


1. Introduction
Essential Newborn Care is the care given to the newborn infant following birth within the delivery room by skilled personnel. Birth is a major challenge to the newborn to negotiate successfully from intrauterine to extra uterine life. This transition from intrauterine to extra uterine life is dramatic one and demands considerable and effective physiological alterations by the baby in order to ensure survival. Immediate proper care of newborn is important for survival, growth and development of a newborn [1,2]. This immediate care time is crucial time to the babies for later wellbeing and adaptation. Skilled care during labor and childbirth with prompt management of complications alone can prevent about 50% of newborn mortality. Combined with adequate newborn care in the postnatal period, 75% of current newborn deaths can be prevented. It is a comprehensive strategy designed to improve the health of newborns [3-5].
The precise timing of clamping and cutting the umbilical cord is important to transfer from the placenta of about 80 ml of blood at 1 minute after birth, reaching about 100 ml at 3 minutes after birth. Clean cord care which is very important in preventing early neonatal infections. These more volumes of blood can supply extra iron amounting to 40-50 mg/kg of body weight [6,7].
Newborns are most vulnerable during the first hours and days of life, yet this critical window of opportunity is being missed [3]. Globally 2.5 million children died in the first month of life at an average rate of 18 deaths per 1,000 live births in 2017. There are approximately 7000 newborn deaths every day, amounting to 47% of all child deaths under the age of 5-years, up from 40% in 1990. The world has made substantial progress in child survival since 1990. Globally, the number of neonatal deaths declined from 5 million in 1990 to 2.5 million in 2017. However, the decline in neonatal mortality from 1990 to 2017 has been slower than that of post-neonatal under-5 mortality: 51% compared with 62% globally [2].
Despite promotion of ENC as one strategy for improving newborn health outcomes, the standardized procedure for providing ENC is not fully practiced [8]. A study conducted in eastern Uganda on using the three delays model to understand why newborn babies die showed that neonatal mortality autopsies indicated that the low levels of knowledge among health workers regarding newborn care as a major determinant of neonatal death [10]. Evidence shows that initiating breastfeeding within one hour of birth reduces the neonatal mortality by 44%, recent data show that worldwide less than half of newborn babies receive the benefits of breastfeeding per standard [3].
In Africa a cross-sectional observational assessment of quality of newborn care in health facilities across six sub-Saharan African countries shows that those immediate dried baby with towel were 79%, cut cord with clean blade were 94%, initiated breastfeeding with in the first one hour were 43%, and ties/clamp cord when pulsation stop or 2-3min after birth were 65% [13]. Study conducted in Sudan Khartoum on immediate care of the newborn showed poor practices on immediate care of the newborn [14]. Study conducted on essential newborn care in Bamako, Mali showed that the dosage of vitamin K was poorly known by the staff that was 18.9% and 17.2% among midwives nurses respectively [15].
In Ethiopia, a cross-sectional national facility based observational surveys conducted on maternal and newborn care practices at hospitals shows that immediate essential newborn care is only 18% [9,15,16,24]. A study conducted in Jimma zone on knowledge and practice of essential newborn care among nurses and midwives showed that (48.9%) of respondents had poor practice on essential newborn care [9]. The Study conducted in India on assessment of Essential Newborn Care Services in secondary-level facilities pointed out the overall average skill score was 34%. However, the average practice score for doctors were 31% and for nursing staff was 35% [27].
A study conducted in Tigray Eastern zone on knowledge and practice of immediate newborn care among midwives showed that (47.6%) of respondents had poor practice on essential newborn care [26]. A study conducted in Bahir Dar city on knowledge and practice of immediate newborn care among health professionals showed that 40.3% of respondents had poor practice on essential newborn care [8]. Taking this situation into account, the Ethiopian government collaborating with its partners has launched various initiatives for improving knowledge and skill of health care providers through training health care provider on ENC, equipping health facility with staffs and equipment for provision of essential newborn care [2,3].
Despite this implementation of neonatal mortality rate reduction activities, neonatal death remained stable at 37 deaths per 1,000 live births in the 2011, and 29 deaths per 1,000 live births in 2016 EDHS survey. Over the past 16 years, neonatal mortality declined only by 20% [17,18]. According to goal set in number 3 of sustainable development, United Nation globally aims to end the preventable deaths of newborns from 22 deaths per 1000 live births to 12 deaths per 1000 live births by 2030 [4-7,10]. The current Ethiopian situation of Newborn mortality is far away from UN targets.
Despite all these efforts, neonates face problems after delivery in many public health facilities of Wolaita Zone. So, this study aims to assess the practice gaps of health care provides on essential newborn care and to recommend solutions on the identified gaps to the program managers, policy makers and program implementors. Because similar study was not conducted in my study area before, so this study was carried out to identify gaps on practice of essential newborn care.
2. Objectives of the Study
- To determine magnitude of essential newborn care practice among Nurses and midwives working in MCH case team at public health facilities of Wolayta Zone, 2019.
- To identify factors associated with essential newborn care practice among Nurses and Midwives working in MCH case team at public health facilities of Wolayta Zone, 2019.
3. Methods and Materials
3.1 Study setting and period
The study was conducted in public health facilities in Wolayta zone from March to April, 2019. Wolayta zone is one of the 14 zones in Southern Nations Nationalities and Peoples Region (SNNPR), Ethiopia. In the zone, there are currently 5 governmental hospitals and 2 nongovernmental hospitals, 68 health centers post and 342 health. Totally, there are 406 midwives and nurses who are working in MCH case team at public health facilities of Wolayta Zone.
3.2 Study design
Health facility based cross-sectional study with quantitative and non-participatory observational method of was used.
3.3 Population
3.3.1 Source population
All nurses and midwives who were working in MCH case team at public health facilities of Wolayta Zone during data collection period were source population.
3.3.2 Study population
All nurses and midwives who were working in delivery and postnatal care unit in selected public health facilities of Wolayta Zone during data collection period were considered as study population.
3.4 Inclusion and exclusion criteria
All midwives and nurses who work in labor and delivery unit in selected public health facilities at the time of data collection were included. Student nurses and midwives and those who were in annual live were excluded from study.
3.5 Sample size determination
Sample size was calculated for first and second objectives taking the following assumptions: P= magnitude of practice is 51.1% from study conducted on essential newborn care in Jimma zone [9]; Zα/2= critical value at 95% confidence level of certainty (1.96); d= the margin of error or accepted error between the sample and the population= 5%; and sample size calculation was made taking out come in unexposed and adjusted odds ratio to each factor used from different studies, the sample size was calculated by using Epi info version 7.2.1.0 and taking confidence interval of 95%, power= 80%, ratio of exposed to non-exposed as 1:1; and final maximum sample size after adjustment and adding 10% non-response rate was 218.
3.6 Sampling procedure
The study was carried out in randomly selected public health facilities of Wolayta Zone. A 31 health centers were selected by using simple random sampling technique and all public hospitals were included in the study. Finally all nurses and midwives who are working in labor and delivery unit in selected public health facilities were enrolled in the study.
3.7 Study variables
3.7.1 Dependent variable
- Practice of essential newborn care.
3.7.2 Independent variables
- Socio-economic factors: sex, age, income level, marital status.
- Personal factors: educational status, years of experience, training, knowledge, type of profession, interest to work in delivery unit.
- Institutional factors: availability of equipment, presence of guidelines, facility type.
3.8 Operational definition and definition of terms
Essential Newborn Care: is care provided to a newborn immediately after delivery which includes the time between births to 24 hours care and it includes dry and stimulate, evaluate breathing, keep the newborn warm (Prevent hypothermia), initiate breastfeeding in the first one hour, administer eye ointment, administer vitamin k intramuscularly, weigh the newborn when it is stable and warm, cord care and delay bathing of the baby for 24 hours after birth.
Good knowledge: when the health care provider answers equal to mean or above from 22 knowledge questions.
Poor knowledge: if the health care provider answers below the mean in 22knowledge questions.
Good practice: if the health care providers perform more than or equal to 70% the practice procedures in observation.
Poor practice: if the health care providers performs less than 70% of the practice procedures in observation.
3.9 Data collection tools and methods
3.9.1 Data collection instruments
Data were collected using interview administered questionnaire and observation check list to get quantitative data. Interview-administered structured and pre-tested questionnaire was used to get data on variables of respondents and observation check list was used to assess practice of immediate newborn care. Questionnaire and observation checklists were adapted from different literatures and modified by using different WHO guide lines was used to collect data from nurses and midwives on different variables.
3.9.2 Data collectors and data collection procedures
The data was collected by ten diploma midwives/nurses and five supervisors who have a bachelor degree in Midwifery/nursing with experience were involved in data collection. Training was given for data collectors and supervisor before the pretest on the objective of the study the contents of the questionnaire, observation checklist, and issue related to the confidentiality of the response and the right of the respondents. The non-participatory observation was applied while a nurse or midwife attend delivery and provide essential newborn care. After observation, other variables were asked from nurse or midwife through interview in private room.
3.9.3 Data quality control
Data quality was controlled through training of data collectors on objectives, questionnaire, and ways of conducting interview and observation. Pretest was conducted in 5% of sample size in Sodo Christian hospital and Dubo hospital and the necessary arrangements and corrections were made to standardize and ensure its validity. All filled questionnaires were checked for completeness, accuracy, and consistency. Supervision was done by the supervisors and principal investigator throughout the data collection period.
3.9.4 Data processing and analysis
First data were coded, completeness and consistencies of questionnaires were checked and data entry was made using Epi data 3.02. Then the data were exported to the SPSS statistical package version 22 for further analysis. Before analysis, data were further cleaned for possible errors. Data were presented in frequency, proportions and summary statistics to describe the study variables and factors under study.
Bivariate analysis was carried out to identify variables that are significantly associated with knowledge of immediate new born care. Variables whose p value ≤ 0.25 in bivariate analysis were included in multivariate analysis. Then, multivariate analysis was done to identify independent factors by controlling for possible confounders. AOR at 95% CI with p-value ≤ 0.05 were estimated to measure strength of association and variables were interpreted as having statistically significant association when p ≤ 0.05 in logistic regression.
3.10 Ethical consideration
Ethical approval letter was taken from research review committee of Arba Minch University College of Medicine and Health Sciences. An official letter from the university was submitted to Wolayta zone health department. Then letters were written from Wolayta Zone health department to respective Woreda health office and hospital. Data was collected after informed written consent was taken from each participating nurse and midwives on whom observation will be made.
4. Result
4.1 Socio-demographic characteristics
In this study, 216 nurses and midwifes were participated making a response rate of 99.1%. Among these, 174 (80.6%) were females. The median age of respondents was 26. Regarding profession, 163 (75.5%) were midwifes and 53 (24.5%) were nurses. Regarding their educational qualification, 152 (70.4%) were with diploma level of education and 64 (29.6%) were with Bachelor degree level of education as shown in Table 1.

4.2 Facility and individual characteristics
Regarding work experience of study participants, 161 (74.5%) had less than five years work experience and participants who had greater than six years of work experience in labor and delivery unit were 55 (25.5%). Among the study participants, 43 (19.9%) responded that they had no interest to work in delivery room. 148 (68.5%), 133 (61.6%) and 128 (59.3%) of participants responded presence of guide lines on immediate new born care, equipment for newborn care and vaccines and drugs for newborn care at their health institution respectively. Regarding training, 147(68.1%) of participants got training on ENC as described in Table 2.

4.3 Knowledge on thermal protection, airway clearance and neonatal resuscitation
Regarding hypothermia protection newborn placement immediately after birth, 65.7% responded that that newborn should kept on the mother’s chest/ belly immediately after birth, the rest 34.3% did not know the recommended place where newborn should be placed immediately after birth. Among respondents, 68(31.4%) did not respond the recommended time of bathing newborn. Concerning measures to be taken if baby not crying immediately after delivery, 153(70.8%) of them responded that the correct measure is calling a help and start resuscitation.
Regarding the position of the baby’s head to open the airway, 137(63.4%) of respondents responded that the baby’s head should be slightly extended and 59(27.3%) were responded as flexed position of the head and 20(9.3%) of them responded as hyper extended position of the head.
4.3 Knowledge of breast feeding
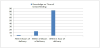
Regarding breast feeding, majority of study participants were aware that initiation of breast feeding after delivery should be taken within the first hours of delivery. When the participants asked about the duration of exclusive breast feeding, 172 (79.6%) of the respondents knew that the mother should feed breast her baby exclusively for the first six months, but 44 (21.4%) of the respondents did not know for how long the mother should exclusively breast feed her baby; 3 (1.4%) responded as less than six month and 41 (19%) responded as for greater than six month shown Figure 1.
4.4 Knowledge of prevention of infection on cord care, eye care and care of low birth weight
From the respondents half of study participants 109 (50.5%) were aware that the cord of crying baby should be clamped or tied at 2-3 minutes of delivery or after the pulsation of umbilical artery stopped, but 45 (20.8%), 62 (28.7%) of them responded as that the cord should be clamped or tied immediately after delivery and within 1-2 minutes of delivery respectively. Out of the total respondents, the vast majority, 182 (84.2%) know to use sterile scissor to cut the cord, but only 14 (6.5%) were aware that new surgical blade can also be used to cut the cord whereas few respondents; 20 (9.3%) mentioned clean scissor. The vast majority, 196 (90.7%) were aware that silver nitrate/tetracycline can be applied for the treatment of eye infection for newborn but, only 13(6%) were aware that sterile water can also be used to clean infected eyes.
4.5 Knowledge of nurses and midwives on birth weight of newborn child
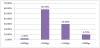
About the recommended cares of low birth weight babies, 99 (45.8%), 137 (63.4%), 27 (12.5%) and 8 (3.7%) of participants identified as breast feeding early and frequently, keeping the child warm, infection prevention and bathing often respectively. Participants who have knowledge on prevention of newborn bleeding were 200 (92.6%) and 109 (50.5%) have knowledge about the correct dose of Vitamin K to be given to a term newborn shown in Figure 2.
4.6 Provider’s knowledge on immediate newborn care
The overall knowledge of nurse and midwife on immediate newborn care in public health facilities of Wolayta zone is 125 (57.9%) the average knowledge score is 58% and standard deviation was 0.495.
4.7 Essential Newborn care practice among nurses and midwives
Observations were made on nurses and midwifes while they giving immediate newborn care. Among the total 216 respondents, 44.4% (95% CI: 38%, 51%) participants have good immediate newborn care practice as shown in Figure 3.

Specifically 192 (88.9%) of the participants have properly practice putting a baby on to mother’s abdomen immediately after delivery, 185 (85.6%) of the participants place the baby in skin-to-skin contact and on the breast to initiate breastfeeding, 160 (74.1%) of participants apply tetracycline eye ointment and 70 (32.4%) give Vitamin K IM on anterior mid-thigh. From health worker place identification labels on newborn were 45 (20.8%). Health workers weigh the baby immediately after birth was 205 (94.9%) and initiation of breast feeding within one hour was 196 (90.7%) shown in Table 3.

4.8 Bivariate and multivariate analysis result on practice of immediate ENC
In bivariate analysis, monthly income, type of profession, educational status, experience in delivery unit, type of facility, interest to work in delivery unit, got in service training, availability of BEmONC guidelines, availability of equipment, availability of drug and vaccines and knowledge on ENC were variables with p-vale less than 0.25; hence candidate for multivariate analysis.
Among variables entered in multivariable analysis; knowledge on immediate newborn care (AOR= 3.53, 95% CI: 1.75, 7.09), type of facility (AOR=0.23, 95% CI: 0.097, 0.55), availability of equipment in health facility for ENC (AOR=3.44, 95% CI: 1.64, 7.21), getting onjob training (AOR= 2.768, 95% CI: 1.25, 6.13) and work experience in delivery unit (AOR= 2.58, 95% CI: 1.198, 5.566) were variables significantly affecting participants’ practice on essential newborn care shown in Table 4.

5. Discussion
This study was planned to assess magnitude of immediate newborn care practice and to identify associated factors among nurse and midwife in public health facilities of Wolayta zone. Accordingly, magnitude of good practices on immediate care of newborn was 44.4% (95% CI: 38%, 51%).
This finding goes in line with the study conducted in Khartoum [14] and Jimma zone (51.1%) [9]. However, this finding is lower compared to study conducted in Tigray eastern zone (72.8 %) [26] and Bahir Dar city (59.7%) [8]. The difference might be due to variation in set up which is well equipped and areas where there are many nonprofit organizations working with regions, zones and health facilities. Those different organizations provide training and support health facilities with basic facilities.
Regarding factors affecting practice on immediate new born care, knowledge on ENC, training, type of facility, availability of equipment and work experience in delivery unit were identified to be significantly associated with practice on immediate new born care. Knowledge based practice essential to minimize errors while giving care to newborn. Nurses and midwives with good knowledge are nearly four times more likely to give proper newborn care when compared with those with poor knowledge. This finding was supported by study conducted on knowledge and practice on essential newborn care in Jimma Zone, Ethiopia [29], in Bahir Dar [8], and in Tigray Regional state [23]. This might be due to type of professionals in the health care setting and proof of knowledge is basic to practice.
Availability of equipment in health facility for ENC was significantly associated with participants’ practice on essential newborn care. Those health nurses and midwives working in facilities with adequate equipment for ENC were practicing ENC in proper way compared to those working in health facilities having shortage of equipment for newborn care. This study finding is similar with study conducted in Tigray eastern zone [26]. This finding is contrary to the finding from Jimma zone which report that availability of equipment in health facility is statistically insignificant on practice of ENC [29]. The difference might be due to difference in commitment of health system managers across regions and number of nonprofit organizations that provide equipment to health facilities.
The type of facility was significantly associated with participant’s practice on essential newborn care. Those participants working in health center were less likely practicing of essential newborn care compared to those participants working in the hospitals. This finding is similar with study conducted in central zone of Tigray region [23] and Tigray eastern zone [26]. This finding is different from the study conducted in Uganda, which shows the type of health facility has no significant association with newborn care practice [25]. This difference may be due to difference in study setting and may be difference in availability of required equipment for essential newborn care.
Training found to be significantly associated with participants’ practice on essential newborn care. Participants who had got training on essential newborn care were more likely practiced essential newborn care practice than those who did not trained on essential newborn care. This finding is similar with study conducted in Jimma zone [9,29]. This similarity may be due to similarity in study population. Finding from this study shows work experience in delivery unit was significantly associated with practice of essential newborn care. Participants who had served six years or longer were more likely practiced essential newborn care than participants who had served five years or less. However this finding is contrary to the study conducted in Tigrie eastern zone which report that no statistical difference in practice of essential newborn care among different work experience groups [26]. This difference may be due to difference in work experience groups among study populations and may be due to difference in study period.
6. Conclusion and Recommendation
Practice gap exists among midwives and nurses on care given to immediately born baby in the study area. Especially, cord clamping time, consistently administration of Vitamin K, placing identification and using clean mask during attending delivery take lion share of practice gap among midwives and nurses in the study. The managing bodies of health facilities should strive to improve practice of essential new born care through creating training opportunities for staffs working in delivery room.
In addition, the institutions should create strong structure to follow poor practice providing strong supportive supervision system and constructive feedback mechanism. All other concerned bodies that work on MCH should take part by appraising good performers in taking care of essential new born care through supporting necessary supplies. Further research in the area should consider qualitative method and should involve the whole region.
Competing Interests
The authors declare that they have no competing interests.
Author Contributions
The idea of the study was conceived, designed, write up and initial draft of manuscript was done by Zerihun Z and Aseb A; whereas Addisu A. and Zeleke A. worked together on methodology, field supervision, and analysis and manuscript review process.
Acknowledgments
We are very grateful to Arba Minch University College of Medicine and Health Sciences for giving chance and supporting throughout this research project. Our sincere and deepest gratitude goes to administrators of public health facilities for their crucial assistance and facilitation. We would also like to extend our heartfelt appreciation to the study participants for their cooperation.