



1. Introduction
The incidence of injury during kendo practice is low compared with other sports [1], but low back pain is common in persons continuing kendo. This is a characteristic of sports disorders in kendo [2]. Moreover, it is occasionally reported that low back pain frequently occurs in kendo players [3-6]. Generally, it is said that collapse of the spinal alignment leads to the occurrence of low back pain in ordinary persons as well as in athletes [7-10]. Spinal muscles have been considered to be important as a role to prevent the collapse of spinal alignment. Because the major psoas muscle and lumbar multifidus muscle are particularly involved in postural maintenance and lumbar segmental stability, they have been considered important in preventing low back pain [11-13]. In recent years, noninvasive MRI evaluation has been conducted to examine the relationship between low back pain and the cross-section areas of the spinal muscles [14-16]. Therefore, we investigated the characteristics of the spinal alignments and spinal muscles for the purpose of obtaining indicators to study the factors of low back pain in male university kendo players.
2. Subjects
The subjects were 20 out of 37 male kendo players of the university from whom consent was obtained after explanation of the major purpose of the present study. The average age was 19.6 ±0.7 years, the average duration of kendo experience 12.1 ±1.9 years, the average height172.5 ±5.4 cm, and the average weight 71.7 ±7.1 kg. The study received approval from the Ethics Committee of Graduate School of Sport and Exercise Science, Osaka University of Health and Sports sciences
3. Methods
We evaluated the spinal alignments and spinal muscles(a ratio of the multifidus muscle to the major psoas muscle).
3.1 Alignment evaluation using spinal X-ray pictures
X-ray pictures of the frontal and lateral spines in standing and stepping postures were taken, and the degrees of lateral spinal curvatures in the X-ray images were measured by the Cobb method. For the degrees of lumbar flexures, the angle between the superior margin of the L1 vertebral body and the inferior margin of the L5 vertebral body was measured according to the Cobb method (Figure 1). And the degrees of lumbar flexures were compared between standing and stepping postures. Moreover, when a lateral curvature of the spine was observed, the degrees of lateral spinal curvatures were compared between standing and stepping postures as with the degrees of lumbar flexures. In addition, the players were instructed to make striking motions to the front head close to actual practice, and a stepping posture was set as an instantaneous posture when the right foot touched the floor.

3.2 Evaluation of the spinal muscles by lumbar MRI(a ratio of the multifidus muscle to the major psoas muscle)
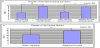
Cross-sectional T2-weighted images of the lumbar spine were taken by the MRI device, Achieva 1.5T HP(from PHILIPS), and the muscle area of the superior surface of the L3 vertebral body sliced perpendicular to the alignments of the multifidus muscle and major psoas muscle was measured by tracing the outlines of the right-andleft iliopsoas muscles and multifidus muscles with a mouse using the workstation, View Forum (from PHILIPS) (Figure 2). Then, a ratio of the multifidus muscle area to the major psoas muscle area (the multifidus muscle area /the major psoas muscle area ×100% was defined as a ratio of the multifidus muscle to the major psoas muscle) and a ratio of the left multifidus muscle area to the right multifidus muscle area(the left multifidus muscle area/the right multifidus muscle area ×100% was defined as a ratio of the right-and-left multifidus muscles) were measured to examine the right-and-left differences in the ratios of the multifidus muscles to major psoas muscles and the correlation between the spinal alignment and the spinal muscle. The measurements were performed twice by one radiological technologist in order to calculate the average value.

3.3 A correlation between the spinal alignment and the spinal muscle
- A correlation between the degree of change of lumbar flexurein stepping motion(the flexure degree in stepping posture -the flexure degree in standing posture) and the right-and-left average value of the ratios of the multifidus muscles to major psoas muscles.
- A correlation between the lumbar flexure degree in standing posture and the right-and-left average value of the ratios of the multifidus muscles to major psoas muscles.
- A correlation between the lumbar flexure degree in stepping posture and the right-and-left average value of the ratios of themultifidus muscles to major psoas muscles.
- A correlation between the degree of change of the lateral spinal curvature in stepping motion(the lateral curvature degree in stepping -the lateral lumbar curvature degree in standing) and the ratio of the right-and-left multifidus muscles.
3.4 Statistical analysis
We examined the lateral spinal curvature degree and the lumbar flexure degree in standing and stepping postures using the paired t-test. Moreover, we compared the right-and-left differences in the ratios of the multifidus muscles to major psoas muscles by spinal MRI and studied them using the paired t-test. The correlation between the lumbar alignment and the spinal muscle was studied with the Pearson correlation coefficient test. The statistical processing software, SPSS 11.0 for Windows was used in the above statistical analysis, and each significance level was less than 5%.
4. Result
4.1 A comparison of the lateral spinal curvature degrees in standing and stepping postures
For the lateral spinal curvatures during stepping motion, all 20 players showed convex lateral curvatures in the left lumbar spine and the right thoracic spine. The average value of the lateral curvature degrees was Cobb angles 8.4 ±1.6° in the lumbar spine and 8.9 ± 2.3° in the thoracic spine. In standing, 3 players had good conditions of the lateral spinal curvatures, but 17 players showed convex lateral curvatures in the left lumbar spine and the right thoracic spine as with stepping motion. The average value of the lateral curvature degrees was Cobb angles 4.3 ±2.4° in the lumbar spine and 5.0 ± 2.8° in the thoracic spine. In addition, the lateral spinal curvature degree in stepping significantly increased both in the lumbar spine and thoracic spine as compared to standing (p<0.01)(Figure 3a).
4.2 A comparison of the lumbar flexure degrees in standing and stepping postures
The average value of the lumbar flexure degrees was 27.5 ± 5.5° in standing and 39.0 ± 2.3° in stepping, showing a significant increase in stepping compared to standing(p<0.01) (Figure 3b).
4.3 A comparison of the right-and-left differences in the spinal muscles(a ratio of the multifidus muscleto the major psoas muscle)
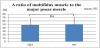
The average values of the ratios of the multifidus musclest o the major psoas muscles were 48.3 ± 19.6% in the right and 50.3 ± 20.8% in the left, showing no big difference (Figure 4).
4.4 A relationship between the ratio of the multifidus muscle to the major psoas muscle and the lumbar flexure
There was a significant negative correlation that when the ratio of the multifidus muscle to the major psoas muscle was low, the degree of change of the lumbar flexure was high (p<0.01) (Fig. 5a). Moreover, stepping motion showed no correlation between the ratio of the multifidus muscle to the major psoas muscle and the degree of change of the lumbar flexure, but standing postures had a significant positive correlation that when the ratio of the multifidus muscle to the major psoas muscle increased, the degree of change of the lumbar flexure increased(p<0.01) (Figure 5b, 5c).

4.5 A relationship between the ratio of the right-and-left multifidus muscles and the lateral lumbar curvature
There was no correlation between the degree of change of the lateral spinal curvature in stepping(the lateral spinal curvature degree in stepping -the lateral lumbar curvature degree in standing) and the ratio of the right-and-left multifidus muscles (Figure 5d).
5. Discussion
In the present study, the characteristics of the spinal alignments in the male university kendo players were convex lateral curvatures in the left lumbar spine and the right thoracic spine. Stepping motion caused an increase in the degree of change of the lateral curvature and lumbar flexure. It was indicated that this malalignment or alignment change provided kinetic loads such as compression, extension, and twist to the lumbar spine, which might lead to the occurrence of low back pain. In addition, Sakai [17] reported that lateral overloads due to sports activities might cause imbalance in the spinal support mechanism and develop sports-related lateral curvatures, leading to the occurrence of low back pain. In the present study, it can be considered that the occurrence of convex lateral curvatures in the left lumbar spine and the right thoracic spine is related to stepping motion in kendo. Stepping motion in kendo provides unbalanced movements such as a big step forward with the right foot and a kick backward with the left foot from the posture in which the right hand and foot are put in front and the left hand and foot in behind, which leads to twists of the lumbar flexure and pelvis to the left side. As a result, it can be considered that coupling motion with a twist of the inferior lumbar spine to the left side against the superior lumbar spine causes a right-sided flexion with a convex lateral curvature in the left lumbar spine [18-20]. Furthermore, it can be thought that a convex lateral curvature in the right thoracic spine moving in the opposite direction from the lumbar spine due to a countermovement of the thoracic spine developed in the spine in order to keep a right-sided movement of the gravity center in the base of the gravity center by the movement of lumbar spine [21,22]. In standing posture, however, 17 (85%) out of the 20 players showed lateral curvatures similar to those of the spinal alignment in stepping motion. From these results, it was considered that a lateral spinal curvature was likely to occur in kendo players practicing stepping motions characteristic of kendo for more than 10 years and was one of the physical characteristics. Additionally, the author’s past survey of the spinal alignments of kendo players suffering from low back pain showed lateral spinal curvatures due to stepping motions similar to those in the present study, but no lateral spinal curvatures due to standing postures [23]. The subjects of the survey were 5 high school students, 1 university student, and 2 adults aged 30 or over. Although their duration of kendo experience was 9 to 10 years, the high school students practiced kendo every day, and the university student and adults did it only twice a week. On the other hand, the subjects of the present study practice kendo almost every day, 6 or 7 days a week for 2 or 3 hours twice daily. High school students are doing everyday with practice hours 2 or 3 hours one daily, but the history of kendo was 6 to 7 years and less than 10 years. Therefore, the occurrence of lateral spinal curvature was probably related to the amount of practice as well as the duration of kendo experience. Generally, proprioceptive dysfunction due to abnormal distribution of paraspinal musclespindles [24] and asymmetric muscle weakness were confirmed in lateral spinal curvature [25,26]. However, because the present study showed no difference in the right-and-left average values of the ratios of the multifidus muscles to major psoas muscles and no correlation between the ratio of the right-and-left multifidus muscles and the lateral spinal curvature, a reduction in the balance of the right-and-left muscular strength is less likely to develop a lateral spinal curvature and is probably due to other factors, which could not be elucidated in the present study. Therefore, in addition to the factors, prevention of lateral spinal curvatures is an issue in the future. Lumbar flexure showed a negative correlation that when the ratio of the multifidus muscle to the major psoas muscle became low, the degree of change of lumbar flexure became high. For this reason, it can be considered that when the ratio of the multifidus muscle to the major psoas muscle is low, the degree of stress associated with lumbar flexure is high. A factor for which the ratio of the multifidus muscle to the major psoas muscle becomes low and the degree of change of lumbar flexure becomes high is considered not to be an increase in the degree of change of lumbar flexure during stepping but a decrease in the degree of change of lumbar flexure during standing. This is because there was no correlation in stepping and a positive correlation in standing between the ratio of the multifidus muscle to the major psoas muscle and the postures. We describe the reason why the ratio of the multifidus muscle to the major psoas muscle becomes low and the degree of change of lumbar flexure becomes low is probably that the multifidus muscle action, extension of the lumbar spine decreases [27] and the major psoas muscle action, flexion of the lumbar spine increases [28,29]. The rate of the multifidus muscle is low compared to the major psoas muscle. This is because the segmental stability of lumbar spine may reduce and become unstable. Because the multifidus muscle is abundant in proprioceptive receptors, it is believed that the multifidus muscle keeps the stability of each segment in cooperation with sensory feedbacks from articular capsules and ligaments [30]. Moreover, when the amount of activity of the multifidus muscle reduces, the spine is not sufficiently supported or protected by the central nerve system and sensory feedbacks. In return for it, the long is simus muscle or iliocostal muscle may contract excessively. Hirohashi et al. [31] described that muscular and fascial low back pain was common in kendo players with low back pain, and Waku et al. [32] described that low back pain in kendo players resulted from physical fatigue by continuation of kendo. For these reasons, it was considered that male university kendo players were at risk of having muscular fatigue due to excessive activity of the long issimus muscle or iliocostal muscle in terms of the physical characteristics stated above.
6. Conclusion
We investigated the characteristics of the spinal alignments (lateral spinal curvatures and lumbar flexures) and the spinal muscles (a ratio of the 9 multifidus muscle to the major psoas muscle in the superior margin of the L3 vertebral body) and the correlation between the spinal alignments (lateral lumbar curvatures and lumbar flexures) and the spinal muscles in male university kendo players. The spinal alignment showed lateral spinal curvatures with a curve convex to the right in the thoracic spine and that to the left in the lumbar spine during stepping motion, and 85% of the players had similar lateral spinal curvatures during standing. Furthermore, stepping motion of kendo provided a significant increase in the degree of lateral spinal curvature or lumbar flexure compared with standing. Particularly, a decrease in the ratio of the multifidus muscle to the greater psoas muscle produced a negative correlation that the degree of change of the lumbar flexure between standing and stepping was increased.
Key Point
- We investigated the characteristics of the spinal alignments(lateral spinal curvatures and lumbar flexures) and the spinal muscles(a ratio of the multifidus muscle to the major psoas muscle in the superior margin of the L3 vertebral body) and the correlation between the spinal alignments(lateral lumbar curvatures and lumbar flexures) and the spinal muscles in male university kendo players.
- The physical characteristics of the spinal alignments in male university kendo players are convex lateral curvatures in the right thoracic spine and the left lumbar spine, and an increase in the degree of change of the lateral spinal curvature and lumbar flexure during stepping.
- There was a negative correlation between the ratio of the multifidus muscle to the major psoas muscle in the superior surface of the L3 vertebral body and the degree of change of lumbar flexure.
- It was indicated that selective training of the multifidus muscle and increasing the amount of the muscle led to the prevention of low back pain
Competing Interests
The authors declare that they have no competing interests.