



1. Introduction
The lifetime prevalence of neck pain in Western populations has been estimated at around 70%, while annual or point prevalence rates range from 10% to 35% [1-3]. Chronic neck pain (CNP) can be defined as pain experienced in the anatomic region of the cervical spine between C1 and C7 and the surrounding musculature only, in accordance with the criteria set by the International Association for the Study of Pain and the American Pain Society which defines the condition as chronic when pain persists beyond 3 months regards the normal tissue healing time [4,5]. Many factors contribute to the development of CNP and many have not yet been identified. However, it is known that pain can become more complex in its pathophysiology than its original injury. Chronic musculoskeletal pain, like CNP for instance, usually develops as a result of an injury or an insult followed by neurogenic inflammation, hyperalgesia, and allodynia; then occurs a central sensitization followed by a loss of nociceptive control [6,7].
Clinical guidelines for CNP treatment recommends cervical mobilization, thoracic spine thrust manipulation, flexibility exercises for specific muscles group (anterior/medial/posterior scalene, upper trapezius, elevator scapulae, pectoralis minor, and pectoralis major), the use of coordination, strengthening, and endurance exercises to reduce neck pain and headache. To improve recovery in patients with whiplash-associated disorder, clinicians should educate the patient to be more confident in coming back at a well-being status [8]. It is well known that there are many therapeutic strategies for CNP, but the long term effects of individual rehabilitation approaches are limited. Between the flexibility muscles exercises, the relaxation of myofascial trigger points (MTrPs) in the splenius capitis, elevator scapulae, or upper trapezius muscles as a clinical entity seems to contribute to CNP [9]. Moreover, the reported pain elicited by active MTrPs in the neck and shoulder muscles has been shown to contribute to symptoms of mechanical neck pain [10,11]. An MTrP is defined as a hyperirritable focus within a taut band of skeletal muscle that is painful on compression and that, when stimulated (usually by compression, percussion, or needling), can evoke a characteristic pattern of reported pain and related autonomic phenomena [12].
However, no studies have investigated the effects of mesotherapy on MTrPs to improve chronic neck pain and function. Moreover the efficacy of mesotherapy was confirmed as a viable option as an additional treatment in an overall rehabilitation treatment planning in other research on chronic lower back pain [13]. Mesotherapy was introduced 50 years ago by Michel Pistor, a French physician who used this technique as a novel analgesic therapy for a variety of rheumatologic disorders. Mesotherapy is a minimally invasive technique that consists of subcutaneous injections of drugs and, occasionally, plant extracts, homeopathic agents, or other bioactive substances [14-16].
The pharmacological effects of intradermal administration do not entirely account for the observed clinical benefits of mesotherapy. The needle dry prick activates the cutaneous and subcutaneous receptors (reflex effect), and it is thought that endorphin levels actually increase after the introduction of the needle which is also believed to be true in acupuncture [17,18]. Microinjections, without drugs, seem to facilitate the rebalancing of the nociceptive system through a series of complex and local actions that are not well-understood as of yet involving nociceptive receptors, nociceptive central feedback mechanisms, and the immune system [19]. The lack of scientific papers on the application of mesotherapy in treating chronic neck pain led us to make this investigation while bearing in mind the reduced adverse effects of local pain therapy, as opposed to a systemic drug therapy often used for treatment of CNP. More specifically, we wanted to determine whether mesotherapy is effective in treating CNP and to evaluate the effects of superficial trigger point injections with lidocaine versus dry ones.
2. Materials and Methods
2.1 Design of the study
A retrospective study was conducted on analysis from 01/01/2013 to 01/01/2014 of 84 medical records of outpatients treated for CNP with mesotherapy with medication or dry. All patients who underwent mesotherapy had signed an informed consent regarding the treatment protocol that respected the guidelines for experimental investigation in compliance with ethical principles of research per the Declaration of Helsinki. The research protocol was reviewed and approved by the local Department ethics committee.
2.2 Setting
Treatment was carried out at the Complex Unit of Physical Medicine and Rehabilitation, at Azienda Policlinico Umberto I Hospital, “Sapienza” University of Rome, Italy.
2.3 Type of participants
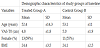
In this study we observed 84 patients with the diagnosis of CNP underwent mesotherapy treatment with medication or dry, 42 were eligible according to the inclusion criteria: age between 18 and 60 years old, a current pain intensity of ≤ 5 on a 10 cm visual analogic scale (VAS) [20], the presence of superficial trigger points for the trapezius muscle (superior, middle and inferiors fibers) and the splenius capitis muscles. Exclusion criteria are listed as follows: allergy to lidocaine, presence of acute neck pain, neck pain due to other causes such as vertebral fractures, spondylolisthesis, stenosis, herniated discs, presence of rheumatological, neurological or oncological concomitant diseases, presence of systemic infectious disease, presence of a severe systemic disease, previous cervical spine surgery, severe cognitive impairments and pregnancy, chronic or recurrent headaches. Patients did not receive any other medical intervention during the study and they were furthermore instructed not to take any new medications, NSAIDs or muscle relaxants drugs during the course of the study.
The sample selected of forty two (n=42) patients were divided into the Drug Mesotherapy Group (Group A: n=22) and the Dry Mesotherapy Control Group (Group B: n=20). At baseline all patients underwent complete evaluation by a physiatrist, who recorded detailed medical histories and reports of any allergic reactions to anesthetics, and performed a routine physical examination and a neurological investigation. Each patient was asked to provide a standard radiography (anterior-posterior and lateral X-rays) of his/ her cervical spine.
2.4 Interventions
Mesotherapy consists of a series of “microinjections” of a drug or active substance into the dermis, by means of short needles that are positioned at appropriate angles depending on the thickness of the skin.
The study group (A) received local microinjections of 1 cc of local anesthetic lidocaine hydrochloride 2% while the Control Group (B) received microinjections (performed with a needle) without any drugs (dry mesotherapy). The main investigator used a point by point microinjecting technique with specific needles (Luer needles, 30 G 0.4 mm × 4 mm) that were fully inserted and a 5 cc syringe held at 45° angle from the skin; only 0.10 ml of anesthetic was introduced at each selected site. We examined and treated 8 local superficial trigger points of the most important accessible muscles of the cervical tract that were identified by palpation following the guidelines provided by Travell and Simons trigger point manual [10,11]. More specifically, we treated 4 points on each side of the neck of the trapezius muscle (superior, middle and inferiors fibers) and the splenius capitis muscles. All subjects received 3 treatment sessions, 1 time per week for 3 weeks, and each session lasted about 10 minutes. The same doctor (a physiatrist) performed all treatments.
2.5 Outcome measures
Socio-demographic and anthropometric data were collected at the baseline. The primary outcome was the reduction of chronic pain. The following outcome measures were assessed at the baseline (T0), at the end of the treatment program (Tend) and at the three month (T3m) follow up.
Patients were evaluated with the Visual Analogue Scale (VAS). It is a simple, sensitive and reliable instrument that lets patients express their pain intensity as a numerical value. Patients were asked to mark on a 10-cm line the point corresponding to their perceived pain intensity, with 0 indicating the absence of pain and 10 the most severe pain [21,22].
The Neck Disability Index (NDI) is a clinical tool designed to assess perceived pain and disability in patients with neck pain. It consists of a total of 10 items, each having 6 possible choices. The NDI is a valid, reliable, and sensitive tool for measuring changes in pain and disability in patients with neck pain. The test can be interpreted as a raw score ranging from 0 to 50 (best and worst disability level) or as a percentage [23,24]. We expressed the score as a percent ranging from 0 % to 100 % (no disability and complete disability) [25].
The Verbal Rating Scale (VRS) is a five-category verbal rating scale with the eligible alternative answers “no pain” (0), “mild pain” (1), “moderate pain” (2), “severe pain” (3), “intense pain” (4). Pain was assessed by asking patients to indicate which of the five words gave the best description of their current pain. A score (e.g., from 0 to 4) that is assigned to each word is then used to measure pain levels [26].
The Short Form-12 Health Survey (SF-12) was administered to evaluate the quality of life with respect to CNP. The questionnaire consists of 12 items that explore eight subcategories that deal with physical activity (PF), the role and physical health (RP), the role and the emotional state (RE), mental health (MH), pain physical (BP), overall health (GH), the vitality (VT) and social activities (SF) and two indices that summarize the overall assessment of the subject with respect to his or her physical (ISF) and mental (ISM) health. Indices are derived from 8 evaluated subcategories and make it possible to summarize results. The questions relate to the day when the patient fills out the questionnaire and the four preceding weeks. The questionnaire is self-administered and its score ranges from 0 (worst health status) to 100 (best health status). The questionnaire has been translated in many languages including italian [27,28].
2.6 Statistical analysis
The data are expressed as mean and standard deviation and median. Because the clinical scores are ordinal numbers, nonparametric statistics were chosen for the between- and within group analyses. Between-group comparisons were analyzed by Mann-Whitney U-test for each assessment time, Bonferroni correction was applied. The alfalevel was set to 0.05. For the statistical analysis of the data collected was used utility software SPSS for Windows, version 18.
3. Results
Baseline scores (T0) did not differ significantly for any scale. Patient characteristics at baseline are listed in Table 1. The primary outcome measure was reduction in pain, assessed by VAS, the results of which are shown in table 2.Group A treatment significantly reduced pain for VAS at T1 (p=0,000), which rose after the end of treatment at T-follow-up and remained significantly lower than baseline levels (p=0,003). Short-term benefits were also observed in terms of the secondary outcome measures, but the medium-term effects were less significant. As shown in Table 2, a significant improvements in VRS and NDI scores were noted at the end of treatment in Group A respect Group B. The SF-12 scores are reported in table 3: group A patients had significantly different scores than their counterparts who received dry therapy at the end of treatment (p p=0,000 at T1, p=0,000 at T-follow up).


No side effects were recorded during the study.
4. Discussion
To our knowledge, this is the first study that evaluates the effectiveness of lidocaine using superficial trigger points mesotherapy for patients with chronic neck pain. The results showed that at the end of the therapy sessions (T1), inside the group A the average reduction in pain measured on the VAS scale was 2.26 points, compared to the control group in which the average reduction was only 0.79 points. The comparison between the values of the medians shows a variation even more significant reduction in pain between groups, 2.40 in treated patients, compared to 0.5 in the controls. Even disability measured by NDI is reduced more markedly in the A group compared to the control group, with a variation of the disability score which starts from 7.50 points for the controls and reaches 24,64 points for the treated patients. The same trend holds for changes measured by VRS. At 12 weeks after therapy the effect of improvement in pain and disability decreased slightly in both groups, while maintaining a statistically significant difference in favor of the group receiving treatment with lidocaine. Then, microinjections of 1 cc of local anesthetic lidocaine hydrochloride seems to have a good efficacy in CNP; on the other hand, also dry microinjections have a positive effect, not statistically significant, but clinically interesting.
The needle prick activates the cutaneous and subcutaneous receptors (reflex effect), and it is believed that endorphin levels actually increase after the introduction of the needle, but this hypothesis was not confirmed. Furthermore, interactions between the microvascular system and the immune cells in the dermis may play a role in the clinical benefits [17,29].
It could be hypothesized that lidocaine, administered using mesotherapy, produces a high drug concentration in the subcutaneous tissue and generates local effects in close proximity to inflammatory cells, sensory fibers, and vascular mediators that orchestrate inflammation and pain. It is thought that “microdoses” of active substances produce a mechanical distention of the surrounding tissues and sensitive fibres.
The maintenance of the result at follow-up (=after 3 months), certainly strengthens the patient compliance, and thus mesotherapy can be considered a good treatment for CNP, along with physical therapy.
The Physical and Mental Health Composite Scale scores (PCS and MCS) derived from the SF-12 have little intuitive meaning because the range of possible scores varies considerably. PCS and MCS scores tend to vary over the life span for different age groups as well (PCS tends to decrease with age, while MCS tends to increase).
Regarding of the indices of physical and mental health, measured by the SF-12 Physical and Mental Health Composite Scale scores, the confrontation analysis between the groups it shows different trends depending on the questionnaire. For SF-12 MCS residues of score between the timing of the end of therapy (T1)/12 weeks post therapy (T2) and the baseline (T0) were different between the groups in a statistically significant way, and instead, in the case of SF -12 PCS, the test that compares the median between the two groups does not produce significant results, the null hypothesis cannot be rejected. This fact indicates that in terms of mental well-being will notice a significant improvement in the treatment group (=A) compared to the control group (=B) in both timelines, instead of physical differences scores between groups may be random. The average gain of mental well-being was 10 points in the T1-T0 interval and respectively, 8.76 in the T2-T0 interval in the treated group; the score variation in the control group was 3.39 points in the T1-T0 interval and 1.96 points in the T2-T0 interval, statistically significant difference values.
On the other hand, this study has some limitations. We did not use a pressure algometry to identify a pressure pain threshold so we applied a clinical criteria according to Simons DG and Travell JG [10,11]. The sample size was small and we considered a short follow up evaluation, therefore further research is necessary to investigate the maintenance of results over a longer period. We were not able to compare our results to those of other authors, because of the lack of studies in related literature on mesotherapy treatment in CNP. Moreover, during the study, no patients reported adverse systemic effects, since mesotherapy treatment has a lower incidence of adverse events because of the lower systemic bioavailability of the drugs used. Moreover, no local reactions were found as a consequence of the treatment. Mesotherapy also provides benefits in terms of reduced costs and smaller number of treatment sessions required.
Surely, these findings suggest that further Randomized Control Trials (RTC) are required to assess the efficacy and tolerability of mesotherapy in a single treatment or in association with therapeutic neck exercises for CNP. While various attempts to reduce drug toxicity have been made, the use of local therapy (neural block, intraarticular, or periarticular injections of corticosteroids) has become popular among physicians, despite some controversies concerning its efficacy as a therapeutic remedy [30-32]. The superficial layer of the skin appears to have a sort of an innate “slow-release system”, and it is interesting to note that the terminology “local intradermal therapy” is used to highlight the fact that it modulates the absorption and diffusion of drugs at a local level [17,18].
5. Conclusion
In conclusion, results of the study indicate that administration of lidocaine using superficial trigger points with mesotherapy is an effective and well tolerated method for managing CNP in the short-term. Furthermore, injection of low doses of anesthetic with mesotherapy could be an alternative choice to conventional treatment approaches in this field.
Competing Interests
The authors have no competing interests with the work presented in this manuscript.
Author Contributions
Study concept and design: T. Paolucci, G. Piccinini Acquisition of data: G. Piccinini, F. Zangrando Analysis and interpretation of data: D.T. Pompiliu, Drafting of manuscript: T. Paolucci, G. Piccinini Critical revision of manuscript for important intellectual content: V.M. Saraceni, T. Paolucci, G. Piccinini Statistical analysis: D.T. Pompiliu Obtained funding: None Study supervision: V.M. Saraceni