



1. Introduction
Work-related musculoskeletal disorders and complaints cause seriouspuclic health problem in many countries. These problems could effect individuals work performance and day of absent.
Scapular dyskinesis is defined as alterations in the normal position of the scapula and the patterns of scapular motion during scapulohumeral movements [1,2]. One or more asymmetric positions of the scapula are called ‘dyskinesis’. Kibler has defined three dyskinetic patterns. Type I is the prominence of the inferomedial border of the scapula due to abnormal posterior tilt the scapula; when this type occurs isolatedly, the scapula may be lower than the opposite side. Type II consists in the prominence of its entire medial border of the scapula. These types could be seen with superior labrum injuries (SLAPs). Type III displays upward rotation of the superomedial border of the scapula around of the scapula , this type can be seen when the size of the acromiohumeral space decrease or potential rotator cuff injuries occur. Also Type IV is defined as normal scapular position and motion [2].
There are many factors which are bone and joint related, neurologic causes that lead to dyskinesis. Bone related factors define as thoracic kyphosis, nonunion/malunion clavicle fracture. Joint-related factors are high-grade acromioclavicular (AC) instability, AC arthrosis, glenohumeral joint derangement and neurologic factors such as cervical radiculopathy or spinal nerve palsy [3]. Also pain, soft tissue tightness, strength imbalances, muscle fatigue and awkward posture would cause abnormal scapular kinematics [4].
Postural malalignment is often reported as the cause of workrelated musculoskeletal disorders among office workers [5]. Neck and shoulder pain are common in the general population. Work related pain can impact on the ability to perform normal daily activities and the resultant treatment costs and work loss contribute to a substantial economic burden for both the individual and society. Shoulder pain could be results of extrinsic risk factors such as repetitive overhead use especially more than 60° of shoulder elevation, sustained overhead work, and higher loads raised above shoulder height. Intrinsic risk factors such as forward head, rounded shoulder posture, altered scapular kinematics and muscle activity play an important role in presence of scapular dyskinesis [6]. With forward head posture, thoracic kyphosis angle will have increased so that position of the scapula will have altered [7]. Furthermore neck pain occur result of scapular downward rotation. Scapular downward rotation increase upper trapezius muscle length while not transfer the weight of an upper extremity load to the sternoclavicular joint, and increased levator scapulae muscle stiffness which will increase compressive load on the cervical spine.Repetitive and excessive stress in the cervical region cause cumulative micro trauma to tissue which will lead to neck pain, and limite range of motion [8]. There is relationship between chronic neck/shoulder pain and scapular dyskinesis. Scapula is a bridge between the shoulder and the cervical region and plays a very important role in providing both mobility and stability for neck/ shoulder region [9]. The association between scapular dyskinesis and neck pain has been well shown in some studies. Patients with scapular dyskinesis are also more likely have pain in the shoulder, scapular and neck region [24].
Physical risk factors such as prolonged sitting and neck flexion have been reported as predictors of neck pain in a mixed population of workers from various industry, health and professional settings [25]. However these and other physical factors have not been investigated in office workers. This pilot study will be helpful for further studies being the first study that evaluate the scapular dyskinesis and pain levels in office workers.
The purpose of this study was to evaluate the scapular dyskinesis and work-related pain level in office workers.
2. Material and Methods
36 office workers were participated in this study. Inclusion and exclusion criterias were as follows.
The inclusion criteria:
- Ages between 20 to 50
- Working at least 1 year
- Working at least 20 hours a week.
- Having full range of motion in neutral position,45 shoulder abduction and 90⁰ shoulder internal rotatio
The exclusion criteria
- Obese individuals (BMI> 39 kg / m2)
- Having surgical operation related upper extremities
- Taking physiotherapy treatment in the last 3 months
- Having structural scoliosis , neurological or systemic diseases.
2.1 Lateral Scapular Slide Test (LSST)
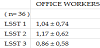
Lateral Scapular Slide Test (LSST) was used to evaluate the scapular dyskinesis. LSST assess scapular asymmetry under varying load positions. Measurements of scapular position are taken while scapular position with the arm abducted 0, 45, and 90 degrees in the coronal plane (Figure 1,2,3). Distance from the inferior angle of the scapula to the spinous process of the thoracic vertebra in the same horizontal plane was measured in all 3 position.If the distance is greater than 1.5 cm, it means LSST is positive [12].



2.2 QuickDASH
For evaluation activities and functionality of upper extremity of individuals , the shortened version of the Disabilities of the Arm, Shoulder and Hand questionnaire (QuickDASH) was used. The QuickDASH is an shortened version of the DASH by extracting 11 items from the original DASH.. 0 means Each item of the Q-DASH is scored between 1 (no difficulty at all) and 5 (unable to do), with higher scores indicate greater disability.QuickDASH score is calculated by [(sum of n responses) / n - 1] × 25], where n = total number of questions answered. If three or more items are not answered, this score cannot be calculated. Total score were obtained by conversion to a 100-point scale [13,14,15].
2.3 Neck Disability Index (NDI)
Neck Disability İndex (NDI) was used for functional evaluation of the neck. NDI contains 10 items that 7 related to activities of daily living, 2 related to pain, and 1 related to concentration. Each item is scored from 0 to 5, with higher scores corresponding to greater disability [16] .Total scores vary from 0 to 50, where 0 is considered “no activity limitation” and 50 is considered “complete disability.” Also interpretation of total scores means : 0 to 4, no disability; 5 to 14, mild disability; 15 to 24, moderate disability; 25 to 34, severe disability; and greater than 35, complete disability [17].
2.4 Visual Analogue Scale (Vas)
Before the study , assessment that will be made to individuals explained to office workers and informed consent form has been signed. After questioning sociodemographic characteristics of individuals, visual analogue scale (VAS) was used for assessing the severity of pain. This scale consists of a 10 cm line with the end points no pain ( 0 cm) and worst pain (10 cm). Participants were asked to mark on the line that represented their current pain intensity about neck and upper extremities. Then, the distance from the point that was marked to 0 mm point was measured by a ruler [10]. According to mean value of VAS , 0 stated no pain , 1-4 stated mild pain, 5-6 stated moderate pain, 7-10 stated severe pain [11]. The pain localization was questionned to individuals with body localization diagram.
2.5 Statistical Analysis
SPSS Statics 20.0 was used for statistical analysis. Numeric variables were determined by mean and standard deviation.
3. Results
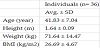
36 office workers participated in this study. The average age , height, weight and body mass index was 41,83 ± 7,04 year , 1,64 ± 0,09 m, 71,64 ± 14,47 kg , 26,69 ± 4,67 kg/m2 respectively. Table 1 describes the Sociodemographic characteristics of individuals. 41,7 % of office workers have positive lateral scapular slide test while 58,3 % of them have not. The mean value of difference between distance from the inferior angle of the scapula to the spinous process of the thoracic vertebra in three position are 1,04 ± 0,74 , 1,17 ± 0,62 , 0,86 ± 0,58 cm respectively as shown in table 2.
The mean value of Q-DASH in participants was 6,06 ± 11,92 and neck disability index was 4,78 ± 3,2. The VAS scores of participants was evaluated at rest position. The VAS scores was 2,50 ± 3,33 cm. Table 3 shows mean values of Q-DASH , NDI and VAS.Also the localization of the pain was questioned to individuals. 35,7 % of them had low back pain, 28,6 % of them had neck pain , 14,3% of them had upper back pain, 14,3% of them had shoulder pain and also 7,1 % of them had ankle pain as shown in figure 1.
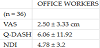
VAS:Visual analogue scale , Q-DASH : Quick-DASH , NDI: Neck Disability İndex.
4. Discussion
We found that the incidence of scapular dyskinesis in Cypriot office workers was particularly high. There are many studies about office workers in the literature but we especially want to evaluate all of the parametres that related musculoskeletal disorders such as scapular dyskinesis, functional impairment and work-related pain in office workers. Musculoskeletal complaints about upper extremity among office workers are known to be associated with both work-related physical and psychosicial factors.

Scapula is a bridge between the shoulder complex and the cervical spine which plays an important role in ensuring Scapula is a bridge between the shoulder complex and the cervical spine which plays an important role in ensuring both mobility and stability of the neck/shoulder region. The association between abnormal scapular positions, motions and problems related to glenohumeral joint has been well established in the literature, whereas studies investigating the incidence of scapular dysfunction in office workers have not recently begun to emerge.%41.7 of the individuals face with scapular dyskinesis in our study. It was found to have problems in activity and function of the upper extremity. These problems can occur because of work-related physical and psychological factors, earlier experience of neck/shoulder injury, female gender, low pain pressure threshold, and high intrinsic efor so that quality of life decreases [18]. Office workers generally works at static position with forward head posture and greater shoulder elevation range of motion. Prolonged static posture and increased muscle load will lead to the development of symptoms in the upper extremity [19]. This position has been shown to change the normal plane orientation of scapula. Weakness in the posterior rotator cuff muscles and parascapular muscle imbalances cause changing of scapular positions [20]. Hush et al. indicated that the 1-year incidence of neck pain in office workers was 49 %. The quantitative results show that physical, workplace and psychosocial factors lead to this pain.Factors like gender, exercise frequency, mobility of the cervical spine and psychological stres were revealed that can impact on the risk of developing neck pain [21]. In our study the incidence of neck pain was %28.6.Ranasinghe et al. found that incidence of arm , neck and shoulder complaints was 56,9 % at office worker using computers. This condition established relationships with work posture (rotation of the head and neck, asymmetric body ) and poor work habits (sitting in one position for a long time , repetitive movements or working with lifted shoulders ) [22]. We will investigate the work posture and conditions of office workers in our subsequent study.Eltayeb et al. found that neck and shoulder compliants significantly more often than the other upper extremity region at office workers and they associated these compliants with poor head and body posture and work demands [23]. Like these studies,our finding that work posture lead to changes in the musculoskeletal system at office workers. Scapular dyskinesis was especially observed in individuals who had problems in the activity and function of the upper extremities.A number of previously published studies concerning shoulder and neck pain have been included both mechanical and psychosocial exposures.Better work conditions and posture alignment should be ensured in office workers so that may be protective of scapular dyskinesis and pain. This study have several limitations.The age of participants was not homogen and the propotions of their gender was different.
5. Conclusion
This is the pilot study that held in North Cyprus. The incidence percentage of scapular dyskinesis was found high at office worker. Although the number of people affects the reliability of the results, study will be developed by increasing the number of people in the future.
Competing Interests
The authors declare that they have no competing interests.