


1. Introduction
Cervico-vaginal infections are one of the most common problems in clinical medicine. The diagnosis of vaginal discharge is based on a History, Physical examination, and a few simple diagnostic tests [1]. Some patients with cervicitis note a purulent vaginal discharge, deep dyspareunia, and spotting after intercourse, while others may be symptom-free. The most common infections are Gardnerella vaginalis Candidia albicans and Trichomona vaginalis that are responsible for 90% of the cases of diseases infectious origin [2,3].Candida causes intense itching with a cheesy, dry discharge. Gardnerella causes a foul-smelling, thin white discharge. Trichomonas gives irritation and frothy white discharge. Chlamydia may cause a purulent vaginal discharge, post-coital spotting, and deep dyspareunia. Gonorrhea may cause a purulent vaginal discharge and deep dyspareunia [4].
Papanicolaou stain (Pap-smear or Pap test) is a cytological method used for screening of cervical cancer and some infectious disease like Gardnerellavaginalis, Candidia albicans and Trichomonasvaginalis by identification either of the organism or of characteristic cytological cellular changes [5,6]. The Pap test is easy to perform, and relatively inexpensive, as well as large number of women can examined by Pap –smear annually [8]. Thus, this technique can become an important tool and the easiest method for detection of cervico-vaginal infections, especially, in developing countries [4,9]. This study aimed to show the causes of cervico-vaginal infections among Sudanese women with vaginal discharge concerning their age, place of residence, and circumcision using Pap smear. The purpose of this study is to assess the clinical efficacy of tigecycline in hospitalized patients.
2. Methodology
Study design: In this cross sectional hospital based study, one hundred cervico-vaginal samples collected from Sudanese women complain of vaginal discharge attended at gynecology department – Khartoum teaching hospital from different places of Sudan. All patients signed an informed consent form.
Sample collection: Cervico-vaginal specimens were collected by expert gynecologist using spatula, the collected samples were spread on clean microscopic slides.
Papanicolaou stain: The smears were fixed immediately in 95% ethanol for 15 minutes, and then rehydrated through descending grades of alcohols 80%, 70%, 50%, and washed with distilled water. Then they were stained with papanicolaou stain using slandered Pap stain procedure.
Data Analysis: Statistical Package for Social Sciences (SPSS) version 20 was used in this study, to analyze, descriptive statistics such as frequency tables, mean. Chi-square test was applied to find the association between two variables. The significance level of 0.05 was considered for statistical analysis.
3. Results
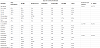
The age of patients ranged from 17 to 50 years (median 29 years) with a mean of 31.5 ± 16.15 years. Most of cases included in this study were in the 3rd decade of life, this group represents 41%of total study population. Out of 100 women, 95women were circumcised and the remaining five women were non-circumcised. Concerning the geographical location, 47women were from Northern, 41from Central, 8from Eastern, 2 from Western and 2 from Southern Sudan as described in Table 1.The most common type of infection was bacterial vaginosis (54%) followed by candida infection which represented18% of the studied cases while the remaining 28%had non-infected vaginal discharge (figure 1).

The cytological features of the types of infection were illustrated in Figure 2.

Twenty six % of circumcised women were negative (non-infected), 48% had bacilli infection, 1% had Actinomyces, 2% had leptothrix, 1% had Gardinellavaginalis and 17% had Candida albicans. Two % non-circumcised were negative (non-infected), 1% had bacilli infection, 1% had actinomyces, and 1% had Candida albicans as shown in table 1.
In this study, the major cause of cervico-vaginal infection was bacterial vaginosis(bacilli) followed by candidiasis seen in women came from Central and Northern Sudan (table 1).
Regarding the occupation of women, the majority of them were housewives.This group represents 73% of the total cases. 24% of them were negative, 28% had bacilli infection, 2% had actinomyces, 2% had leptothrix, 1% had Gardenellavaginalis and 16% had vaginal candidiasis. The employees represented 27% of the participants, 4% were negative, 21% had bacilli infection and 2% had candida infection. 51% of the studied cases live in Khartoum city of whom 13% were negative, 25% had bacilli infection, 1% had leptothrix, 1% had Gardenellavaginalis and 11% had vaginal candidiasis. 27% of cases came from Omdurman city of whom 6% were negative, 12% had bacilli infection, 1% had leptothrix and 3% had candidiasis. 27% of participants live in Khartoum north (Bahri) of whom 9% were negative, 12% had bacilli infection, 1% had actinomyces, 1% had leptothrix and 4% had vaginal candidiasis. Concerning the educational level, 79% of the study participants were at the secondary level of education. This group represents the majority of cases, while 11% of them were graduated. 4% of the women were illiterate and 6% of them stopped their education at the primary level.
4. Discussion
Vaginal discharge is one of most frequent gynecological problems encountered in females especially during their reproductive stage [10]. The microbiological flora of the lower female genital tract provides a dynamic, complex example of microbial colonization, the regulation of which is not fully understood. When an exogenous bacterial species, with its array of virulence factors, is introduced into the host, disease does not always occur. Conversely, under selected conditions, commensal endogenous bacteria—for example, Gardnerella vaginalis and group B streptococci can participate in disease processes [11].
This study has shown that most cervico-vaginal infections were attributable to bacterial vaginosis (54%) and vaginal candidiasis (18%).These findings to some extentis in agreement witha previous study in which the prevalence of bacterial vaginosis and vaginal candidiasis among women with vaginal discharge was (40%) and (25%) respectively [12].
Our findings differed from the results of a study carried by Maria et al 2014in Iran who reported that most cervical-vaginal infections were attributable to Candida and then Trichomonas and Gardnerella [4]. Other studies reported that the prevalence of bacterial vaginosis and vaginal candidiasis varies from 15- 61% and 14 – 30% respectively [12-15]. These differences are due to different study populations, various climate, socio-economic and cultural conditions, different sensitivity of diagnostic tests, applying different diagnostic methods [4,13,14,15].
Our findings revealed that women aged up to 30 years had the highest prevalence rates of cervical-vaginal infection by bacilli bacteria, Actinomyces and Leptothrix while the highest rates of prevalence of cervico-vaginal infection by candida was observed in the women aged 41 to 50 years. This is consistent with the result of many previous studies [3,4,13,16].
Akingbade et al. reported that the prevalence of Candida albicans amongst women attending antenatal and gynecology health centers in Abeokuta, Nigeria was 24.4% [10].
Bacterial vaginosis is best described as a disruption of the vaginal microbiota or as a vaginal bacterial dysbiosis. It is characterised by a reduction or a replacement of the protective Lactobacillus species by an overgrowth of other anaerobic bacteria [17].
Our study showed that there was no significant association between cervico-vaginal infections with age group, circumcision, and occupation (p- value of these variables were 0.481, 0.137 and 0.791 respectively). This findings support the result of the study carried by Rathod et al., who did not find strong evidence for associations between sociodemographic characteristics and the diagnosis of vulvovaginal candidiasis [18].
Xang et al. (2009) reported that the three most frequent reproductive tract infections (RTIs) were endocervicitis, bacterial vaginosis (BV) and trichomoniasis, with prevalence’s of 41.7%, 12.0% and 4.5%, respectively. Multiple infections were prevalent among our sample. 20.4% (10,854) of our sample had two RTIs and 8.8% (4713) had at least three RTIs. Multivariate analysis showed that women's age, education, occupation, dysmenorrhea, number of deliveries, personal hygiene habit, menstrual cycle, menstruation, abortion, the interval between abortion and sexual intercourse afterwards, RTI knowledge and the frequency of sexual intercourse per month were all related to RTIs in their sample [19].
Bacterial flora and mycosis of the vagina was studied by Turovskiy et al. 2011, to estimate the microbiological profile of vaginal flora and its association with any of the suspected demographic criteria in women complaining from pathological symptoms (pruritus, burning, vaginal discharge). They concluded that the common reason of vaginitis is bacterial infections. Both, place of living and women’s age influence the type of etiological factor [20]. However, our findings were not in consistency with this result as the p value of our result concerning residence versus infection was 0.387, which was statistically non-significant.
5. Conclusion
The most frequent infection among Sudanese women complain with vaginal discharge is bacterial vaginosis and Candida albicans. Pap smear had a relatively low predictive value for the presence of vaginal pathogens among women complaining of vaginal discharge.
Competing Interests
The authors have no competing interests with the work presented in this manuscript.
Ethics Approval
All patients were assured that all their obtained information will be handled in a confidential atmosphere and it will not affect their life after taking verbal and written consent. Ethical clearance and protocol approval were obtained from research and ethics committee of University of Medical Sciences, Sudan.
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in Brazil 2013.