


1. Introduction
Forty-four percent of the childhood deaths in the world are due to newborn deaths [1]. In Sub Saharan Africa the newborn mortality rate (NMR) is 29 deaths per 1000 live births whereas in Uganda it is 19 deaths per 1000 live births [1]. Worldwide, the main causes of newborn deaths are preterm and low birth weight complications, birth asphyxia and sepsis [1-4]. Unless global health programs address newborn deaths more effectively the new global target of reducing child mortality to 20 deaths per 1000 live births or less by 2035 will not be realised [4,5].
In response, many sub-Saharan African (SSA) countries are rolling out both community and facility based interventions for newborn care. Many including Uganda have introduced home visits and referral of sick newborns for facility–based care, following a recommendation by World Health Organisation (WHO) and the United Nations Children Fund ( UNICEF) [6].
The Uganda Newborn Survival Study (UNEST) was conducted between December 2008 to May 2012, in eastern Uganda, aiming to improve maternal and newborn outcomes, details of which have been described elsewhere [7] . UNEST used a community-based intervention to link communities and health facilities by training sixty one community health workers (CHWs) to conduct home visits to pregnant and newly delivered mothers. During the home visits, CHWs identified and referred sick newborns to health facilities for care and those born outside health facilities for immunisation and other postnatal care. Furthermore, UNEST conducted health facility strengthening activities to reinforce maternal and newborn care services in health facilities as described in Figure 1.

Sub-Studies conducted within UNEST have shown that: i) CHWs can identify and appropriately refer newborns for facility-based care [8] , and ii) caretakers of newborns largely complied to referrals to seek postnatal services, such as immunisation for healthy babies and treatment for those with danger signs [9] . The challenge is whether the health care facilities have the capacity to provide appropriate care for the referred newborns. Furthermore, some studies conducted elsewhere in SSA have reported inadequacies in logistics for newborn care in health facilities [10-14]. However, there is a dearth of data on whether the lower level health facilities in rural Uganda would be able to provide care to newborns referred by the CHWs. We conducted a study to assess the capacity of mainly lower level health facilities to provide care for newborns in rural eastern Uganda within the context of the UNEST for the main newborn mortality causes; preterm and low birth weight, birth asphyxia and sepsis.
2. Methods
2.1 Study setting
This study was conducted within the Iganga-Mayuge Health and Demographic Surveillance Site (HDSS) [15] located 120 kilometres east of Kampala, the capital city of Uganda. The HDSS consists of 65 villages that are predominantly rural. The total population under surveillance is approximately 80,000 people, the majority (56%) being below 18 years of age [16]. The main source of livelihood is through subsistence farming, followed by small scale retail trade.
2.2 Study design, population, tools and data collection
Between July and August 2013, we conducted a cross-sectional study to assess the capacity of 20 health facilities at different levels of primary health care, to provide care to sick newborns. The health facilities selected were those targeted by UNEST for strengthening (Figure 1.) during its intervention [7]. They included: one district hospital; one level IV health facility that offers out and in-patient care, caesarean section and minor surgery; six level III health facilities that offer in-patient and delivery facilities; and 12 level II health facilities that offer only out-patient services. A total of ninety -two health workers at these facilities also participated in face-to face interviews: fifty health workers assessed for knowledge and forty-two assessed for newborn resuscitation skill.
2.3 Study tools
Capacity of a health facility to care for newborn was defined to include: availability of equipment, supplies and drugs and competent health workers who are knowledgeable and skilled in newborn care. Thus three study tools were used to collect data: health facility checklist, knowledge semi structured questionnaire and a skill assessment checklist.
2.4 Health facility checklist
The health facility assessment was conducted using a modified version of the “Newborn Rapid health facility assessment checklist” developed by the Inter-agency Newborn indicators Technical Working group of Healthy Newborn Network (HNN). HNN is an initiative of Save the Children’s Saving Newborn Lives [17]. This tool measures whether a health facility has capacity to address the main causes of newborn deaths: birth asphyxia, preterm births/ low birth weight and infections [2]. The indicators measured by the tool include: newborn service availability, equipment and supplies, documentation, trained staff and supervision. Although this tool has not been used in Uganda before, the indicators are similar to those outlined in the Newborn Health Implementation Framework- Standards for Newborn Health Care Services of Ministry of Health, Uganda [18] . Furthermore, the tool was adjusted to align with the latter framework by adding items that were not captured by tool. These included: multivitamins, vitamin K, 50% dextrose, tetracycline ointment adrenaline and phenorbabitone. The modified tool was pre-tested in a non-study health facility. Following the pre-test, some questions were rephrased and re arranged to ensure clarity and logical flow. Elements assessed under each indicator are described in Additional file 1.
In this tool, equipment and supplies were scored for availability and functionality at the service area. Availability was captured as ‘observed’, ‘reported not seen’, and ‘not available’ while functionality was reported as ‘yes’ or ‘no’. An item was considered available if it was observed to be present and functional (for equipment) and not expired (for drugs). Service availability was reported as ‘able to provide today’, ‘provided in past 3 months’ and ‘ever provided in facility’ by answering ‘yes’ or ‘no’. A facility was deemed to offer the service if the interviewee reported that the service could be offered on the day of data collection. Health workers’ training in newborn services was scored as ‘trained within past 12 months’, ‘trained over 12 months ago’, and ‘no training’. Health workers were asked when they last received a supervision session, that is, in last three months, 6-12 months , more than 12 months ago and whether the supervision included observation while providing any form of newborn care. A health worker was considered trained or supervised if s/he was trained in the previous 12 months or supervised in last three months respectively by answering ‘yes’ or ‘no’. The tool was administered through face to face interviews to in-charges of the health facilities and staff on duty.
2.5 Health worker knowledge semi-structured questionnaire
Health workers were assessed on knowledge of newborn care using a tool adapted from UNEST training materials. The tool consisted of three components about essential newborn care services, the main causes of newborn mortality; i) preterm birth complications/ low birth weight; ii) birth asphyxia and iii) infections. The tool had a total of 64 multiple choices questions. All questions were weighted equally. A correct answer was awarded 1 point and an incorrect one 0 points. Thus the minimum score for knowledge was 0 and maximum 64 points. This was converted into a percentage score. Due to lack of national references an arbitrary pre–determined pass mark of 80% was set. This mark was set given that the questions were multiple-choice in nature and prompted, so the test was considered to be relatively easy. The health workers, who attained the pass mark or more, were considered “knowledgeable”, while those who obtained less than the pass mark were categorised as “not knowledgeable”. The tool was pretested prior to data collection and administered face to face by the researchers to prevent health workers from consulting each other about the appropriate responses.
2.6 Health worker skill assessment checklist
Health workers were assessed on newborn resuscitation skill with ambu-bag and mask technique on a mannequin (dummy baby). The checklist was adapted from the UNEST training materials. The checklist had four components: i) performing ten resuscitation steps scored as “done correctly” , “done incorrectly” and “not done”; ii) recognition of a successful or failed resuscitation procedure; iii) participant knowing what to do if the resuscitation was successful or not; and iv) participant knowing what to do after the resuscitation procedure was completed. The checklist was also pretested and administered face to face by the researchers.
Each item correctly done or answered was awarded 1 point, otherwise no point was awarded. All items were weighted equally, hence the minimum score for the exercise was 0 and maximum 23 points. Two consultant pediatricians agreed that a health worker would be considered “skilled” if he/she correctly performed: i) at least 7 out of 10 resuscitation steps (7 points), and ii) was able to recognise a failed or successful resuscitation and knew the appropriate actions to take if resuscitation fails and what to do when the procedure was completed (6 points). This translated into a pass mark of 13 points. The health workers obtaining these points or more were considered skilled in newborn resuscitation.
2.7 Data collection
Two Public health specialists and three research assistants with nursing training collected data for health facility assessment and conducted interviews to health worker knowledge in newborn care. Two paediatric consultants conducted the newborn resuscitation skill assessment among the health workers. The health facilities were assessed for presence of health workers 24 hours all the seven days of the week using available duty schedules, equipment, drugs and supplies, protocols and guidelines, forms and registers and whether the health workers were trained and supervised in newborn care. Health workers assessed for knowledge of newborn care were those on day time duty at service areas where newborn care is likely to be offered including: outpatient department, antenatal, postnatal and labour wards. The skills assessment for resuscitation of newborns was conducted among health workers who had participated in newborn resuscitation training between January 2009 and December 2011 during the implementation of UNEST project. The consultant paediatricians observed the health workers as they performed the resuscitation procedure on the mannequins using a checklist.
2.8 Data analysis
All the data were checked for completeness and entered in the computer using EPI Data software and exported to STATA version 10 (Stata Corp, TX, USA). Proportions of health facilities with the different items (equipment, supplies, and drugs) and offering delivery and newborn care services were computed. Mean availability index and scores and were computed using the Service Availability and Readiness Assessment (SARA) method , developed by WHO for measuring health systems readiness in service delivery [22], as used by O’Neil et al., to assess service delivery in six countries [23].
The proportions of health workers who had trained in newborn care, those who had received supervision and those knowledgeable about newborn care were also calculated. The overall median score and median scores for each of the three knowledge areas of: preterm/ low birth weight, birth asphyxia and infection were determined. Furthermore, differences in health workers’ knowledge by facility ownership were examined. The proportion of health workers skilled in newborn resuscitation was computed and stratified by health worker characteristics of cadre, and facility type. For all the analyses, the differences between groups were tested using Fisher’s exact test and the level of significance was considered at <0.05.
2.9 Ethical approval
Makerere University School of Public Health Higher Degrees Research Committee and the National Council of Science and Technology approved the study protocol (Ref. SS2660). All study participants were requested to give written informed consent prior to the interviews. Confidentiality was observed by use of identification numbers so that results could not be traced back to the participants. Permission was also sought from the management of Iganga– Mayuge Health and Demographic Surveillance Site.
3. Results
3.1 Availability of newborn care services equipment, drugs, supplies, registers and protocols
A total of 20 health facilities were assessed: 12 at level II, six at level III, one at level IV and one general hospital, of which majority (15) were government-run (public) and five were private not for profit (PNFP). Fifteen of the 20 health facilities offered newborn care and at all these facilities, a skilled provider was stated to be available 24 hours including weekend days from the available work schedules.
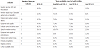
First level facilities (Level II) had the lowest (31%) availability score for resuscitation equipment compared to the hospital/level IV (71%) and those at level III (74%). None of the level II facilities offered kangaroo mother care (KMC) services for preterm/ low birth weight, while the availability score for this service was 67% for level III and 100% for the hospitals/ level IV. Availability score for newborn sepsis drugs was 8% for level II, 67% and 75% for level III and the hospital/ level IV, respectively. For newborn protocols availability scores were 25%, 19% and 18% for hospital/level IV, level III and level II, respectively. Other indicators are shown in (table 1). An additional table file shows this in more detail (Additional file 1).
3.2 Knowledge of newborn care by health workers
Of the 50 health workers assessed for knowledge of newborn care, nurses n=20, (40%) were the main profession. Eleven (22%) of the health workers knew all the definitions of a preterm and low birth weight baby, 46 (92%) correctly defined KMC and 42 (84%) correctly defined asphyxia. Forty- six (92%) correctly named eight or more newborn danger signs, preterm (low-birth weight) being the least known by 36 (72%) (Table 2).

Overall, 33 (66%) of the health workers, scored above the pass mark of 80%. The overall knowledge median score was (84%) (Interquartile range (IQR) 77%, 88%). ‘Infection’ was the most, and ‘preterm complications/low birth weight’ the least known newborn areas, with 42 (84%) and 23 (46%) health workers scoring above 80%, in each area respectively. Overall, a higher proportion of health workers from public health facilities 26/34(76%) scored the pass mark of 80% or more, than those from private not for profit (PNFPs) facilities 7/16 (44%) (p-value = 0.03) (Table 3).

3.3 Training and supervision of health workers on newborn care
Out of the 50 health workers, 42 (84%), reported to have received training in at least one of the following newborn care components within one year prior to this study: Newborn resuscitation using ambu-bag, early and exclusive breastfeeding, newborn infection management (including injectable antibiotics), sterile cord cutting and appropriate cord care, thermal care (including immediate drying and skin-to-skin care), KMC for low birth weight babies, special delivery care practices for preventing mother-to-child transmission of HIV, use of corticosteroids for preterm labor, goal oriented antenatal care, essential newborn care, and partographs. Out of the 50 health workers, 41(82%) had received support supervision within the three months prior to the study. Twenty- one (42 %) of health workers received supervision from their seniors within the health facility, and had been observed as they provided newborn care. Sixteen (32%) had been directly observed by supervisors from district and national level as they offered newborn care.
3.4 Newborn resuscitation skills
Of the 42 health workers assessed for newborn resuscitation skill, 20 (48%) were midwives and an equal proportion worked in the hospital. The median skill score was 12/23 (IQR 5, 16). Seventeen (40%) were considered skilled in newborn resuscitation and out of these, a majority 11(65%) worked in the hospital. Equal proportions of nurses and midwifes 8/17(47%) were considered skilled. There were no significant differences among the skilled health workers by cadre or health facility type.
4. Discussion
In this study we show that health facilities in this setting largely had staff to provide newborn services all the time of the day. Also, health workers were generally knowledgeable in newborn care, although their skills in newborn resuscitation were unsatisfactory. Many of the health workers had received training in at least one newborn care component and had been supervised and mentored during work. The admitting health facilities (hospital, Health Centre (HC) IV and HCIIIs) offered KMC services, indicating that preterm and low birth weight babies could be supported. However, the health facilities had inadequate equipment, drugs and supplies, in some cases due to stock-outs or non-replacement of non-functional equipment, and in other cases by policy. For-instance by policy, level II facilities are not stocked with medicines that are recommended for treatment of newborns with septicaemia.. A few of the facilities had the protocols to guide the staff in management of newborns. Our findings add onto the existing evidence that health facilities in SSA are inadequately prepared to care for newborns due to lack of essential inputs [10-14].
Uganda largely has adequate policies and guidelines to support delivery of newborn services with one exception: drugs to treat newborn sepsis are not allowed at the first, most accessible level of the formal health system which receives a majority of the sick newborns [9] referred by CHWs to health facilities [8]. While some countries in Asia are opting for community based sepsis treatment [19,20] , Uganda as many African countries opted to refer newborn with suspected septicemia to health facilities for assessment and treatment. We have earlier shown that CHWs are largely able to identify sick newborn [8], and parents take their sick newborns to the nearest facility particularly a level II [9] , however, the newborns do not receive the expected care since the Uganda essential medicine list does not provide for the relevant medicines at this level of health service delivery [21]. It was not therefore surprising that we found such medicines largely absent at these facilities. There is need for revision of this policy to bridge this gap. We argue that, sepsis treatment needs to be available at the most accessible health facility level, which will require a policy change in Uganda. Implementation of essential care for the newborns in health facilities remains a challenge not just in Uganda but also in other low income countries [22]. Level II health facilities are the majority in the districts, nearest to the communities and are the first points of contact with the formal health system where communities are expected to seek health care as described in the Uganda health strategic plan [23] . We have earlier shown that 77% of caretakers sought newborn referral care from public lower health facilities and only18% from the hospital [9]. Referral of sick newborns from first level health centres to hospital does not seem like a realistic alternative. Peterson et al., in their study under integrated management of childhood diseases, also demonstrated that completion of newborn referrals from lower level facilities to higher ones hardly happened, increasing the risk of death of these babies. Only two in ten of children aged 1week to 2 months completed referrals from level II facilities to hospitals for referral care, due to barriers like lack of money and transport problems [24]. Furthermore, Mbonye et al., in their analysis of newborn survival in Uganda in the last decade, echoed a similar message that the most essential treatment procedures for newborns are at a service level (HC- IV) which many families may not access [25]. Therefore, the current policy barring level II health facilities from stocking medicines like injectable gentamycin to treat newborn infections should be re-evaluated to enable the health workers at this level to treat sick newborns.
We found that most of the health facilities could provide normal delivery services 24 hours, including eight level II facilities, although at this level of service the policy stipulates only emergency deliveries. The level II facilities were providing delivery services because in some cases the district leadership operationalised them to conduct normal deliveries. In other scenarios it is because the staffing norm at level II includes a midwife whose duty is to conduct antenatal and emergency deliveries, but due to demand by the communities, normal deliveries are conducted. In both instances, the midwives are automatically exposed to newborns that may require resuscitation, and/or preterm and low birth weight interventions like KMC, yet the facilities are not equipped for these services. While we are not advocating that all HCIIs should conduct deliveries, our view is that the Ministry of Health should consider amending policies and guidelines to provide level II facilities that conduct normal deliveries, with basic newborn resuscitation equipment and KMC.
We found that many health workers had received support supervision either internally or from district and national level, but many times the supervision was not done when the health workers were offering newborn care (hands-on), which might have contributed to inadequate skills in newborn resuscitation among two thirds of the staff. Another possible explanation for insufficient skill could be allocation of staff as described by Vesel et al., in Ghana, where staff were working at service points where their newborn resuscitation skills were not exploited, compromising the quality of newborn care offered in the health facilities [11]. Equipping and maintaining competent health workers at health facilities to address the main causes of newborn death, would at a larger extent enhance the progress towards achieving MDG-4 by 2015 in Uganda.
We found that there were more health workers in the public health facilities who were considered knowledgeable in newborn care than in the private facilities. This could partly be due to uneven supervision and mentorship, where emphasis has been put on the public facilities. This calls for strengthening and involvement of private health facilities in district training activities for newborn care.
As Uganda scales up community based newborn care through Village Health Teams [26], health facilities at all levels of service must at the same time be strengthened, so that they are prepared to offer care to the referred newborns. This includes providing newborn sepsis drugs to all level II facilities to treat newborn sepsis, and ensuring that wherever deliveries are conducted there is also capacity to take care of the newborn. Else empowering communities to seek care alone, without improving the health facilities may not translate into the desired reduction in newborn deaths. This was demonstrated in the NEWHINTS study in Ghana where findings showed that a community strategy of home visits and referring sick newborns to health facilities, without strengthening the latter did not result in substantial reduction in newborn mortality [27,28]. This study was conducted in an area and health facilities that had enjoyed a newborn intervention under the Uganda Newborn Study. Possibly, this means that our findings reflect a better situation than the typical one in Uganda. However, it is evident that further improvement in formal health system capacity to care for newborns is required even beyond what was done under the UNEST intervention, and that this may require policy changes in some instances.
5. Conclusion
Health-workers had good knowledge but modest skills for newborn care. Overall, higher level health facilities were more prepared for newborn care than the lower level facilities. The national essential drug policy should be revised to provide level II facilities with medicines that treat newborn sepsis. Health facilities that conduct deliveries should also provide good quality preterm/low birth-weight and asphyxia care, irrespective of the level of service.
Competing Interests
The authors declare that they have no competing interests. The opinions expressed in this paper are those of the authors and do not necessarily reflect views of the funders neither the institutions of affiliation.
Author Contributions
CKN conceived and designed the study together with JK, PW, and SP. CKN, AT,NH, GN and SN collected data with supervisory guidance provided by JK, GT,PW and SP. CKN, FN, PW and SP conducted data analysis. CKN prepared the first draft guided by GT JK, PW and SP. All authors reviewed and approved the final manuscript. SP and PW contributed equally as senior authors.
Acknowledgments
This study was funded in part by the Swedish International Development Cooperation Agency (Sida) and Makerere University and Save the Children (USA) through a grant from the Bill &Melinda Gates Foundation that sponsored UNEST. The funders had no role in study design, data collection and analysis or preparation of the manuscript. We also acknowledge the partial funding provided by the African Doctoral Dissertation Research Fellowship award, offered by the African Population and Health Research Center, in partnership with the International Development Research Center. We thank the Uganda National Newborn Steering Committee, Iganga and Mayuge district authorities, the health workers and research assistants who participated in the study and the management of Iganga- Mayuge HDSS.