



1. Introduction
People suffering from Alzheimer’s disease are often unable to take care of themselves or carry out normal day to day activities, let alone support their family and carry out social responsibilities. Dementia caused by Alzheimer’s disease [1] leads to patients’ unusual behaviors, aggression, agitation, forgetting, repetitive questions, culturally inappropriate behaviors, sexual disinhibition, and/or shadowing [2]. Most Saudi Alzheimer’s patients are cared for at home [3] by family members who act as caregivers to help patients have as normal a life as possible. The job of caregiving for a patient suffering from Alzheimer’s is not an easy one and it becomes more difficult when patients develop more problems with ADLs (Activities of Daily Living). Caregivers face challenges in the form of physical, economic and mental burdens. Some Alzheimer’s patients get agitated easily from simple things and even become violent. Alfakhri, et al.[4] mentions that handling agitation in patients is one of the most difficult parts of caregiving.
It is estimated that there are at least 50,000 senior citizens suffering from Alzheimer’s disease in the Kingdom of Saudi Arabia [3] and a Saudi citizen over the age of 85 has a 50% chance of being diagnosed with Alzheimer’s disease [5]. The family members who usually provide caregiving for these patients are usually motivated by cultural and religious beliefs [6]. Alqahtani, et al. [7] found that 70% of Saudi caregivers of Alzheimer’s patients experience some level of depression.
With the high prevalence of Alzheimer’s disease there and the dominance of family-based caregiving them, it is vital to investigate factors influencing how caregivers are affected. The Saudi Arabian government has been taking steps to raise awareness of Alzheimer’s disease and provide support facilities to enhance the quality of life for both patients and their families [5]. Khusaifan and El Keshky [8] have conducted a study investigating the role of social support as a mediating variable between depression and life satisfaction for those caregivers and found that social support was negatively correlated with depression among the caregivers and positively correlated with life satisfaction.
2. Caregiving to patients with Alzheimer’s disease
Dementia patients suffer from mental deterioration and physicians alone cannot ensure their proper care. Although daycare services, psychological counseling and support groups can provide help to Alzheimer’s patients, most Saudi Alzheimer’s patients are cared for at home by caregivers, usually family members and friends, who provide them with emotional and physical assistance, including support in daily life activities, sharing their pain, and helping them to feel comfortable, loved and valued [9-10]. This reflects what many researchers have found: caregiving involves physical, monetary and emotional support for to people in need by friends and family members to improve their quality of life [11]. Caregiving can be stressful and can cause depression [12-13]. Previous studies have shown that, along with some other factors, a caregiver’s socio-demographics play a vital role in the depression related to caregiving stress [4,14-18]. The amount of stress depends also on the support s/he receives from family members, friends and society.
De Fazio, et al. [19] and Levine [20] stated that caregivers who had to provide assistance for more activities and ADLs and had to face angry or aggressive behavior are more likely to be depressed. Other studies have shown that depression arising from caregiving may also depend on the caregiver’s gender, ethnicity, age, education, income, culture and geographic location [14]. Social institutions such as home care, day care, psychological counseling and support groups can help caregivers significantly and share the burden.
This study focuses on these socio-demographic factors influencing depression levels and life satisfaction among Saudi caregivers of Alzheimer’s patients.
3. Hypotheses
Two sets of hypotheses have been developed for this study.
To illustrate the relation between these socio-demographic factors and a caregiver’s depression level, the following hypotheses have been developed (H1-H8). A caregiver’s depression level depends on his/ her: gender (H1); economic status (H2); employment status (H3); age (H4); education (H5); marital status (H6); relation to patient (H7); hours spent caregiving per day (H8).
To illustrate the relation between the socio-demographic factors and a caregiver’s life satisfaction level, the following hypotheses have been developed (H9-H12). A caregiver’s life satisfaction depends on the support s/he receives from his/her: family (H9); friends (H10); significant other (H11); life satisfaction (H12).
4. Method
4.1 Participants
The study involved 154 caregivers over Alzheimer's disease patients in Saudi Arabia. The sampling method was completely random with participants' age ranging between 20-60 years. Male participants constituted 30% of the total sample. Participation of caregivers was completely voluntary. Anonymity was maintained by not recording the subjects' names. The confidentiality of collected personal demographic information was maintained.
4.2 Measures
4.2.1 Socio-demographic form
Demographic information collected from sample subjects includes gender, age, marital status, educational level, economic and employment status. In addition, the number of care giving hours per week and the relation to the patient were collected. The measuring scales used for determining caregivers’ social support, depressive symptoms, and general life satisfactions were as follows:
4.2.2 2nd Beck Depression Inventory Edition (BDI-II)
Participant depression level was assessed by the Beck Depression Inventory, Second Edition (BDI-II) [21]. BDI-II is a self-reporting tool that includes 21 items corresponding to symptoms of depression based on the Diagnostic and Statistical Manual of Mental Disorders criteria (DSM-IV). Items are self-rated based on a 4-point scale (0-3). Possible raw scores from the tool range between 0-63 and correspond to cut-point descriptive symptom classifications, including minimal, mild, moderate and severe.
4.2.3 Satisfaction With Life Scale (SWLS)
SWLS [22] was used to assess the individual’s global cognitive judgment of her/his life satisfaction. It includes 5 items based on a 7-point Likert scale. Total scores range from 5-35, with better life satisfaction indicated by higher scores.
4.2.4 The multidimensional scale of perceived social support (MSPSS)
MSPSS [23] was used to measure support perception. It includes 12 items equally divided among three subscales to evaluate support from family members, friends and significant other. A 7-point Likert scale is used in MSPSS ranging from 1 "very strongly disagree" to 7 "very strongly agree". Scores for each subscale range from 4-28, with the total score varying between 12-48. More perceived support is indicated by higher scores.
4.3 Data analysis
The data collected through questionnaires have been numerically coded and entered into SPSS (Statistical Package for the Social Sciences) and AMOS (an add-on module for SPSS). First of all, the data was checked for inconsistency, incompleteness or multiple answers. After rectification of the missing data and data entry errors, an Exploratory Factor Analysis (EFA) model was developed using SPSS. The EFA was observed to factor extraction. It was used the Kaiser-Meyer-Olkin score (KMO) that must be > 0.6 to be adequate for factor extraction [24].
The reliability analysis, indicated by Cronbach's Alpha score, was conducted to check the internal consistency of the items within each factor. The consistency among the item groups had to meet the minimum requirement of >0.6 to be satisfactorily [25]. Upon finding satisfactory results, a Structural Equation Model (SEM) was developed. SEM combines t tests, analysis of variance and multiple regressions. SEM is better suited for this study as the model expands beyond a simple X → Y and estimates relations between various constructs of the hypotheses [26].
The goodness-of-fit indices assessed in this study for evaluating model fit, following previous reports [27], were: The ratio of the chi square value to the degree of freedom, i.e., CMIN/DF (χ2/df), Incremental Fit Index (IFI), Tucker-Lewis index (TLI), Normed Fit Index (NFI), Comparative Fit Index (CFI), Root Mean Square Residual (RMR), Root Mean Square Error of Approximation (RMSEA), and the Goodness-of-Fit Index (GFI) [28] and the Adjusted Goodness of Fit Index(AGFI).The cutoff values of these indices for evaluating model fit were pre-specified in the computer program as previously reported [27,29]. The values of χ2/df < 3, < 5, and > 5 represent a good fit, a marginal fit and a poor fit respectively. For IFI, TLI, NFI CFI, GFI and AGFI, values typically range between 0 and 1, with 1 indicating perfect fit, the cutoff value of 0.90 is the most used to evaluate model fit [27]. If the value is <0.90, it is considered an unacceptable fit. Values of RMR and RMSEA, which do not range between 0-1, would indicate: ≤ 0.05 a ‘‘close fit’’, ≤ 0.08 a ‘‘reasonable fit’’, and > 0.10 ‘‘unacceptable fit’’ [30]. Values of PCLOSE ≥ 0.05 indicate also a good fit for RMSEA.
5. Result
5.1 Socio-demographic details
Out of 154 respondents, 108 (70%) were female and 46 (30%) were male. The sample had a fairly equal distribution of respondents in terms of age The respondents (%) had different ages and were organized into groups spanning ten years: 23.4%, for 20-30; 29.2% for 31-40; 22.1% for 41-50; 20.8%, for 51-60 and 4.5% for >60 years old. The 22.1% of the respondents completed less than high school, 8.4% completed high school and the remaining 69.5% completed college. 81% of the respondents were from middle income, or middle class and the remaining 19% from a wealthy, or the upper class. 51% of the respondents were employed; 61.7% were married; 13% were widowed/divorced and the remaining 25.3% were never married. The 3%, 35.7% and 26% of the respondents were spending <5 hours/ day, 5-10 hours/day, >10 hours/day in caregiving respectively. The 154 respondents, 60.4% were children of the person being cared for, 20.8% were grandchildren and 4.5% were spouses. The 45.5%, 33%, 13.6% and 7.8% respondents had family members <5, 5-7, 8-10 and >10 respectively.
5.2 Reliability analysis
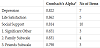
A reliability analysis was conducted to ensure that there is adequate internal consistency among the items for each construct. Table1 shows that the consistency was adequate (>0.6) among all items from different groups.
5.3 Exploratory factor analysis
Exploratory factor analysis has been conducted to extract the factors included in the model. 38 item covering factors such as depression, life satisfaction and social support. The analysis retained 7 items representing a measure of depression, 5 items for life satisfaction, and 10 items for social support. Table 2 shows the factor analysis (Kaiser- Meyer-Olkin, or KMO, scores) with associated p values. The loading strength for each item on the respective factors was determined using a maximum likelihood approach with Varimax rotation technique. The loading strength for each item on the respective factors, determined using a maximum likelihood approach with Varimax rotation technique, was adequate (Factor loading is illustrated in Appendix).

5.4 Factors influencing depression
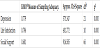
The independent effect of each caregiver’s socio-demographic factors on the depression level was analyzed and the summary is provided by Table 3. Therefore, the influence from other possible factors has not been considered here.

Table 3 shows that there are significant relationships between depression level and gender as well as between depression level and upper and middle classes, it being highest in male and upper class respectively. In addition, having or not employment does not have any influence on depression level. On the contrary, age has a significant effect on depression level. A post-hoc test revealed that participants who belong to the age category of 30-40 years experienced more depression than others (p<0.05). No significant relation was found between the measure of depression and socio-demographic factors such as caregivers’ education level, marital status, number of hours they spent caregiving per day and their relation to the patient (p>0.05).
5.5 Structural Equation Model
The use of SEM in Figure 1 shows the relations hypothesized in this study between three social support subscales (support from significant other, family and friends) and life satisfaction. Caregiver socio-demographic factors, such as education, age, gender, economic status and also the number of hours spent caregiving per day, have been controlled for in this model. As all these factors have been controlled for, the model is expected to illustrate a more accurate depiction of the influence of life satisfaction on caregivers’ depression levels.

5.6 Discussion on model fit indices
The ratio of the chi square value to the degree of freedom, i.e., CMIN/DF (χ2/df), is within the acceptable limit (1.597). GFI and AGFI achieved a good fit with a score of 0.956 and 0.9 respectively. CFI also attained a good fit (0.921), illustrating an adequate χ2-df ratio for the proposed model. Similarly, good fits have also been obtained for IFI (0.930). Although TLI (0.846) and NFI (0.833) did not reach an acceptable cutoff value (0.9), they were very close to it. Acceptable fits were also achieved for the RMR (0.059) and RMSEA (0.062) indices having this last one a reliable PCLOSE measure (>0.05). The model met all the applicable fit indices and therefore has been used to estimate the relations predicted in the conceptual design.
All three social support factors, i.e., significant other subscale (β=0.132, p<0.05), family subscale (β=0.209, p<0.05) and friend subscale (β=0.226, p<0.05), significantly influence life satisfaction. The positive coefficient value indicates that better social support improves life satisfaction. In addition, a caregiver’s life satisfaction has a significant influence (β=-0.405, p<0.05) on his/her depression level. A negative coefficient shows that better life satisfaction is likely to reduce depression in caregivers. Along with the number of hours spent in care giving, respondents’ socio-demographic factors, such as age, gender, education and economic status, have been controlled for in the model. Controlling for these factors enables the model to determine the influence of social factors on life satisfaction and the relation between life satisfaction and depression more accurately.
The hypotheses developed earlier were tested using the findings from ANOVA and SEM. Since hypotheses H1, H2 and H4 were not rejected, that means that caregiver’s depression level depends on his/her gender (H1); economic condition (H2) and age (H4). But, caregiver’s depression level does not depend on his/her employment status (H3), education (H5), marital status (H6), relation to patient (H7), and number of hours spent in caregiving everyday (H8) because hypotheses H3, H5-H8 were rejected.
Hypotheses H9-H12 were not rejected which establishes that caregiver’s life satisfaction depends on the support s/he receives from his/her family (H9), friends (H10), significant other (H11) and life satisfaction (H12).
6. Discussion
In this study, one way ANOVA and independent t tests have been conducted to analyze the effects of socio-demographic factors along with other variables on caregiver’s depression. Findings show that caregiver's gender, economic income and age are factors that can influence the level of depression arising from caregiving. In this sense, there have been reports with similar or different results.
Similar to Khusaifan and Keshky [8], we report here, that male caregivers were more vulnerable to depression than female caregivers. On the contrary, different reports indicated that female caregivers were more vulnerable to depression than males [14-16]. In addition, there was a neutral report conducted on Saudi participants that did not find any difference in depression levels for male and female caregivers [4]. One possible explanation is that in Saudi society, men generally have more opportunities to have leisure activities than women. Therefore, restraining free time due to caregiving could cause stress and with time depression more in males than females.
Janevic and Connell [17] and Schulz, et al. [18] found that caregivers who belong to a lower income group are more depressed, whereas this study found that higher income groups are more vulnerable to depression like Yurtsever, et al [30]. Alfakhri, et al. [4] found that financial obligations do influence the depression level. People with high economic status may have the possibility of hiring a formal trained caregiver to take care of an Alzheimer’s patient. Probably, if this valuable help is not required by the caregiver, it could be for religious, among other reasons. This self-restriction of free time may cause a high burden that may continue to depress.
This study achieved results similar to those of previous works [17,18,31], regarding the relation between age and caregiver’s depression level. Caregivers who were younger, especially participants who were 30-40 years old, seemed more vulnerable to depression than older participants. Perhaps the reason behind this is that most of the caregivers who fell into this age range were employed and this meant they had the additional burden of a job in their daily lives. Alfakhri, et al. [4] found that caregiver’s occupational status does influence depression levels. However, this study’s analysis did not reveal any significant relation between caregiver’s employment status and depression level. Another possible explanation is that in this age range the majority of people want to form his/her own family and caregiving tasks make it difficult to do that.
Other reports have indicated that education levels [14,17,31], number of hours spent in caregiving and relationship to the patient [17,31], and marital status [4] also influence caregivers’ depression levels. Nevertheless, no significant relation was found between these factors and caregivers’ depression level in this study.
It has been proposed that the difference among the previous factors, found in various reports including this one, could be due to variations in geographic location, ethnicity, available health care system, religion, culture, etc. [4,14,18,19].
Structural equation modeling shows that caregivers’ life satisfaction significantly influences his/her level of depression since stress can be reduced if the overall quality of life is better. Social factors such as support from family, friends and significant other also play a vital role as it does in other studies [9-11]. This is especially true for the significant other, i.e. wife/husband, incoping with stress from caregiving.
7. Conclusion
This study, focused on Saudi caregivers, showed that depression arising from caregiving to Alzheimer’s patients was significantly influenced by socio-demographic factors, specifically the gender, economic income and age of caregivers. The relationships between caregivers’ socio-demographics and depression level may vary due to, among others, geographic and ethnic differences. Another important point drawn from this study was that social support that may come from family members, friends, neighbors, and especially significant other can improve life satisfaction.
8. Limitations
There are several limitations in this study that must be acknowledged. The 154 samples had a 70%-30% gender ratio. The author considered the effect of gender as a socio-demographic factor but was careful not to assume equal variance during the independent t test. Although an 80-20% distribution in the economic status factor is very realistic, similar caution was taken during the t test with economic status and equal variance was not assumed. The sample size is not big enough for the SEM and therefore the outcomes cannot be generalized with a high level of confidence. The model could also be expanded by adding many other factors. There could be many small and large influences exerted by other factors which have not been considered. Influences and differences due to geographic locations and ethnic differences of the participants have not been considered. This study focused on one specific geographic location (Saudi Arabia). Therefore, generalization of the results is not recommended without further research.
Competing Interests
The author declare that there is no competing interests regarding the publication of this article.
Acknowledgments
This project was funded by the Deanship of Scientific Research (DSR), at King Abdulaziz University, Jeddah, under grant no. (G- 521 - 246 -39). The authors, therefore, acknowledge the DSR with thanks for their technical and financial support.