



1. Introduction
Majority of the hip osteoarthritis (OA) patients in Japan are secondary OA patients who are forced to change their life style to avoid undergoing total hip arthroplasty (THA) and re-operation for as long as possible. Thus, some of these patients prefer to endure mild pain rather than to undergo early operation. These needs warrant medical facilities that provide various types of care, including those that help control pain, maintain and enable physical functions and daily activities, and provide information regarding self-management. To address these needs of OA patients, the paradigm of rehabilitation must shift its aims and activities from simple physical maintenance and improvement to the overall mental and physical satisfaction of patients. There are some previous studies about relationship between OA hip and rehabilitation. Jigami [1] reported that aquatic exercise and land based muscle strength exercise improved lower extremities muscle strength and gait ability. Several other reports [2-5] also showed similar results. These studies, however, did not conclude that rehabilitation is effective to delay the deformity and postpone the orthopedic surgery. Recently, the importance of assessments of mental function and quality of life (QOL), in addition to physical function, has gained attention and internationally accepted rating scales such as SF-36, which can evaluate the mental states and QOL, as well as physical function, have begun to be widely used [6]. For evaluating hip OA patients, disease specific scales such as the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) and Harris hip score are also used. Most studies using these rating scales, however, aimed to compare the QOL before and after the surgical operation or physical rehabilitation intervention [1]. There is lack of studies that observed the natural course of QOL of hip OA patients, especially the worsening in the QOL, which encouraged patients to opt for surgical intervention. Our previous study of patients undergoing conservative treatment [7] showed that the patients instructed to perform active physical therapy by orthopedic doctors or physical therapists maintained significantly higher QOL scores than other patients. That study, however, was cross-sectional and retrospective study. We think that the timing of orthopedic operation greatly related to not only degree of hip pain but also decrease of QOL. Thus, we consider that subjects who decided the orthopedic operation, due to a decrease in physical and mental QOL, show a characteristic trend among the sub-items of the SF36. In the present study, we investigated the longitudinal time course of QOL in patients under conservative care and patients who received THA by comparing their QOL scores along with the rehabilitation and life style parameters.
2. Methods
Sixty-three female patients (age 58.7±7.1 years) of hip OA under continuous conservative treatment were surveyed intermittently by SF-36v2 (a modified version of SF-36) and an additional questionnaire developed by us. The period of survey was from April 2009 to April 2011. The survey was performed by mail 4 times for each patient with 6-month intervals. Patients who had received THA before the last mail survey were designated as the THA group and others were designated as the non-THA group. The questionnaire content included rehabilitation (contents, beginning time, durations and places etc.), living environment (type of beds, availability of family members etc.), and the level of ADL (stand-up and sit-down, out-door walking, walking up and down on stairs, putting on and taking off socks and shoes, clipping of toe nails etc.). Mann-Whitney U-test and χ2- test were used for comparison between the two groups and p-values of less than 0.05 were considered significant. Kruskal-Wallis test was used for the comparison of results of 4 consequent questionnaires. Non-THA group was further divided into two sub-groups based on the results of questionnaire and analyzed by Mann-Whitney U-test. The study was approved by the Ethical Review Board of the Tokyo Metropolitan University, Japan.
3. Results
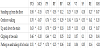
Six patients received THA operation during period of survey and were designated as the THA group. Among the remaining 57 patients, 37 patients answered all four subsequent questionnaires and were designated as non-THA group. Table 1 shows the characteristics of two groups at the beginning of survey. Significant differences were observed between two groups in terms of “age” and “continuing rehabilitation in the hospital” (p<0.05).

*:non-THA group-THA group: Mann-Whitney U test p<0.05 **:non-THA group-THA group: χ2 test p<0.05.
Figure 1 shows the average of the eight-scale scores of SF-36v2. The scores of physical functioning at the time of the first survey were significantly lower in the THA group compared to the non-THA group (p<0.05) and Odds ratio was 1.045 (95%CI; 1.004-1.088).

Figure 2 shows the average scores of SF-36v2 of four subsequent surveys in the non-THA group. None of the elements showed a significant difference among four average scores. The non-THA group was further divided into the rehabilitation continuing group (RC group; n=8) in the hospital and the discontinuing group (non-RC group; n=29) from the result of the questionnaire. The scores of elements of physical activity were significantly higher in the RC group when compared to the non-RC group. Table 2 shows correlation coefficients between the subjective ADL scores and QOL scores. Physical functioning showed significant correlation with all of ADL scores p<0.05). Especially, it showed a strong correlation with “standing up from the floor”, “walking up and down the stairs”, and “outdoor walking” (p<0.05).

PF: Physical functioning, RP: Role physical, BP: Bodily pain, GH: General health, VT: Vitality, SF: Social functioning, RE: Role emotional, MH: Mental health, p<0.05.
4. Discussion
It has been reported [7] that no significant correlation exists between the clinical stage evaluated by X-ray or CT-scan imaging and the subjective QOL in conservatively cared female hip OA patients. QOL of hip OA patients has been reported to be worse than that of healthy people. While some reports suggest that the physical exercise intervention of hip OA patients can improve patient’s QOL, other reports showed no significant improvement [2,8]. Thus, it remains uncertain of how the QOL of hip OA patients changes during the conservative treatment and whether an active intervention can improve QOL or not. In this study, we found that the scores of “physical functioning” in SF-36v2 at the beginning of survey were significantly lower in the THA group than that in the non-THA group. This indicated that the “physical functioning” is more important indicator of the necessity of THA than other sections of SF-36v2. In the non-THA group, patients who continued rehabilitation in the hospital scored higher for the “physical functioning” than the ones that discontinued rehabilitation at the last survey. Among the ADL score, “stand-up and sit-down on the floor”, “out-door walking” and “up and down of the stairs” showed a strong positive correlation with the “physical functioning”. These results indicate that the “physical functioning” is the most important factor in patients’ decision to receive THA and the improvement of ADL scores concerning indoor and out-door free movement may postpone patients’ decision to receive THA. These results are consistent with previous studies [5,6], which reported that the QOL of hip OA patients depended on the habit of physical exercise and ADL. A long-term observation of the QOL of hip OA patients may contribute to the development of a better intervention strategy for conservative care without THA by elucidating the characteristics of QOL change that may help OA patients’ decision to receive THA.
Limitation of this study is that the number of THA patients was relatively small. In addition, the timings of questionnaire were simultaneous in all subjects and independent of the timings when the THA patients decided to receive THA. In further research, therefore, it is necessary to expand number of THA patients and also to include the subjects such as outpatient hospital and community dwelling OA hip patients continuing conservative treatment.
5. Conclusion
“Physical functioning” of SF-36v2 is an important factor which helps hip OA patients to decide on receiving THA. The continued rehabilitation for physical activities such as standing up and sitting down on the floor or practical walking is important for improving “physical functioning” score and may help patients to avoid THA.
Competing Interests
The authors declare that they have no competing interests.
Acknowledgments
We are grateful to the members of Nozomi-kai (Japanese patients group of hip osteoarthritis) and Ms. Funahashi for their cooperation.