


1. Introduction
Patient safety is a significant factor to high quality patient care. Medical errors have to a large extent undermined this safety and therefore the quality of patient care. Medical error defined as the incorrect action or plan that may or may not result in patient harm [1]. These errors are an occurrence within the healthcare system as a consequence of its fragmented and decentralized nature [2,3]. Medical errors can be trivial or serious and life threatening and may result in patients making fully recovery, partial recovery, or death [4]. The prevalence of medical errors around the world is high, parallel investigations that have been conducted in the nations of the United Kingdom, Australia, Italy, Switzerland, and Denmark have shown that human errors in healthcare is a serious global public health concern [5]. Other studies note that medical errors are a significant clinical issue and result in high rates of morbidity and mortality in healthcare setting around the world [6,7]. This is further illustrated that deaths associated with medical error in the US have been estimated to exceed the yearly number of deaths due to motor vehicle accidents, HIV/AIDS, or breast cancer. Further, the cost of medical errors is quite high and estimated amount of $17 billion. This cost is incurred in form of disability, direct health care, and income [8]. From the above, the impact of medical errors is quite detrimental thus serving as a significant force that has propelled increased focus on this issue and particularly its reduction and improvement of the healthcare system. One key way towards improving safety of patients and fostering quality of the healthcare system is to ensure that there is an awareness of these errors. Disclosure of medical errors is a significant step towards this issue so disclosure of an adverse event serves as an essential element towards management of the consequences of error [9]. Szostak et al., postulates that patients have a need to learn about all medical errors despite their severity, further, patients equally are concerned about the key preventive measures that hospitals have made in order to prevent such errors from taking place in the future [10]. This is further demonstrated by Al-Nomay, et al who affirms that patients are keen to known about medical errors that may have adverse effects on them [11]. Despite this, there is a considerable amount of absence of disclosure of medical error [12]. The Kingdom of Saudi Arabia also reports quite a number of cases of medical error among physicians and found that patient safety and medical errors has emerged as a critical national problem [13]. However, there is limited research on this issue even more so as a consequence of less disclosure of these errors among healthcare providers [14,15]. Nonetheless, there are a number of researchers that have delved into this area of field and provided insight into medical errors in KSA and subsequent impact on patients and the healthcare system.
Research in medical errors by physicians within the KSA context is underlined with the issue of inadequate cases and process of disclosure of these errors, and physicias continue to undermine the significance of medical error disclosure. The problem that emerges in regard to disclosure of medical errors to patients and their families is harmful errors are seldom disclosed [16,17]. Szostak et al. explains that healthcare providers do not always reveal medical errors out of fear of litigation and damage to their reputations or that of their hospitals [10]. Majority of hospitals sometimes disclose medical errors but it is only one third that have policies in place to tackle this problem [18,19]. However, in the event that these errors are disclosed they usually do not meet the expectation of patients nor their families. Therefore, this inadequacy in relation to disclosure of medical errors poses a much serious hazard for patient safety [20,21]. The aim of this research is to investigate the key causes of medical errors among physicians, identify the main challenges of disclosure to patients and their families, and provide context for development of effective techniques and procedure for disclosure of these errors in Saudi Arabia. This is accomplished by undertaking the following key objectives. Firstly, the research will assess existing literature on medical errors including their disclosure to patients and their families. Secondly, this research will also explore the key reasons contributing to the limited cases of disclosure of medical errors by physicians.
2. Objectives
To identify the main cause and nature of medical errors, detect main issues and challenges hindering the disclosure of these errors by physicians, and developing a background for developing constructive strategies of disclosure of these errors.
3. Methods
3.1 Design of research
This study is cross sectional descriptive which entailed the collection and analysis of data on medical errors by physicians and their disclosure at a specific point in time from February till September 2018.The data collection process was carried out using self-administered online questionnaires to physicians and hard copy questioner to patient/family. The physician questionnaire contained a total of 15 questions. Some of the questions were developed to capture the characteristics of the physicians in terms of demographic information, professional roles, the characteristics of the participants including key information regarding their title, gender, nationality, specialty, institute, experience post residency certificate, and post graduate outside KSA training experience.
Followed by first question in regards disclosing different medical errors ranging from minor to fatal errors, disclosing harmful errors in hopeless ill patients, and disclosing other doctors errors. Second question about how and when to disclose the error, third question barriers to error disclosure. Followed by the physician would evaluate ways of disclosing medical errors by physicians using two scenarios. The first scenario entails the treatment of a patient with severe asthma with continuous Salbutamol Nebulization. By mistake the physician makes an order of 10 times the dose resulting in the patient arrest for 3 minutes due to Hypokalemia. The patient is resuscitated and is expected to make a full recovery. The second scenario involved a patient that was admitted with left pleural effusion by mistake chest tube placed at the opposite side confirmed by x-ray. Both scenarios followed by several questions first what would you most likely say about what happened? Second question how would you most likely say regarding an apology? Third question how would you discloses this error? (Supplementary File). On the other hand, the patient family questionnaire was made up of six questions that included demographic information including level of education and response to medical error disclosure by physicians, whether filing complaint to the administration of the hospital, complaining to judicial office, politely asking what led to complication, demanding for an explanation by raising a voice or taking the issue to the media (Supplementary File).
3.2 Procedure
The procedure of conducting this research study entailed undertaking the following steps. In the first place, the study began by a through brainstorming of the research topic accompanied by a brief look up of literature on it. The significance was to capture the research gap that the topic had. The next step was development of a research proposal that provided an overview of how the study will be pursued. In addition, this also entailed obtaining ethical authorization from the institutional review board (IRB) to carry out the study. The next key steps that followed were development of a comprehensive literature review, search and recruitment of participants, data collection, analysis and interpretation of the data, and developing the final copy of the study. Another step that equally significant for this study was in relation to providing informed consent to the participants a critical aspect of research involving human subjects. In addition, the participants were ensured of confidentiality and protection of their identities and information through use of pseudonyms and careful storage of their data.
3.3 Statistical analysis
All Categorical variables gender and level were presented as numbers and percentages. All data was entered and analyzed through statistical package SPSS version 22. The study is approved by KFMC IRB Committee.
4. Results
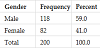
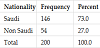
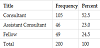
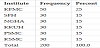
There were two types of questioners, first one is online for the physicians and the second one was hard copy to the patient/families. Two hundred physicians responded through online questioners 59% male versus 41% female (Table1), 73% Saudi compared to 27% non Saudi (Table 2). 52% were consultant, 24% fellows and 23% assistant consultant (table 3) Majority of the responders 19% were general pediatric, 14% were from Internal medicine,12% are emergency physician, 11% are pediatric intensive care physicians, 9% are pediatric cardiologists and ophthalmologists, 8% are neonatologists, 7% are general surgery, rest are pediatric surgery, nephrology, endocrinology and hematology are 3%, 2.5%, 2% and 1.5% respectively (Table 4). Encompassed physician of King Fahad Medical City (KFMC) 25% , while Security Forces Hospital (SFH), National Guard Health Affairs (NGHA), King Khalid University Hospital (KKUH), Prince Sultan Military College of Health Sciences (PSMC), and King Saud Medical City (KSMC) 15% for each center (Table 5).

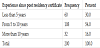
Accordingly, majority of the participating physicians had 5-10 years experience post residency certificate 54%, while 30% had experience less than 5 years, and 16% more than 10 years experience (Table 6). Lastly majority had post graduate training experience outside KSA 73% (Table 7).
In relation to family members that participated in this study most of them were had an academic educational level (48%), female (66%), Saudi (94%), with a relationship of others (59%).
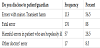
Results of analysis reveal that physicians disclose medical error to patients or their families depending on the type of error that was committed. The most disclosed type of medical error is fatal errors. That is, 88% of the participating physicians admitted to disclosing medical errors that are fatal. This is followed by medical errors with minor or transient harm according to 56.5% of the participating physicians. The next type of medical error that is likely to be disclosed by physicians to families is harmful errors in patients who are hopelessly ill at 28.5%. The least likely type of medical error to be disclosed by physicians to patients and their families is errors by other doctors which received a mere 8.5% (Table 8).
Further, the results indicate that there are several barriers to error disclosure among physicians. The most common barrier is concern that disclosure could result in a harmful reaction by patient/family (79%) followed by concern that the disclosure could result in a lawsuit (68.5%). The next significant barrier is in regard to a lack of formal training in error disclosure (44.5%). The least common barriers to error disclosure are fear that disclosure could harm patient (11%) and difficulty in admitting to personal failure (8.5%) (Table 9).

This research study also evaluated ways of disclosing medical errors by physicians using two scenarios. The first scenario entails the treatment of a patient with severe asthma with continuous Salbutamol Nebulization. By mistake the physician makes an order of 10 times the dose resulting in the patient arrest for 3 minutes due to Hypokalemia. The patient is resuscitated and is expected to make a full recovery. In this scenario majority of the participating physicians revealed that they would definitely disclose this error 57% followed by 36% would probably disclose this error (36%). Five percent of the participants admitted that they would disclose the error only if asked by patients/ parents. Two percent indicated that they will not disclose this error (Table 10).
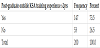
In case of explaining the error to patients/parents only 29.5% admitted that the child blood level of K+ went to low as a consequence of an error that took place, 66% explained the incident however without indicating the medical error that had taken place, whereas 4.5% did not indicate any occurrence of an error (Table 11).

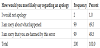
In relation to apology, most participants indicated they would demonstrate they are sorry by stating either “I’m sorry about what happened”, or “I’m so sorry that you were harmed by this error”49.5% for each. Those who asserted they will not apologize were 2% (Table 12).
The second scenario involved a patient that was admitted with left pleural effusion that was inserted by mistake and chest tube placed at the opposite side confirmed by x-ray. The results showed that 61.5% of physicians would definitely disclose this error. In addition, 31.5% would probably disclose this error, and 7% will disclose this error only if asked by the parent/patient (Table 13).

In regard to providing an explanation about what happened majority of the physicians indicated that they would explain what happened however without admitting to the occurrence of an error (62.5%), while there were those who would explain the incident and admitting to the occurrence of an error (34%). There were also those physicians who did not indicate an error nor admitting to one (3.5%) (Table 14).

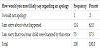
In relation to issuing an apology, many of the participants showed that they would apologize for the error by stating “I’m sorry about what happened” (62%) or “I’m so sorry that you/your child were harmed by this error” (37.5%). However, there are physicians who asserted they will not apologize for the error (0.5%) ( Table 15).
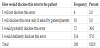
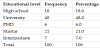
The results of this research also demonstrated parent/guardian reaction to medical error disclosure. There were 100 responders to the questioners, 66% were female relatives as. Saudi nationality account for 94%, most of the responders 48% University graduate, and 21% with Master degree, 18% post high school, 7% with PHD, and least 6% with intermediate certification (Table 16) Accordingly, the most common response that was given towards this was filing a complaint against the doctor to the administration of the hospital 57% followed by both complaining to a judicial official 41%, and politely asking the doctor what led to the complication and the reason for the error 41%. The other reaction is taking the issue to the media 25%. The least response demanding for an explanation by raising a voice to the doctor 21% (Table 17).

5. Discussion
The findings of this research indicate that physicians are not willing to disclose medical errors to patients or their families unless they are fatal. These findings are in line with those of Jones et al, who found that in many surveys, physicians, residents, and medical students all agreed that disclosure of major errors to patients is something that should be done. Despite this, less than half of those that were surveyed had disclosed a minor medical error to a patient [24]. Similarly, general acceptance of full disclosure of medical related errors can take place only in cases that involve adverse events which result in harm of the affected patient [25]. This is also in line with the findings of Al-Kaabba et al., that the main factor would influence physicians to disclose a medical error is the seriousness of the error [26]. Further, the most common barriers related to disclosing medical errors as identified in this study include: concern of disclosure resulting to a lawsuit, harmful reaction by the patient or their family, inadequate training regarding disclosure of medical errors, harm to the patient, and difficulty towards admitting to failure, this finding is in tandem to Moffat-Bruce et al, who explicate that physician do not disclose medical error due to the lack of favorable response to this disclosure, beside the financial risk associated with disclosing medical errors as a consequence of lawsuits further inhibit the likelihood of disclosure of medical errors. That is, there is worry over the cost of liability [27]. Further, most physicians revealing medical mistakes is a challenge because of the long history of feelings of reticent concerning disclosure of such information, and this challenge is also experienced as a consequence of physicians’ strong emotional reaction. This can be illustrated by the anxiety experienced in reaching a decision of disclosing medical errors [28]. Others pointed out that one of the difficulties that physicians face in the course of disclosing medical errors is the possibility for the patient may respond by demanding for cost reimbursement which will result in a legal process [29]. In incidents of medical errors that are fatal findings of this study indicate that doctors are not willing to admit to the error in the course of informing the patient or their family. However, they are quite likely to apologize for the incident without admitting to the medical error. Thus, physicians are not willing to disclose errors they have committed however they show some form of remorse by apologizing for incidents that came about as a consequence of the medical error. This is in line with the findings of Yürür et al., who postulate that when physicians do not admit to the occurrence of a medical error they thus fail to provide patients with all information necessary for their future medical decisions and treatments [30]. In regards the relative responders, although most of the responders are highly educated with University, Master and PHD but still their reaction to medical errors mostly with filing a complaint to the administration and judicial complaint which will put extra burden on physician and be barrier to disclose medical error.
6. Conclusion
This research was carried out to demonstrate the high prevalence of medical error among physicians, its impact on patients, and the significance of its disclosure to patients and their families. Accordingly findings of this research have shown that physicians have very willingness to disclose medical errors to patients. That is, they will mainly disclose these errors in the event that they are fatal. Further, in the course of explaining an adverse outcome as a consequence of medical error they do not admit to the occurrence of the error. Further, the findings of this study have demonstrated that physicians are however willing to apologize for occurrence of a medical error. The findings of this study are significant in that they confirm the problem of inadequate management of medical errors by physicians given the many failures associated with disclosure of these errors to patients and their families. The main barrier to error disclosure is the concern that disclosure could participate a lawsuit or harmful reaction by patient/ family. The fact that medical errors continue to be on the rise and their impact on the affected patients and health care system detrimental there is need to find better ways of handling this issue.
7. Recommendations
The following represents the key recommendations provided by this research study towards improving the cases as well as procedure of medical error disclosure by physicians. First, hospitals should develop and apply constructive strategy of medical error disclosure, this will be essential in enhancing transparency in this process.
Secondly, there should be establishment of standardized training concerning medical error disclosure. In particular, focus should be on informing patients and their families of the error that took place and its impact, and the doctors need to be sensitized on how to disclose medical errors. Significant focus is to be placed on the process of apologizing for the error. Also it is recommended that there should be more public education focusing on communication with health care providers in cases of medical error disclosure and how to deal with it. Many, patients and their families do not have an idea on the best wayof reacting to medical error disclosure as shown by this study. The final recommendation given in this research is restriction of media in relation to false propaganda on medical errors by physicians and their disclosure.
8. Ethics Approval
The research was approved by IRB Committee at King Fahad Medical City (IRB 17-227.)
Competing Interests
The authors declare that they have no competing interests.
Author Contributions
S. Al-Yousef and Ohood Al-Rehaili: Study conception and design,
drafting of manuscript, critical revision.
S. Al-Youse, Ohood Al-Rehaili and Haya AL-Johani: Data Acquisition,
analysis and interpretation.