



1. Introduction
Functional changes occurring in patients with Multiple Sclerosis (MS) measured by functional magnetic resonance imaging (fMRI) have been reported to be either adaptive, if correlated with a compensatory increase in behavioral performance or maladaptive, if paralleling a reduced efficiency [1].
Abnormalities of brain fMRI activation occur early in the disease course [2]: MS patients with absent [3] or mild cognitive disability [4] manifest greater recruitment of cortical areas during attention [5] and working memory [6] tasks, compared to healthy volunteers, suggesting that increased recruitment of brain areas might contribute to limiting the impact of MS related damage, being “adaptive or beneficial”. On the other hand, in patients with severe cognitive impairment, a reduced activation has been shown in comparison with less impaired ones [5] and a loss of the brain’s compensatory abilities due to disease worsening [5,7] has been postulated and considered to be “maladaptive”. The relation between brain activation and cognitive impairment could be expressed by an inverse u shape curve: whenever the brain pathology exceeds a threshold, the brain is considered no longer able to functionally compensate brain’s pathology [5], due to disease progression.
Furthermore, studies investigating resting state functional connectivity (RSFC) in MS, reported opposite patterns of connectivity in relation with severe cognitive impairment: i.e. a reduction of RSFC in the frontal lobes [8] or an increased FC [9] in impaired patients, It seems that thinking about functional reorganization processes as either “beneficial” or “maladaptive” when related to cognitive impairment as their underlying mechanisms are complex [10].
Studies investigating the functional basis of cognitive reserve (CR) at a functional level are lacking.CR is considered the sum of premorbid “cognitive enrichment” due to education, leisure and social activities, which is known to mitigate cognitive deterioration due to brain pathology [11], As shown in Alzheimer’s disease (AD) and in healthy adults, people with a high CR tend to withstand more agerelated changes and disease-related pathologies [12,13] than those with low CR.
Not only years of education, but also premorbid engagement in leisure activities might provide a synergic increment of the CR [12,14]. Thus, the CR construct was further finished by considering the influence of other enriching activities (i.e. reading books or newspapers, playing an instrument, social and physical activities), as part of the CR [11,15], effective in reducing progression of the cognitive decline also in healthy elderly individuals [16].
The protective role of CR on cognitive impairment has been shown in MS patients (Scarpazza et al. [17], Martins Da Silva et al. [18], see Sumowski et al. [19], for pre-morbid intelligence, Lezak, [20], for vocabulary knowledge, Ghaffar et al. [21] for occupational attainment and Sumowski et al. [22] for cognitive leisure).
Sumowski et al. [23] found in highly educated MS patients less deactivation of the default mode network (DMN) and less recruitment of prefrontal cortices compared to less educated ones, both at easy and at difficult n-back tasks, suggesting that in MS patients a high CR would reduce the expression of multiple sclerosis-related patterns of cerebral activity.
The current study aims to deeper investigate the functional correlates of CR and cognitive impairment in MS patients, by using an event related f MRI during a n-back task, known to be very sensitive in measuring information processing speed and working memory impairment, a typical deficit of MS patients. Our hypothesis was to positively correlate the degree of brain functional activation with cognitive deficit and inversely with cognitive reserve.
2. Methods
Twenty subjects (seven males and thirteen females, mean age: 51.15±8.1 years), with clinically definite MS [24], provided informed consent and participated in this study. The study was approved by the Ethic Committee of the Spedali Civili of Brescia and was conducted in accordance with the declaration of Helsinki. Ten patients were affected by the relapsing-remitting form; the others had a progressive course (3 with a primary progressive and 7 with a secondary progressive course). They had to be free of relapse in the previous year and able to perform the task in the fMRI equipment to be included. Exclusion criteria were dementia, (MMSE<24) and psychiatric disorders requiring medication. Their mean Expanded Disability Status Scale (EDSS [25], was 3.5 (SD±2.5). Their treatment was copolymer (n=2), interferon B (n=4) and with fingolimod (n=1). Thirteen sex, age and education matched healthy volunteers served as healthy controls (HC).
The Rao Brief Repeatable Battery in the Italian version (BRB, [26]) was used, including the Selective Reminding Test (SRT) which measures both the Long Term Storage (LTS) and the Consistent Long Term Retrieval (CLTR), the /36 Spatial Recall Test (SPART), the Symbol Digit Modality Test (SDMT), the Paced Auditory Serial Addition Task (PASAT) every 2” or 3” and the Word List Generation (WLG) with the Wisconsin Card Sorting Test (WCST, [27]), to investigate executive functions. WCST total errors (te) and perseverative errors (pe) were measured. The number of neuropsychological tests whose performance resulted below the normal range was recorded (“total number of impaired test” variable) for all the subjects.
A Cognitive Impairment Index (CII) was computed for each patient, in order to create a variable expressing the cognitive impairment severity, by summing each test’s “z score” score [28]. Since negative z scores indicate a worse performance, a smaller CII (i.e. the more negative is the score) indicates greater cognitive impairment.
Cognitive Reserve Index (CRI) was measured through the Cognitive Reserve Index Questionnaire (CRIq, [15]), including demographic data and education, working activity and leisure items. The total CRIq score is standardized and transposed onto a scale (mean = 100 and standard deviation= 15). The higher the CRIq score, the higher the estimated Cognitive Reserve.
The mean age of disease onset in our sample was high (41.5±9.7), thus decreasing the possibility that MS related difficulty influenced both education and occupational attainment. Moreover, the correlation between age at MS onset and years of education was not statistically significant (r=0.16, p=0.64), indicating that the disease had no impact on patients’ education. Finally, participants classified in two groups based on occupational attainment [29] indicated a balance across groups in the level of responsibility at work: 9/20 MS patients (45%) and 7/13 HC (53.8%) were in the high occupational attainment group (chi square=1.28, p=0.25).
Between-group analyses on socio demographic data, excluding gender and education, were performed using two independent sample t-test. Between-group analysis on gender and years of education used chi square test and Mann-Whitney test respectively (not normally distributed data: Kolmogorov-Smirmov d >.20). All the neuropsychological data were analyzed by means of non parametric statistics.
Spearman rank correlation coefficients as well as regression analyses were used to analyze the relationship between the CRI and the CII. Partial correlations between the CR and the CII, while controlling for EDSS and Structural MRI data were also calculated.
2.1 MRI examination
Paradigm: A n-back working memory task (15 stimuli/block; 2 blocks 1 or 2 back) was used in an event related fMRI. Subjects were required to recognize (by pressing a button) whenever a letter stimulus was the same as the one presented 1 or 2 back (task). The task block was alternated with a rest block as control (where subjects had to press a button in response to any appearing cross). Task performance was evaluated for each subject (= true positive responses plus true negative responses/ total number of occurred events).
fMRI acquisition: All scans were performed on a 1.5T MR unit (Avanto, Siemens, Erlangen, Germany), equipped with a dedicated 8-channel head coil (Invivo-Gainesville), using an integrated audio-video system (Eloquence, Invivo-Gainesville) connected to an external computer to allow the task synchronization. EPI T2- weighted sequence during n-back test (TR/TE: 2000/50ms, 23 slice, 4mm thickness, covering the whole brain, voxel size 3.5x3.5x3.5mm, with base resolution of 64x64) and anatomical high resolution 3 dimensional T1-weighted sequence for brain areas representation (TR/TE: 2050/2.53ms, TI 1100ms, 176 slices, 1mm thickness, voxel size 1x1x1mm, with base resolution of 256x256) were acquired.
fMRI data analysis: fMRI data were analyzed using Statistical Parametric Mapping (SPM8) software (Wellcome Department of Cognitive Neurology, Institute of Neurology, London), running on Matlab 8.3. For each subject, the first two volumes of the fMRI series were discarded to allow for T1 equilibration effects. Images were first corrected for slice timing and motion, then co registered with the 3D structural images, previously processed with the Brain Extraction Tool (BET) included in the FMRIB Software Library (FSL) to eliminate skull and scalp [30]. The 3D structural data of each subject were normalized to the MNI template (1x1x1mm) and the normalization matrix was subsequently transferred to the fMRI dataset. Finally, the normalized fMRI dataset was spatially smoothed using Gaussian kernel of 5 mm and analyzed using a random effect approach. General linear model was applied to contrast task with rest condition in each subject. Statistical significance level was set at 0.006 FWER corrected using cluster based thresholding (cluster size > 100 voxels) on a primary threshold of p<0.0001 [31]. Activations for MS and controls where compared.
For correlation with CRI and CII, the ROIs where a priori selected if present both in the activation map of pooled MS patients and HC and in the reported normative data of healthy subjects while performing the n-back task [32]. This ROIs selection procedure allowed to investigate the task effect in our sample, in regions consistently shown to be relevant for the task used.
A linear regression model was applied to assess the relationship between cortical activations, CRI (where CII was a nuisance variable) and CII (where CRI was a nuisance variable), using age, task performance and grey matter volume (in patients also EDSS, T2 lesion load), as other nuisance variables. Statistical significance level was set at 0.05 using cluster based correction, with cluster size > 30 voxels on a primary threshold of p < 0.001[31].
GM volume was measured by using the New Segment procedure implemented in SPM8 (http://www.fil.ion.ucl.ac.uk/spm), multiplying the number of the voxels underlying the GM partition for the voxel volume. White matter T2 lesions loads were automatically segmented and calculated using Analyze 11.0 (Analyzedirect, Overland Park, KS).
3. Results
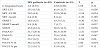
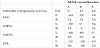
Socio-demographical and clinical results are reported in Table 1. Patients did not differ from HC in age, education and CRI score. As expected, patients were significantly worse than controls in the CII score. The neuropsychological performance of MS patients resulted to be significantly worse than controls both in the total number of impaired tests, and in LTS, CLTR, SPART, SDMT, PASAT 3”, PASAT 2”, WLG scores. Results are presented in Table 2.

A positive correlation between CRI and CII was found in pooled patients and HC (r=0.35, p=0.04), indicating that both in patients and in HC the lower the CRI the higher was the cognitive impairment. In MS group, multiple regression model showed a statistically significant association between CRI and CII, when also disease duration was considered as independent variable (F=3.70, r=0.55, p=0.04), suggesting that in MS patients both disease duration and CRI were the predictors of cognitive impairment. Furthermore, in MS patients a positive, although not significant, partial correlation between CRI and CII emerged when controlling also for GM volume and T2 lesion load (r=0.45, p=0.06), suggesting that CR could mitigate cognitive impairment in face of similar MRI disease burden.
3.1 fMRI results
A significantly worse score in task performance (1 back and 2 back) was noted in MS (mean accuracy 89.2% ± SD 10.4%) compared toHC (94.5%±3.8%) (t-test t= 2.48, p=0.02), with a positive correlation between task performance and CRI both in MS (r=0.62, p=0.003) and in HC (r=0.72, p=0.004), in MS also controlling for GM volume (r=0.52, p=0.02).
In pooled MS and HC, cortical fMRI activation was observed bilaterally in several frontal and parietal regions: the inferior frontal gyrus (IFG), the middle frontal and precentral gyri corresponding to the ventrolateral prefrontal cortex, the middle orbital gyrus (MOG), the premotor area (SMA), the middle cingulum (MCing), the inferior parietal lobule (IPL) and in small clusters of activation in the cerebellum, in the globus pallidus, in the left thalamus and in the right hippocampus. Results are presented in Table 3 and in Figure 1.


Activations were higher in MS compared to HC in all the above reported areas. (see Figure 1), with significant differences in the middle frontal gyrus, in the MOG bilaterally and in the left IFG (p<0.01).
Among these ROIs, the following were selected, since they were also reported in Owen et al. (2005) for regression analyses: the middle cingulate cortex (MCing, one cluster including right and left), right and left MFG, right and left MOG, right and left IFG and right and left IPL (Table 4).
A positive correlation between brain activation and CII was found in both MS and controls. In particular, in MS group in middle Cingulus bilaterally (r=0.78, t=4.16 as a single cluster), left IFG (r=0.76, t=3.91), right MFG (r=0.74, t=3.61), right IPL (r=0.76, t=3.84), as reported in Figure 2; in HC in the right IFG (r=0.92, t=6.37), right IPL (r=0.93, t=6.87) and left MOG (r=0.90, t=5.53), showing that the greater was the cognitive deficit the less was the brain activation, regardless the CR (and the clinical and radiological measures of disease severity for MS).

Conversely, a negative correlation between brain activation and CRI was found in MS in Middle Cingulum (r=0.90, t=7.04), left IFG (r=0.73, t=3.55) and right IPL (r=0.80, t=4.5). Results are shown in Figure 3. In control group, no significant correlation emerged. In other words, MS patients showed less brain activation with the increase of CR, regardless the cognitive impairment and both clinical and radiological indices of disease severity.

4. Discussion
The main result of this study is the opposite correlation found in MS patients, when functional brain activation was correlated to either CR or cognitive impairment, controlling for task performance and disease severity. We found less cortical activation in patients with higher CR (that is higher degree of education, greater cultural enrichment), regardless the severity of their cognitive impairment and of their clinical disability or brain pathology. On the other hand, in cognitively impaired MS patients, also greater cognitive impairment correlated with less brain activation and these two findings could seem contradictory. Traditionally, these data can be considered the manifestation of a greater cognitive efficiency, shown by MS patients with higher CR, who need to activate cortical areas at lesser extent during a given cognitive task, compared to those with less cognitive reserve (the correlation has not been found in controls, for which the protective effect of CR might not be evident as they do not have any brain pathology). On the other hand, a loss of functional compensation due to the progression of disease related cognitive impairment can be invoked, when a positive correlation with cognitive impairment (less activation, lower cognitive scores) is observed. In our opinion, these findings- which could seem prima facie paradoxical- could both be the expression of a different aspect of neuroplasticity in relation to cognitive efficiency. “Adaptive” interpretation [5] suggests that whenever compensatory brain hyper activation ceases, cognitive decline occurs and cognitive impairment becomes clinically evident. We can speculate that in the presence of high CR these “adaptive” mechanisms are probably not requested until pathology advances. Consistently with previous findings, we also found that the higher the CR index was, the less severe was the cognitive deficit when controlling for disease burden [17,19].
In our analysis, several methodological issues were observed: the correlation between each variable of interest (CRI and CII) and brain activation was performed independently from other confounding variables including CII and CRI respectively (allowing us to evaluate the separate effect of CRI and CII on activations), the possible effects of structural brain damage as well as of task performance were considered and finally a complete index of CR, including education, occupation as well as leisure activities, was employed.
Other studies on cerebral efficiency also suggested that less activation means better performance in many cases: i.e. improved language abilities after stroke correlates with reduced and only left sided cortical activation [33], faster finger tapping correlates with smaller cortical activation [34] and point to the hypothesis of a “better efficiency with smaller brain activation”. The same holds true with our findings of less cortical activations in patients with high CR.
Though, brain efficiency would be possibly degraded by neural pathology in MS, whose effects would be to modify brain functional reorganization of neural activity, supposed to increase to compensate brain pathology, which, if advanced, impedes these mechanisms to occur, leading to the worsening of cognitive symptoms [7].
Beyond the simple adaptive /maladaptive interprestation of neuroplasticity in relation to the degree of cognitive impairment, the meaning of increased brain activation needs to be discussed also in relation to cognitive rehabilitation trainings, which have been consistently shown to induce increased brain activations in task specific brain areas and circuits, that correlate with the improved cognitive ability which was trained [7,35] and persist beyond the end of the training [36]. According to these studies, increased brain activation would mean improved cognitive ability and greater “cerebral efficiency”. An alternative interpretation would be that training induced brain activation could only reflect a temporary mechanism of neuroplasticity. Only long term studies on trained and not trained individuals could be informative on the point.
The significance of increased or decreased activations in cortical areas of MS patients are still a matter of discussion between researchers and recently many authors [1,7] claimed for the needs of longitudinal studies in order to clarify the issue, as well as for the need of using more sophisticated functional imaging tools to monitor cognitive deficits, as graph analysis [1,37].
In conclusion, this paper provides evidence supporting the hypothesis that, in MS patients, CR might be expressed, at a functional level, by less task related brain activation, which in turn reflects neural efficiency. On the other hand, cognitive impairment could be the result of the breakdown of the functional compensatory mechanisms and could be reflected by a reduced cortical activation, as well. Therefore functional brain activations should be interpreted cautiously in relation with behavioral measures in patients and longitudinal studies on fMRI correlates of cognition will be useful in the future to this end.
Competing Interests
The authors declare that they have no competing interests.