Emergency Medicine of Azienda Ospedaliera Sant’Andrea of Rome. Between November 2013 and July 2014, a total of 122 patients with clinically suspected UTIs was enrolled upon hospital admission in the Emergency Department. Criteria for the clinical suspicion of UTI were: high levels of leukocytes in urine, their cloudy appearance and/or abnormal color and the presence of a catheter left in place for more than 72 hours. Urine samples from indwelling urinary catheter were obtained from the sampling port using the aseptic technique. The port is usually situated in the drainage tubing, proximal to the collection bag ensuring the freshest sample possible. Urine samples of non-catheterized patients were obtained via the clean-catch midstream technique. Urine samples were collected in the morning in disposable sterile urine collection containers, split into two aliquots and immediately analyzed with the MBS method and using the routine urine culture / antibiogram protocols in use by the hospital laboratory. Among 122 urine samples, 72 were analyzed also using urine dipsticks.
2.2 Ethical approval
Approval of the preliminary clinical trial was obtained on 14.01.2013 from the Ethical Committee of the Azienda Ospedaliera Sant’Andrea, constituted according to DM 12.05.2006 following Good Clinical Practice. The authorization was given on the basis of the declaration that the patients were duly informed and consenting. Only patients subscribing the informed consent were enrolled. In addition, the clinical trial did not require any change in the normal diagnostic and therapeutic strategy. The results from the laboratory analysis with the results obtained from the new device were compared in anonymous way.
2.3 Hospital laboratory tests
Urine specimens were inoculated onto blood agar and selective CHROM agar plates using a calibrated 0.010 ml loop and streaked manually. All culture plates were incubated at 37°C for at least 24 h before reading. Bacterial counts were determined by the dilution plating method. The analytical results were defined according to the Hospital Laboratory report (Positive or Negative) that also specified the presence of a concentration of bacteria ≥ 105 colony-forming units (CFU)/ml (criterion used by the hospital laboratory in the 97% of the positive medical reports). The number and identification of different organisms were primarily assessed by colony color and morphology. The definitive identification was performed using the VITEK® MS (BioMérieux Italia S.p.a., Florence, Italy). The VITEK® 2 system (BioMérieux Italia S.p.a., Florence, Italy) automated system with 64- well cartridges was used for antibiotic susceptibility testing according to the CLSI recommendations [17].
2.4 Urine dipstick test
A small volume of urine from the sterile container was drawn with a sterile syringe, and then applied to the urine dipstick (DIRUI, DIRUI Industrial Co., Ltd, Changchun, China). A positive result was defined in the presence of both leukocytes and nitrite [18]. The test was carried out immediately after urine collection at the patients’ bedside by the hospital personnel.
2.5 Urine Bacterial Count using the MBS POCT
The MBS POCT device for UTIs diagnosis used in this study was made by MBS srl, Rome, Italy. The MBS method measures the catalytic activity of bacteria through a redox indicator that changes color according to the oxidative state of the medium. The presence of bacteria causes a color change of the reaction vials from blue to yellow in times that are inversely related to the logarithm of the bacterial concentration, allowing an unequivocal correlation between the observed enzymatic activity and the number of viable cells present in the sample. It makes use of specific disposable vials for the detection and quantification of bacteria called Urine Bacterial Count (UBC), in which samples can be inoculated without any preliminary treatment. The MBS Multireader automates the analysis process automatically detecting the time for color change. It is designed to be used at the patient’s bedside, it is computer managed and can be battery powered (Figure 1). Vials can be stored for 6 months at room temperature and for 12 months at 4°C. The MBS Multireader does not need any specific maintenance.

According to the MBS method, 1ml urine samples were manually injected in the UBC vials immediately after urine collection. Vials were then incubated in the MBS Multireader at 37°C up to 27 hours in order to check the time taken for the vials to change color also when urine samples did not display a significant bacteriuria but only a low bacterial load.
After analysis, small aliquots of the vials content (that can be assimilated to a bacterial preculture) can be taken out to perform bacterial identification using standard techniques; otherwise, the vials content can be sterilized simply by pressing the cap on top of the vials and then disposed as “Non-Hazardous Waste”.
2.6 Diagnostic accuracy evaluation of the MBS POCT
The outcomes of the MBS POCT were compared with the outcomes of the reference test for urine culture. The performance characteristics were evaluated by the Receiver Operating Characteristic analysis using MedCalc statistical software, Windows version 15,0 (MedCalc software, Ostend, Belgium) [19]. This analysis is widely used in medicine to determine the validity of a diagnostic test and to find its optimal cut off limit. In particular, the Area under the ROC Curve (AUC) is a measure of how well a parameter can distinguish between two diagnostic groups, which is subjects with and without a UTI. An area under the curve equal to 1 is that of a test that displays 100% sensitivity and 100% specificity. Accuracy, sensitivity and specificity of urine dipsticks for the diagnosis of UTIs were also evaluated according to Friedman et al. [20].
2.7 Antibiotic susceptibility testing using the MBS POCT
Presumptive antibiotic susceptibility was assessed by using UBC vials supplemented with three different antibiotics chosen among those recommended by the Infectious Disease Society of America [21]. Antibiotics were arbitrarily added at the clinical breakpoint concentrations, according to EUCAST (www.eucast.org), namely: 8 μg/ml amoxicillin-clavulanic acid, 1 μg/ml ciprofloxacin, and 4 μg/ml trimethoprim-sulfamethoxazole. For the MBS POCT analysis, 1 ml of urine samples was manually injected in the UBC vials supplemented with antibiotics immediately after urine collection. Vials were then incubated in the MBS Multireader at 37°C for 27 hours. After analysis vials were sterilized simply by pressing the cap on top of the vials and then they were disposed as “Non-Hazardous Waste”. Bacteria were predicted to be susceptible if, following urine inoculation in the vial supplemented with the specific antibiotic, they did not induce a color change of the medium, suggestive of absence of growth in the presence of antibiotic. Bacteria were instead predicted to be resistant to the antibiotic if causing a color change in times proportional those determined analyzing the same urine samples in the UBC vial without antibiotic.
2.8 Statistical evaluation
The outcomes of the MBS POCT for antibiotic susceptibility test were compared with the outcomes of the reference standard test of antibiograms. Accuracy, Sensitivity, Specificity as well as Positive Predictive Value (PPV) and Negative Predictive Value (NPV) were evaluated according to Friedman et al. [20].
3. Results
3.1 Patients’ characteristics
During November 2013 and July 2014, a total of 122 patients was enrolled in this study. Among them 59 (48%) were men and 63 (52%) women. The mean patient age was 77 years old (40-49 years of age, 1%; 50-59 years of age, 11%; 60-69 years of age, 11%; 70-79 years of age, 25%; 80-89 years of age, 37%; 90-100 years of age, 14%). Most of the patients were catheterized (89%) and already under antibiotic therapy (80%). The antibiotics administered to the patients were: 28% Fluoroquinolones, 19% Cephalosporins, 16% Penicillins, 10% Carbapenems, 9% Glycopeptides, 9% Nitroimidazoles, 7% Macrolides, 1% Oxazolidinones and 1% Polymyxins. In few cases, more than one antibiotic was administered to the same patient.
3.2 Urine cultures results
Urine cultures were performed by the hospital laboratory and usually results were obtained after 48-96 hours. A positive result was found for 34 patients. Fungal infections were found in 10 patients but considered negative for bacterial UTI. Polymicrobic associations between fungi and bacteria, found in only 2 patients, were considered positive. Regarding bacterial UTIs, Enterococcus faecalis and Escherichia coli were the most frequent causative agents (26% and 20%, respectively), followed by Klebsiella pneumoniae (11%), Proteus vulgaris (9%), Pseudomonas aeruginosa (9%), Staphylococcus aureus (4%). Polymicrobic associations were observed in 19 patients (56%).
3.3 Urine Bacterial Count using the MBS POCT
The MBS POCT analyses were carried out at patients’ bedside. The MBS method is designed for detection and quantification of bacteria and the presence of fungi did not cause color change and produced a negative result. The time taken for the UBC vials to change color was inversely related to bacterial concentration in urine, and no correlation was found between the time required for color change in infected urine and the administration of antibiotics to the patient, indicating that previous administration of antibiotics to the patients does not modify MBS POCT analytical results.
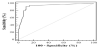
3.4 Diagnostic accuracy evaluation of the MBS POCT
To verify the diagnostic performance of the MBS POCT, quantitative results obtained using the UBC vials without antibiotics, in terms of time taken for the vials to change color, were compared to the ones of conventional urine cultures (positive or negative). The comparative analysis was performed using the Receiver Operating Characteristics curve analysis. The AUC of the MBS POCT was 0.93, very close to the theoretical limit of 1 (Figure 2), demonstrating the overall accuracy of the method. The combination of optimal sensitivity and specificity was obtained at 5 hours (Figure 3). At this time the maximum percentage of true positive and true negative results was observed (Figure 4), with 90.2% accuracy, 91.2% sensitivity, and 89.8% specificity.


3.5 Comparison between MBS POCT and urine dipstick for UTI diagnosis
The effectiveness of the MBS POCT in diagnosing UTI was also compared to that of urine dipsticks, using the standard urine culture as the reference method. Urine dipsticks are widely used for fast and cheap presumptive diagnosis of UTI.
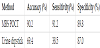
Positivity criteria for UTI were: color changed within 5 hours in the MBS POCT and positivity for both leukocytes and nitrite in the urine dipsticks [18]. Results are shown in Table 1. It can be seen that there is a poor agreement between urine cultures results and urine dipstick which yielded 16 false negative and 6 false positive results out of 72 samples analyzed. Notably, a general agreement between results obtained with the MBS POCT and urine cultures was observed. The MBS POCT displayed a much higher accuracy, sensitivity and specificity compared to urine dipsticks. In fact it revealed only 3 false negative and 9 false positive results out of 122 analyses (Table 2).
3.6 Presumptive antibiotic susceptibility testing with the MBS POCT
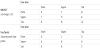
Antibiograms performed by the hospital laboratory yielded results 48-96 hours after urine sampling. Resistance to amoxicillin-clavulanic acid, ciprofloxacin and trimethoprim-sulfamethoxazole was observed in 38%, 84% and 69% of the isolates respectively, following the Clinical and Laboratory Standards Institute (CLSI) procedure.
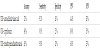
To verify the possibility to use the MBS POCT for a direct susceptibility testing of infecting bacteria, urine samples of 31 patients, resulting positive for UTI with both UBC vials and urine culture, were tested in parallel with antibiotic-free and antibiotic-supplemented UBC vials. MBS POCT considers positive to bacterial growth the color change of the vials and negative to bacterial growth the lack of color change, within 5 hours. In the susceptibility test, an antibiotic resistance induces a color change (positive to bacterial growth), while susceptibility does not induce a color change (negative to bacterial growth). Results shown in Table 3 were used to determine accuracy, sensitivity, specificity, as well as Positive Predictive Value (PPV) and Negative Predictive Value (NPV) for the MBS vials supplemented with the three different antibiotics (Table 4), relative to the standard CLSI method. Although values varied depending on the antibiotic, a similar trend was observed, resulting sensitivity>accuracy>specifi city for all three antibiotics. Results showed a good concordance of true resistant (true positive) results for the UBC vials supplemented with ciprofloxacin and UBC vials supplemented with trimethoprimsulfamethoxazole, underlined by a PPV of 89% and 68% respectively; a high presence of false resistant (false positive) results for the UBC supplemented with amoxicillin-clavulanic acid, underlined by a PPV of 44%. The highest probability of a true susceptibility (true negative) result was obtained with the UBC vials supplemented with amoxicillin-clavulanic acid, demonstrated by an NPV of 83%.

3.7 Discussion
UTIs are the second most common community-acquired and clinical healthcare-associated infections, and urine samples constitute the largest category of specimens examined in most microbiology laboratories [22]. The initial antibiotic treatment of UTIs is most often decided on empiric basis [6]. The gold standard for diagnosis and successful management of UTIs is to perform a urine culture, with identification and quantification of the infecting agents, followed by antibiotic susceptibility testing to determine the specific therapy to be administered to patients. In hospital settings, this approach requires a considerable effort in terms of workload and delays the achievement of results. Furthermore, it can lead to unnecessary antimicrobial overuse which ultimately promotes the emergence of resistance. Semi quantitative urine culture, that are the reference standard for diagnosis of UTI, display in fact several practical problems since at least 24 hours are needed for detection of bacterial growth on culture media. This implies that the diagnosis is uncertain for the first 24–48 hours after sample collection. Urine culture is also expensive and needs a microbiological laboratory with skilled technicians. Because of the clinical importance of early diagnosis, rapid urine tests as urine dipsticks are widely used. This test, however, is not enough accurate, and does not provide suitable indication for antibiotic treatment of UTIs, thus it cannot be used as a replacement test for urine culture [23]. Therefore, there is the urgent need of rapid, accurate, userfriendly and inexpensive tests for UTI diagnosis, confidently usable by unspecialized personnel at the patient’s bedside. The aim of this study was to perform a preliminary clinical study of a new POCT device for the diagnosis and management of UTIs.
The MBS method is a colorimetric system for bacterial counting. The presence of bacteria is detected through a redox indicator that changes in response to active bacterial metabolism. The time of color change is inversely related to the bacterial concentration in the sample. The main characteristics of the MBS method are speed, ease of execution and interpretation of results. It does not require a specialized microbiological laboratory and the presence of skilled personnel. The device used in this study is made of specific, ready to use, disposable, reaction vials and a thermostatic optical reader that automatically detects the color change and calculates the bacterial load. It is designed to be used at the patient’s bedside, it is computer managed and can be battery powered. The MBS POCT has been developed for the detection and quantification of bacteria in urine and for the evaluation of their susceptibility/resistance to a panel of antibiotics.
In this study, the MBS POCT has been used to detect the bacterial load in urine samples of patients with clinical evidence of UTI. However, the final aim of our work is to find the conditions in which it would be possible to substitute the traditional methods of analysis (urine culture and traditional antibiotic susceptibility testing) with the MBS POCT, in order to diminish the time required for UTI diagnosis and drastically decrease the use of empirical antibiotic treatment, addressing in a short time the most suitable therapy using targeted antibiotics.
In this study, the microbiological investigations carried out with traditional methods demonstrated that patients were infected by bacterial species which are most commonly responsible for UTIs worldwide [24] and the diagnostic performance of the MBS POCT has been evaluated using the ROC curve analysis [19]. The effectiveness of the POCT MBS in diagnosing UTI has also been compared to that of urine dipsticks, considering urine culture as the reference method. Results demonstrate that the MBS POCT is able to reveal the presence of a significant bacterial load in urine, hence diagnose a clinical UTI, in only 5 hours. More importantly, the MBS POCT showed much higher accuracy, sensitivity and specificity compared to urine dipsticks. It should also be emphasized that positive vials can also be considered as a bacterial pre-culture ready to use for further microbiological analysis, e.g. bacterial identification. This method has therefore the advantage of providing quantitative information on the bacterial load, which is essential for UTI diagnosis, as well as providing samples for identification and susceptibility testing with traditional methods of analysis. No evident interference due to previous administration of antibiotic was observed.
The MBS POCT was also used for a presumptive evaluation of bacterial susceptibility to a selected panel of antibiotics immediately after urine collection. In this case results were not fully satisfying. The main reason of unsatisfactory MBS method results is due to the MBS POCT detection of many false resistant results probably as a consequence of a very high concentration of bacteria inoculated in the vials. It is possible that the bacterial metabolism was detected before antibiotics had an effect, leading to a color change of the vial even if inoculated with bacteria susceptible to the tested antibiotic. In fact, the inoculum size has a profound impact on antibiotic susceptibility results [25]: increasing inoculum size can diminish the activity of certain antimicrobial agents. The inoculum size has in fact been recognized as the single most important variable in susceptibility testing for both bacteriostatic and bactericidal antibiotics [26]. Conventional antibiotic susceptibility tests must be performed using a standard bacterial inoculum, and the activity of antimicrobial agents is referred to that specific inoculum concentration. This condition could not be reproduced in the MBS POCT analysis. The greater concentration of bacteria occurring in the MBS vials was affected by the antibiotic to a minor extent, leading to a partial misinterpretation of results. However, it should be emphasized that the detection of false resistant strains is much less significant than the detection of false susceptible strains. Nevertheless, in the future, this problem could be solved by preliminary adjustment of the volume of urine to be analyzed into the MBS POCT, and further studies will be performed in this direction.
4. Conclusion
The MBS POCT represents a valuable diagnostic tool for a rapid and accurate detection of bacteria causing UTIs. Quantitative and qualitative analyses can be performed simultaneously. In this way it could be possible to have, in a relatively short time compared to standard methods, an accurate indication of UTI and a preliminary evaluation of the antibiotic susceptibility of the infecting bacteria, ensuring a prompt diagnosis and guiding the antibiotic choice long before the conventional antibiotic susceptibility test is performed. Its introduction into routine use in the Emergency Department could thus improve turn-around time for the medical decision making to give or not antibiotic treatment, drastically decreasing the time required to achieve the laboratory-based diagnosis, improving patients’ outcome, reducing antibiotic resistance, and ultimately saving money. We are confident that this test could be targeted to a much more heterogeneous population in laboratory, clinical or field settings. This test will be in fact addressed to virtually all adults affected by UTIs with multiple uses among hospitals, pharmacies and general practitioners: patient management; screening for asymptomatic infections; surveillance; epidemiological studies; evaluating the effectiveness of interventions; and detecting infections with the possibility to also study drug resistance.
Competing Interests
The authors declare that they have no competing interests.
Author Contributions
GA and SDS designed of the study and coordinated the research. AA, VC, VF, FL, OS, FC RM and LM collected the data. AA, FL and OS analyzed and interpreted the data. AA, FL, OS and GA drafting the article. AM, IS and PV critically reviewed the article. The authors warrant that all of the authors have contributed substantially to the manuscript and approved the final submission.
Acknowledgments
The authors gratefully acknowledge Dr. Andreas Bergmann (Sphingotec GmbH, 16761 Hennigsdorf, Germany), Dr. Metod Miklus (Sphingotec GmbH, 16761 Hennigsdorf, Germany), Dr. Robert Hellmich (Oncoprevent GmbH, 16761, Hennigsdorf, Germany) and Dr. Paul Scigalla (Oncoprevent GmbH, 16761, Hennigsdorf, Germany) for helpful discussions.
Abbreviations
AUC = Area Under the Curve
CFU = Colony Forming Units
MBS = Micro Biological Survey
POCT = point-of-care test
ROC = Receiver
Operating Characteristics
UBC = Urine Bacterial Count
UTI= Urinary Tract Infection