


1. Introduction
Despite the flashing advances in medical science investigation and clinical therapy, population of end-stage renal disease (ESRD) with subsequent renal replacement therapy patients is still growing annually [1]. Approximately half of the annual mortality (6-9%) of CRF patients can attribute to the cardiovascular diseases [2]. Cardiac disease is also common in pre-dialysis chronic kidney disease patients and occurs with increasing frequency, severity and mortalityassociated risk as renal function deteriorated [3,4]. Recently, quality of life (QOL) among chronic hemodialysis (HD) patients becomes an important parameter of the treatment adequacy and deserves various clinical investigations, especially cost-effectiveness relation under government insurance coverage [5,6]. HD patients can have impaired daily functioning because of their primary kidney disease and comorbid conditions [7]. Among these efforts, the role of assessments of health-related QOL (HRQOL) by the application of generic and specific measures that are used to examine which dimensions or areas in patients’ life are impaired and necessitate an appropriate intervention is particularly important [8,9]. Self-efficacy of patient-oriented point of view can be of great value in the evaluation of treatment outcome and dialysis course [10,11]. The aim of this study was to analyze the association between independent clinical, laboratory, dialysis factors and self-efficacy of the QOL with HD treatment outcome which will be compared with a validated disease-specific score for cardiac risk stratification [12-14] and the QOL application in HD patients [15].
2. Materials and Methods
There were 43 patients (17 men and 26 women, aged 55.2 ± 12.31 years old) undergoing long-term maintenance thrice weekly HD therapy recruited in this study. Patients answered the Kidney Disease Quality of Life questionnaire (KDQOL-SFTM) which includes the SF-36 (8 dimensions/36 items): physical functioning (10 items), role limitations caused by physical problems (4 items), role limitations caused by emotional problems (3 items), pain (2 items), general health perceptions (5 items), social functioning (2 items), emotional well-being (5 items), energy/fatigue (4 items), and 1 item about health status compared to one year ago; kidney-disease-targeted items (11dimensions/43 items); symptom/problem list (12 items), effects of kidney disease (8 items), burden of kidney disease (4 items), cognitive function (3 items), quality of social interaction (3 items), sexual function (2 items), sleep (4 items), social support (2 items), work status (2 items), overall health rating ( 1 item scored separately), patient satisfaction (1 item), and dialysis staff encouragement (2 items). Self-efficacy scoring system developed locally which is divided into two dimensions; self-awareness (11 items), and self-care (5 items) also added in the questionnaire. Clinical data including dialysis treatment type and co-morbidity (cardiovascular diseases, chronic obstructive lung disease, peripheral vascular disease, diabetes mellitus, cerebrovascular disease, liver disease, hypertension, visual deficit, ambulation deficit, and cancer) were recorded and analyzed. Laboratory parameters including electrolytes, HD efficiency data (e.g.: Kt/V, nPCR, URR), albumin and creatinine were also analyzed. Application of a previously validated cardiac risk score (CRS) using cardiac history (A), dialysis duration (B), body mass index (C) and serum phosphate (D) multiplied by various hazards ratio (HR) was also investigated retrospectively. CRS (A+B+C+D)< 50 allocated low risk, and CRS≥50 stands for high risk of future cardiac events. The impact of various factors on CRS and various factors on KDQOL-SFTM were estimated by multivariate analysis using SPSS® 10.0 depending on variables' characteristics. Cox’s regression analysis for relative laboratory and clinical outcome also performed. The tests were twotailed and P<0.05 was considered to indicate statistical significance.
3. Results
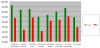
HRQOL dimension scores of KDQOL-SF™ questionnaire (Table 1) obtained from the HD patients is significantly (P< 0.001) lower as comparing with the scores obtained from the normal control in Taiwanese population (Figure 1). Self efficacy was significantly related to the overall health (P<0.01) and physical functioning items (P<0.01). One of the HD efficiency data (nPCR) was also significantly related to cognitive function and quality of social interaction dimensions in KDQOL. Except for the mean dialysis age 7.4 ± 0.94 years is not statistically significant to the self efficacy and health care, or the KDQOL scores. Patients with older age had lower KDQOL coefficients’ scores (Table 2). In comparison with the KDQOL dimensions, correlation coefficients were statistically significant for the following laboratory data (Table 3): potassium (P<0.01), calcium (P<0.05), phosphate (P<0.01), creatinine (P<0, 01), and albumin (P<0.01). Hct was inversely significant in patient satisfaction and dialysis staff encouragement, but significant in dialysis year and patients’ age.

Values for all dimensions vary from 0 to 100 (best quality of life). 43 hemodialysis patients completed the questionnaire.

*p<0.05, **p<0.01.

*p<0.05, **p<0.01.
CRS≥50 was found in 19 patients and 6 had cardiac events after electrocardiography and cardiac stress imaging proven in the following observed 9 months period. CRS< 50 were in the remaining 24 patients with 1 cardiac event occurred. PHC and MHC in QOL were significant in CRS≥50 group (P<0/01), while only MHC in QOL was found relating in CRS< 50 group (P<0/01). Dialysis year was irrelevant to the QOL statistically, but proportionate with CRS.
4. Discussion
The methods used to evaluate the quality of life questionnaires in nephrology are not adequate and impractical as compared with the normal population ones [16]. It is also important to determine whether intra-observer and inter-observer of the self-applied procedure or application of the questionnaire is reliable to reflect clinical changes over times in the dialysis treatment course [17,18]. Additional problems are the wrong choice of questionnaire or problems with its utilization [19]. The KDQOL-SFTM has many advantages compared to other instruments e.g. it has been tested in several populations with kidney disease, it has both general and specific modules to access chronic kidney disease, it has questions about the sexual area and professional rehabilitation, and it can be self-applied or applied by the interviewer [20]. Self-efficacy and health care added in KDQOL-SF™ as a whole to investigate the exact quality of patients on regular hemodialysis proved to be a effective tool not only in predicting the outcome of dialysis patients, but the costeffectiveness among medical intervention needed [21]. We conclude that QOL analyses are particularly helpful for investigating the social, emotional and physical effects of treatment and disease processes on ESRD patients' daily lives [22]. From this study, it is obvious that the older the patients’ age, the less scores he will acquire. However, patients undergoing dialysis did not have lower scores with longer dialysis years. This implied that an intensive bedside assistance and continuous workup with quality survey monitoring will further profit the patients on dialysis, no matter how long they were on dialysis. As expected, the best correlation between KDQOL-SF™ and laboratory data was electrolytes, nutritional status and HD efficiency. Overall, greater dose of HD on high-flux membranes, sufficiently correction of serum electrolytes toward normal value and adequate social and emotional interaction with HD patients can also reflect better outcome [23,24].Greater PHC and MHC score in QOL with less CRS value is found among younger, shorter dialysis duration, sufficiently correction of serum electrolytes including phosphate toward normal, adequate social and emotional interaction HD patients. Application with a combination of CRS and KDQOL-SFTM can significantly enhance their role as a justified non-invasive tool for the need to screen HD patients at risk of cardiac events [25,26].
Competing Interests
The authors declare that they have no competing interests.