


1. Introduction
Hip subluxations often occur in children with CP, especially in children who are unable to walk. Population-based studies have shown that the rate of hip subluxation increases significantly, depending on the child's reduced functional level, from 0-5% in level I of the Gross Motor Function Classification System (GMFCS) [1] to 70-90% in level V [2-5]. The greatest risk of hip subluxation is between the ages of 4 and 12 years [6]. If the hip remains untreated, the hip lateralization progresses at an average RMI + 7% per year depending on age and walking ability [7]. When a complete displacement occurs, hip pain and profound problems with the walking ability, sitting balance, and genital care may occur [8,9]. Therefore, screening programs for the early detection and treatment of hip subluxations were developed [2,10,11].
Soft tissue procedures such as adductor and psoas releases have been recommended as prophylaxis to prevent hip displacement. Although such procedures had a good effect in studies with a mean follow-up time of 3-4 years in 70-80% of the hips [12-14], the rate in other studies with a longer follow-up period was smaller and the recurrence rate above 50% [15,16]. It has not been clarified when and why the operation fails. It is therefore unclear whether fails are caused by a poor primary correction of subluxation or by a later relapse after a satisfactory primary correction. Further research needs to be done.
After the soft tissue procedures, the patient usually was immobilized in abduction splints for at least 6 weeks.The physiotherapy started afterward. It wasn't analyzed whether this immobilization also had a bad impact on the results.
In the Terjesen [5] study, surgical treatment was recommended for children with a migration index (MP) of over 33%. According to the guidelines of the Norwegian working group, soft tissue releases should be used for mild and moderate subluxation, while bony procedures should also be carried out for children with severe subluxation (MP ≥50%).
In the Hägglung [3] study, the risk of subluxation (MP >40%) was directly related to the degree of gross motor function, classified according to the GMFCS, reaching from 0% for children in GMFCS level I to 64% in GMFCS level V. Since lack of movement will probably have a negative influence on muscle mass and elasticity, as emphasized by Silvferskjöld [17], postoperative immobilization and fixation, as little invasive and less painful surgical procedures as possible and early functional rehabilitation treatment were sought. Percutaneous myofasciotomy was chosen as an alternative to the open soft tissue release, and percutaneous femoral neck screw epiphysiodesis according to Lee [18] was chosen as an alternative to derotation-varus-osteotomy of the proximal femur in children over the age of 6.
The rehabilitation program included the movement of all muscles and joints up to the pain limit from the first postoperative day, full load bearing when standing, starting with assisted movements and increasing, as far as possible, to independent movements, lymphatic drainage from the first day against lymphatic congestion and hematomas.
The rehabilitation program included the movement of all muscles and joints up to the pain limit from the first postoperative day, full load bearing when standing, starting with assisted movements and increasing, as far as possible, to independent movements, lymphatic drainage from the first day against lymphatic congestion and hematomas.
We hypothesized that this therapy regime can achieve at least the same result as open muscle and tendon release described in earlier studies.
2. Patients and Methods
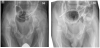
The study program was started in our hospital in 2010. All children with CP who were presented in the hospital or in our external outpatient clinic were indicated for soft tissue release because of severe muscle contractures and showed a RMI above 25% on the X-ray were included (Figure 1). The current investigation includes the results for patients up to operations in early 2016, allowing a follow-up period of at least 4 years. The diagnosis and type of CP were made according to the SCPE 2000 guidelines. The study program includes systematic clinical and radiological follow-up examinations. The movement deflection was measured clinically and classified according to GMFCS and radiologically the Reimer migration index (RMI), the acetabular angle (AC) and the projected femoral neck shaft angle (NSA) were measured.

The present study included 52 children with 99 critical hips who had undergone percutaneous soft tissue release. The mean age at surgery was 4.8 (2.8-6.7) years. 43 children had bilateral CP (14 of them diplegic) and 4 children dyskinetic CP (variable muscle tone) (Figure 2).

The percutaneous myofasciotomy took place depending on the clinical examination findings. To influence the development of the hip, muscles that have a direct influence on the movement of the hip joint were myofasciotomised. These were the adductor longus, the gracilis, the tensor fasciae latae, the gluteus, the rectus femoris, the semitendinosus, the semimembranosus and the quadriceps. As part of the operation, muscles not directly influencing the movement of the hip joints, which can have an indirect influence on muscle tone via the muscle chainswere also treated.
The adductor longus muscle was treated if the abduction was below 60° with the hip and knee flexed, the gracilis if the abduction was not possible with the hip and knee extended up to at least 40°. In the absence of hip extension to 0° with the Thomas grip on the opposite side, the tensor fasciae latae and, if that alone was insufficient, the rectus femoris were released. In case of spontaneous external rotation less than 20° in hip extension the gluteus medius was addressed. The popliteal angle should not be greater than 30°, otherwise, the semitendinosus and the semimembranosus were myofasciotomised and inoverhang the knee flexion with the hip in extension should be at least 70°. Otherwise, myofasciotomy of the quadriceps muscle was performed. All ranges of movement were checked only with slight pressure.
The rehabilitation was carried out early on with functional movement and full load, lymphatic drainage and hematoma treatment as well as splints in extension and abduction during rest.
As of April 2016, we conducted a prospective study with surgical treatment with myofasciotomy and in combination with femoral neck epiphysiodesis in children over the age of 6 if they were presented in the hospital or in our external outpatient clinic, were indicated for soft tissue release because of severe muscle contractures showing an MP of over 25% on the X-ray of the pelvis. So far, 16 hips of 12 children over the age of 6 have been included. The mean age at the operation was 7.9 (6.1-12.7) years. All children had a bilateral CP (5 of them diplegic). In total, we have now performed this treatment in over 160 hips. The range of movement was clinically measured and classified according to GMFCS and radiologically the RMI, the AC and the projected NSA were measured (Figure 3a and 3b).
The muscles were treated in the same way as in children up to the age of 6 years. In addition, a self-drilling and self-tapping banjo screw was inserted percutaneously in the children approximately 3 to 5 cm below the greater trochanter apophysis in the axis of the femoral neck through the femoral epiphyseal plate under fluoroscopic control. The placement in the cortex of the shaft was done using a Kirschner wire. The placement in the femoral neck, however, was done directly without placing the Kirschner wire (Figure 4a, 4b and 4c).

In this group, too, the rehabilitation was carried out early in terms of function, with immediately permitted movement and full load, lymphatic drainage and hematoma treatment, as well as splints in the extension and abduction during rest. Special protection was not required.
The Ethics Committee of the Schön Clinic Munich Harlaching approved ethical permission. No additional examinations or therapies were performed in comparison to our regular surveillance. Our treatment regime in children older than 6 years with hips at risk had guided growth treatment instead of varisation osteotomy.
3. Results
In the group of children under 6 years with myofasciotomy, we found improvement in RMI of 33%, deterioration of 5% and stabilization of 62%. We divided into 3 groups with initial RMI 25-39%, RMI 40- 49% and RMI >50%. The RMI improved from an average of 31% to 30% in the group with moderate subluxation, from 43% to 36% in the group with strong subluxation and from 69% to 62% in the group with extreme subluxation.
The AC improved in the group with moderate subluxation from an average of 23° to 19°, in the group with strong subluxation from 28° to 24° and in the group with extreme subluxation from 40° to 29°.
In the follow-up examination depending on the GMFCS, the AC improved in patients in level 3 from 26° to 22°, in level 4 from 26° to 21° and in level 5 from 40° to 26°. Depending on age, the RMI improved by an average of -4.5% per year for 2 to 3-year-old children, by -5.7% for 3 to 4-year-olds and by -3.7% for 4 to 5-year-olds, for the 5-6-year-olds by -2.2% and for the 6-7-year-olds by -5.6% (Figure 5a and 5b).

We found no differences in the development of RMI according to the different GMFCS levels. The children with level 2 showed an average improvement of -6.0% (+ 0.6% to -11%), the group level 3 of - 4.4% (+2.4% to -13.3%), at level 4 of -5.0% (+13% to -57.6%) and finally level 5 of -2.9% per year from the baseline. Over the entire examination period, the hips improved by 10% or more in 33 hips (33%), the RMI did not change for 61 hips (deviation from the baseline values less than 10% and the RMI deteriorated by 10% in 5 hips) and more.
For our patients older than 6 years who were treated with myofasciotomy and femoral neck epiphysiodesis, we found a mean improvement in RMI of 5% for 16 hips and a 9° NSA improvement at 16 months follow up. More precise and somewhat longer-term results are currently being evaluated and will be published in a next article.
4. Discussion
Hip instability is one of the most common orthopedic problems in CP and can lead to subluxation or displacement before skeletal maturity begins. Therefore, orthopedic management should be carried out according to the age of the patient and the severity of the pathology as well as the functional and mobilizing capacity. Most clinicians prefer surgical treatment as subluxation progresses. Unlike in other published studies, we prefer early percutaneous release of the muscle fascia instead of open tendon releases in children with CP under the age of 6 and additional early guided growth when the femoral neck is steep rather than a varus osteotomy in children over the age of 6. Both treatments allow an immediate full load and movement exercises up to the pain limit. An immobilization as with tendon releases and varus osteotomies is not necessary. The disadvantages of immobilization, pain-related passivity and relief with muscle atrophy and fibrosis of soft tissues are, therefore, less expected. These minimally invasive, gentler interventions also can stop the subluxation for most and even converted into a slight improvement for some cases. According to Terjesen [7] a untreated hip at risk develops a worsening of + 7% RMI per year. According to our results, the positive effect of percutaneous soft tissue release is independent of the existing MP, the GMFCS and the age in the examined age range from 2 to 6.
The current study shows an increased MP in GMFCS IV and V at the time of surgery. All patients with very high MP were from groups GMFCS IV and V. These results are similar to those of other studies.
The classification of our patient group according to GMFCS showed that there were 3 patients in stage II, 9 patients in stage III, 19 patients in stage IV and 21 patients in group V. After the operation, there were 2 Level I patients, 4 Level II patients, 10 Level III patients, 19 Level IV patients and 15 Level V patients. Mutlu et al., [19] found a slight change in measurements in the GMFCS- level in 30 patients with CP through surgical treatment. The preoperative classification of the patient group according to GMFCS showed that there was 1 patient in level I, 4 patients in level II, 5 patients in level III, 9 patients in level IV and 11 patients in level V. After the operation, there were 4 level I patients, 2 level II patients, 5 level III patients, 10 level IV patients and 9 level V patients. Barakat et al. [20] used the GMFCS to evaluate the functional results of 22 patients with CP with whole-body involvement in which soft tissue release and bony surgery were performed due to hip subluxation or dislocation. Before the operation, 5 patients were level III, 7 level IV, 10 level V, while after the operation 9 were level III, 6 level IV and 7 level 5 (20). In the study of Root et al. [21], at the end of a mean follow-up period of 7 years, coverage of the femoral head, a painless hip and an improvement in walking ability by at least one level was achieved. In our study, the GMFCS level remained constant for 37 patients and improved for 15. There was no decrease in GMFCS in any of the patients.
Terjesen [22] recommended a bilateral soft tissue release in ambulant and non-ambulant children with CP and existing hip subluxation. He recommended an early soft tissue release before 50% MP occurred.
Minimally invasive release of muscle fascia appears to be as effective as open release, as it is done with hip screening programs in many countries. The recovery of children who receive minimally invasive treatment is faster. Less surgical soft tissue damage, faster mobilization and fewer restrictions than with a varus osteotomy make guided growth a treatment option for coxa valga in the spastic hip dislocation in non-ambulant children with cerebral palsy.
5. Conclusion
Our initial clinical findings and the data obtained from the study led us to significantly reduce open procedures and to perform minimally invasive procedures as often as medically justifiable. Further studies have to prove the effectiveness of this methods in the long term.
Competing Interests
The author declare that there is no competing interests regarding the publication of this article.